Cervical spine and thoraco lumbar injuries classification with good images
To draw
Cervical Spine & Thoracolumbar Injury Classification
PART 1: CERVICAL SPINE INJURIES
- Upper cervical spine (occiput - C1 - C2)
- Subaxial cervical spine (C3-C7)
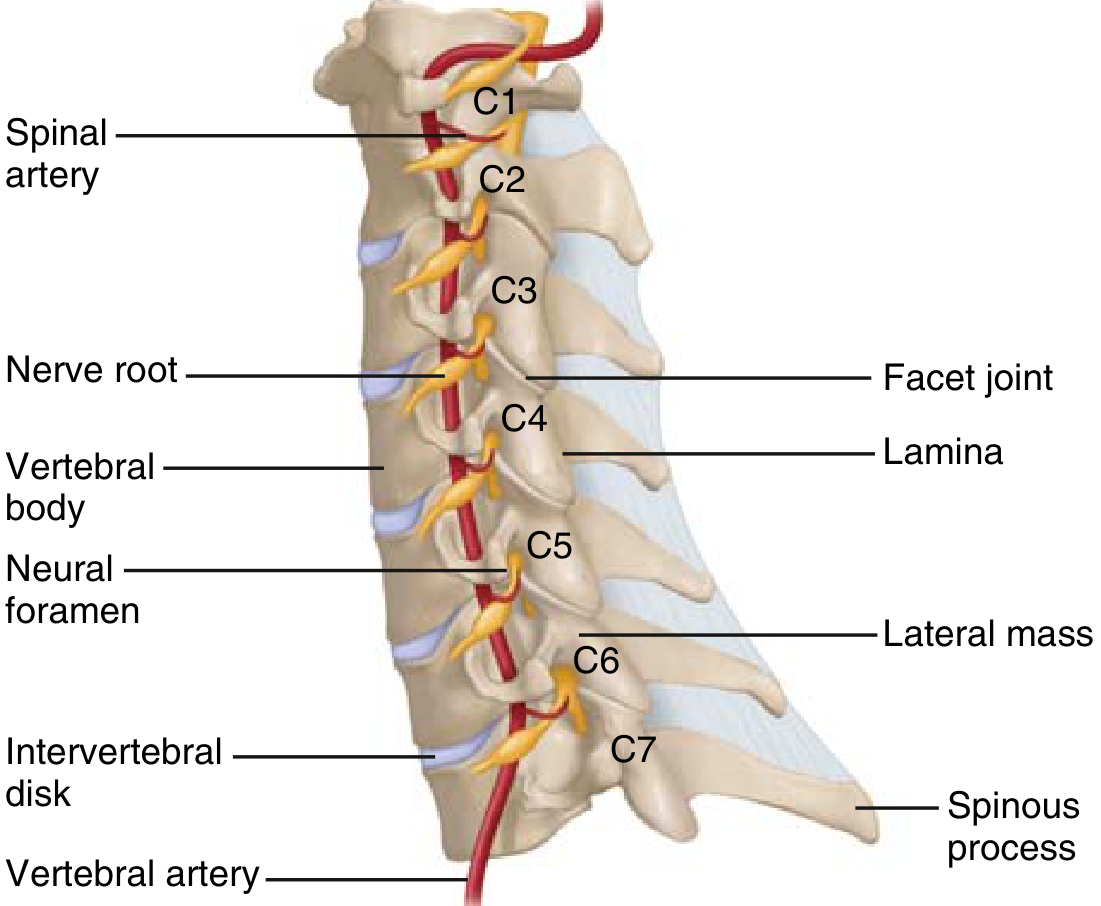
Cervical Spine Anatomy
A. Upper Cervical Spine (Occiput-C1-C2) Injuries
| Injury | Classification | Key Points |
|---|---|---|
| Occipital condyle fracture | Anderson & Montesano (Types I-III) | Type III (avulsion) most unstable |
| Atlanto-occipital dissociation | Traynelis (Types I-III) | Life-threatening; high cord injury |
| C1 (Atlas) fracture | Jefferson burst fracture; posterior arch fractures | Stable if transverse ligament intact |
| C1-C2 instability | Atlantodens interval (ADI) >3 mm adult, >5 mm child | Transverse ligament rupture |
| Odontoid (dens) fracture | Anderson & D'Alonzo classification | |
| - Type I | Tip avulsion | Stable, treat with collar |
| - Type II | Fracture at base of dens (most common) | Highest non-union rate; often surgical |
| - Type III | Extends into C2 body | Usually heals with immobilization |
| Hangman's fracture | Levine-Edwards classification | C2 pedicle fractures from hyperextension |
| - Type I | <3 mm displacement, no angulation | Stable; collar |
| - Type II | >3 mm displacement + angulation | Unstable; halo or surgery |
| - Type IIa | Severe angulation, minimal translation | Hyperflexion variant; traction contraindicated |
| - Type III | Facet dislocation + bilateral pedicle fracture | Most unstable; surgery |
B. Subaxial Cervical Spine (C3-C7) Classifications
1. Allen-Ferguson Classification (Mechanistic)
| Mechanism | Injury Stages | Key Example |
|---|---|---|
| Compressive-Flexion (CF) | CF1-CF5 | Teardrop fracture (CF5) - very unstable |
| Vertical Compression (VC) | VC1-VC3 | Burst fracture |
| Distractive-Flexion (DF) | DF1-DF4 | Bilateral facet dislocation (DF3-4) |
| Compressive-Extension (CE) | CE1-CE5 | Posterior element fractures |
| Distractive-Extension (DE) | DE1-DE2 | Extension injuries - hyperextension |
| Lateral-Flexion (LF) | LF1-LF2 | Asymmetric injuries |
2. SLIC System (Subaxial Cervical Injury Classification) - Treatment-Guiding
| Category | Descriptor | Points |
|---|---|---|
| Morphology | No abnormality | 0 |
| Compression | 1 | |
| Burst | 2 | |
| Distraction (facet perch, hyperextension) | 3 | |
| Rotation/translation (facet dislocation, teardrop) | 4 | |
| Discoligamentous Complex | Intact | 0 |
| Indeterminate (interspinous widening, MRI signal only) | 1 | |
| Disrupted (disc space widening, dislocation) | 2 | |
| Neurologic Status | Intact | 0 |
| Root injury | 1 | |
| Complete cord injury | 2 | |
| Incomplete cord injury | 3 | |
| Continuous cord compression (neurologic modifier) | +1 |
- Score ≤3 → Non-operative
- Score 4 → Indeterminate (surgeon discretion)
- Score ≥5 → Operative
3. AOSpine Subaxial Cervical Spine Injury Classification (Vaccaro et al.)
| Type | Description |
|---|---|
| Type A | Compression fracture - intact posterior tension band |
| Type B | Failure of anterior or posterior tension band - no misalignment |
| Type C | Translational/rotational injury with misalignment |
PART 2: THORACOLUMBAR INJURIES
Denis Three-Column Model (Foundation of All TL Classification)
| Column | Structures Included |
|---|---|
| Anterior | Anterior half of vertebral body/disc + ALL (anterior longitudinal ligament) |
| Middle | Posterior half of vertebral body/disc + PLL (posterior longitudinal ligament) |
| Posterior | Pedicles, facets, laminae, PLC (posterior ligamentous complex) |
Key principle: Injury extending into the middle column is largely considered unstable.
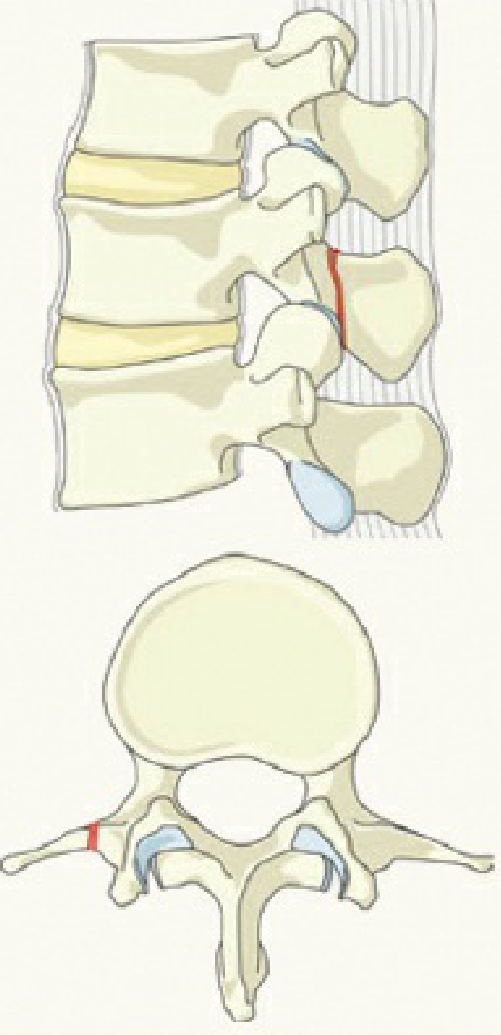
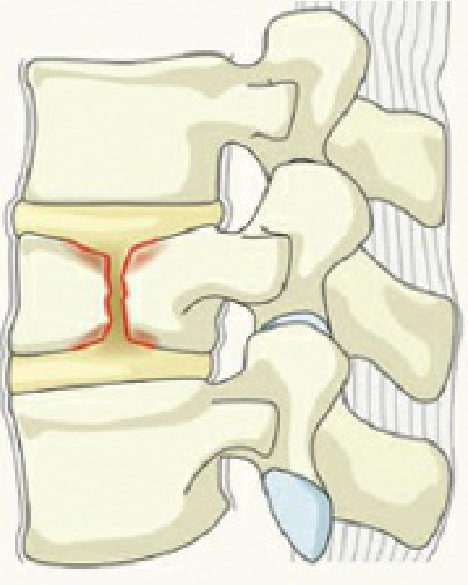
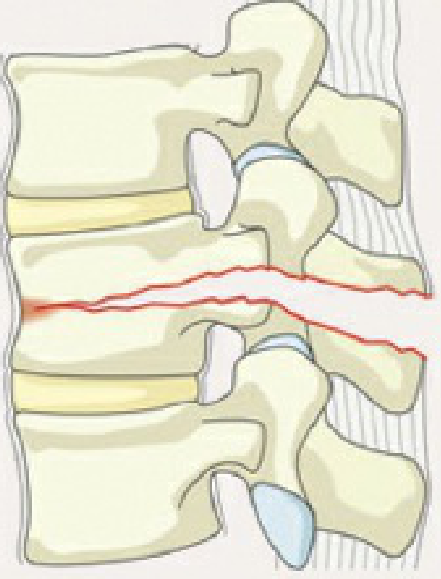
A. Denis Classification (4 Main Types)
| Type | Columns Involved | Stability | Neurologic Risk |
|---|---|---|---|
| Compression fracture | Anterior only | Stable | Low |
| Burst fracture | Anterior + middle (posterior may be involved) | Varies | Moderate-high |
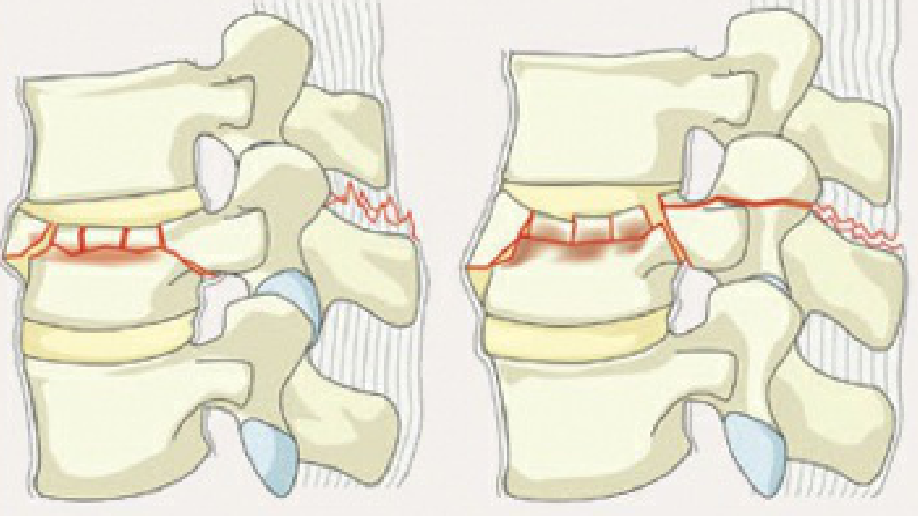
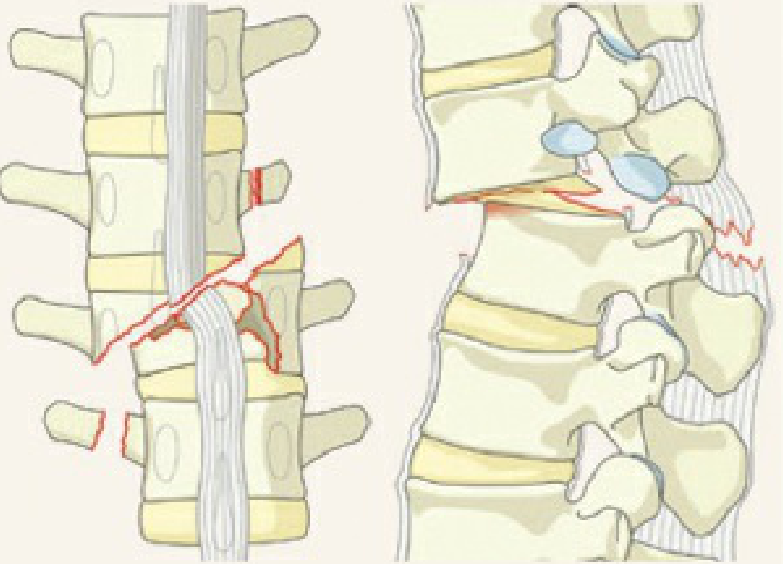
| Flexion-distraction (Chance) | Middle + posterior (tension failure) | Unstable | Variable |
| Fracture-dislocation | All three columns | Very unstable | Very high |
B. AO/Revised AOSpine Thoracolumbar Classification
Type A - Compression Injuries (Axial loading)

Type B - Distraction Injuries (Tension band failure without translation)

Type C - Translational/Displacement Injuries (Most unstable)
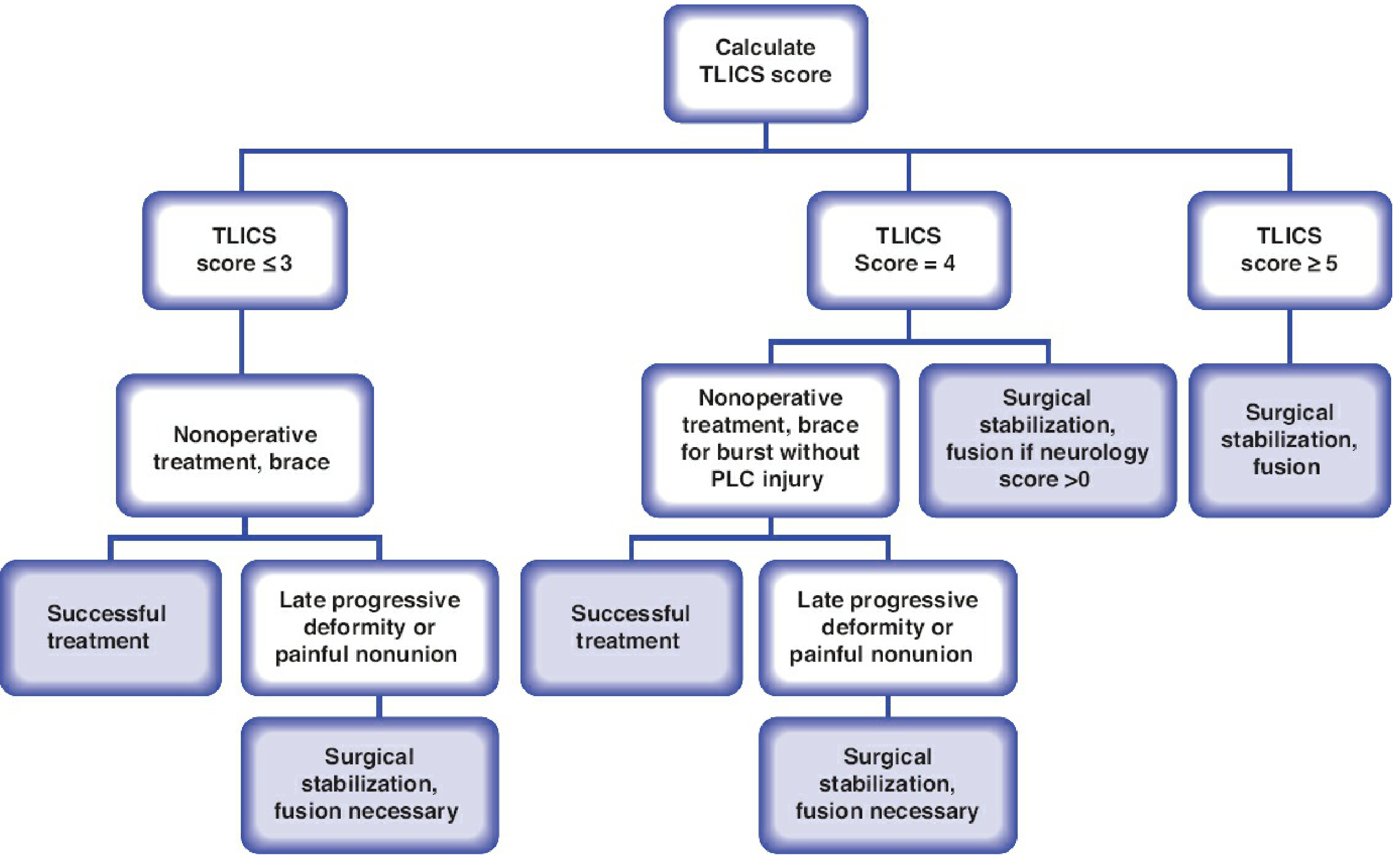
C. TLICS - Thoracolumbar Injury Classification and Severity Score
| Component | Qualifiers | Points |
|---|---|---|
| Injury Morphology | Compression | 1 |
| Burst | 1 | |
| Translational/Rotational | 3 | |
| Distraction | 4 | |
| Posterior Ligamentous Complex (PLC) | Intact | 0 |
| Suspected/indeterminate | 2 | |
| Injured | 3 | |
| Neurologic Status | Intact | 0 |
| Nerve root injury | 2 | |
| Complete cord/conus | 2 | |
| Incomplete cord/conus | 3 | |
| Cauda equina injury | 3 |
- <4 points → Non-operative (brace)
- 4 points → Indeterminate
- >4 points → Operative
TLICS Treatment Algorithm
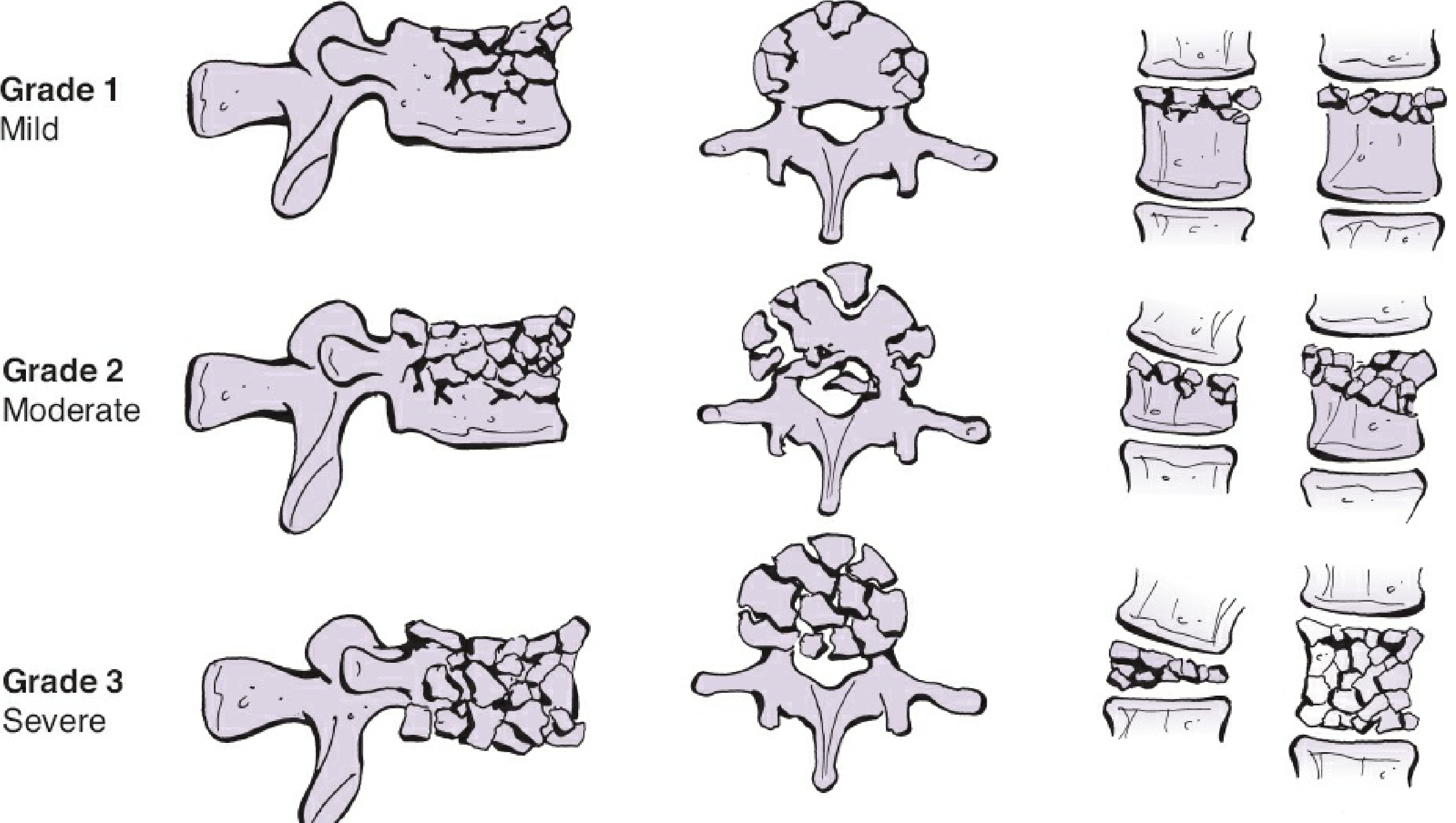
D. Load-Sharing Classification (McCormack)
- Comminution of vertebral body
- Apposition of bony fragments
- Kyphosis correction needed
Load-Sharing Grades - Burst Fracture Severity
Summary Comparison
| Feature | SLIC (Cervical) | TLICS (TL) | AOSpine TL |
|---|---|---|---|
| Region | C3-C7 | T1-L5 | T1-L5 |
| Key domains | Morphology, DLC, Neurology | Morphology, PLC, Neurology | Morphology (A/B/C) |
| Surgical threshold | ≥5 | ≥5 | Type C nearly always; B2 often |
| Main strength | Treatment algorithm | Treatment algorithm | Fracture description/communication |
| Main weakness | Complex; moderate agreement | Requires reliable neuro exam | Less direct treatment guidance |
Sciwora pg 10 mark answer
SCIWORA spinal cord injury without radiographic abnormality exam MCQ 10 marks
SCIWORA (Spinal Cord Injury Without Radiographic Abnormality)
Definition
With modern MRI, the definition has been revised - SCIWORA now specifically refers to normal X-ray and CT (MRI may still show cord signal changes, disc pathology, or complete cord disruption). Cases with positive MRI findings are still classified as SCIWORA by current convention.
Incidence
- Incidence among pediatric trauma patients: 0.15% to 0.2%
- Comprises 4.5% to 35% of all pediatric spinal injuries
- In children 1-17 years: 34.8% of traumatic myelopathy cases
- Presents almost exclusively in children (rare in adults)
Why Children Are Predisposed (Pathophysiology)
| Feature | Effect |
|---|---|
| Proportionally larger head | Creates higher fulcrum (C2-C3 in children vs. C5-C6 in adults); transmits greater force to upper cervical cord |
| Ligamentous laxity | Allows significant vertebral displacement without permanent bony malalignment - spine "springs back" |
| Expandable intervertebral discs | Absorb and transmit forces without fracture |
| Horizontal, shallow facet joints | Permit anterior-posterior slipping without dislocation |
| Weak paravertebral muscles | Less dynamic muscular protection |
| Anterior wedging of vertebrae | Increases susceptibility to flexion injury |
| Ossification centers and synchondroses | Fracture at weak bony points without apparent dislocation |
In children <8 years, injury is at upper cervical spine (C1-C4). After age 9, as head-to-body ratio decreases and neck muscles strengthen, injury shifts to lower cervical spine (C5-C7), similar to adults.
Mechanisms of Spinal Cord Injury in SCIWORA
- Cord contusion - transient compression/distraction during hyperflexion or hyperextension
- Ischaemia - temporary vertebral artery occlusion causing cord infarction
- Transient disc herniation - momentary disc bulge compressing cord, spontaneously reducing
- Ligamentous microtearing - cord traction during momentary distraction
- Motor vehicle crashes (most common)
- Falls
- Sports injuries / diving (teenagers)
- Child abuse - shaking mechanism in infants
Clinical Features
- Transient paraesthesia, numbness, or limb weakness (may be only initial symptom)
- Partial or complete myelopathy - motor/sensory loss below level of injury
- Bowel and bladder dysfunction
- Delayed onset - neurological deficit may appear hours after injury ("latent SCIWORA")
- Presentation ranges from transient tingling to complete cord injury (ASIA A)
Diagnosis
Imaging Protocol
| Modality | Finding in SCIWORA | Role |
|---|---|---|
| X-ray | Normal - no fracture, no malalignment | Initial screening |
| CT scan | Normal - no bony injury | Confirms no fracture/dislocation |
| MRI | Variable - may show cord edema, hemorrhage, contusion, disc herniation, or be normal | Investigation of choice |
MRI is mandatory in any child with:
- Objective neurological deficit after trauma
- History of transient limb paraesthesia or paralysis
- Persistent neck pain after normal X-ray/CT
- Normal (best prognosis)
- Cord edema (intermediate prognosis)
- Cord hemorrhage / contusion (poor prognosis)
- Complete cord disruption (worst prognosis)
Differential Diagnosis
- Transverse myelitis
- Multiple sclerosis (first episode)
- Acute disc prolapse with cord compression
- Epidural hematoma
- Spinal cord ischemia / watershed infarction
- Conversion disorder (diagnosis of exclusion)
- Ligamentous instability without bony injury
Treatment
- Cervical spine immobilization - immediately with blocks, tapes or cervical collar pending MRI
- MRI - urgent; defines cord injury and guides further management
- Bracing / immobilization - up to 12 weeks recommended (to allow ligament healing and prevent recurrent injury)
- Neurosurgical consultation - if MRI shows cord compression from disc herniation or epidural hematoma (surgical decompression may be needed)
- ICU monitoring - for cardiovascular and respiratory management (high cervical injuries cause hypotension and bradycardia from sympathetic disruption)
- Avoid traction in suspected hyperflexion-hyperextension variants
Prognosis
- Normal MRI → best prognosis; most make full recovery
- Cord edema only → variable; partial recovery likely
- Cord hemorrhage / disruption → poor prognosis; permanent deficits
- Latent onset cases (deficit appearing hours post-injury) may have better outcome than immediate complete injury
- Overall better prognosis in SCIWORA than in adult SCI with bony injury, due to the incomplete nature of many injuries
Key Examination Points
| Point | Fact |
|---|---|
| Coined by | Pang and Wilberger, 1982 |
| Imaging | Normal X-ray + Normal CT = SCIWORA; MRI may be abnormal |
| Most common site | Cervical spine |
| Age <8 years | Upper cervical (C1-C4) |
| Age >9 years | Lower cervical (C5-C7) |
| Investigation of choice | MRI spine |
| Treatment | Immobilization + MRI; bracing up to 12 weeks |
| Prognosis marker | MRI signal change |
| Incidence in peds spine injury | 4.5% to 35% |
Include flow chart and images for above and generate new one
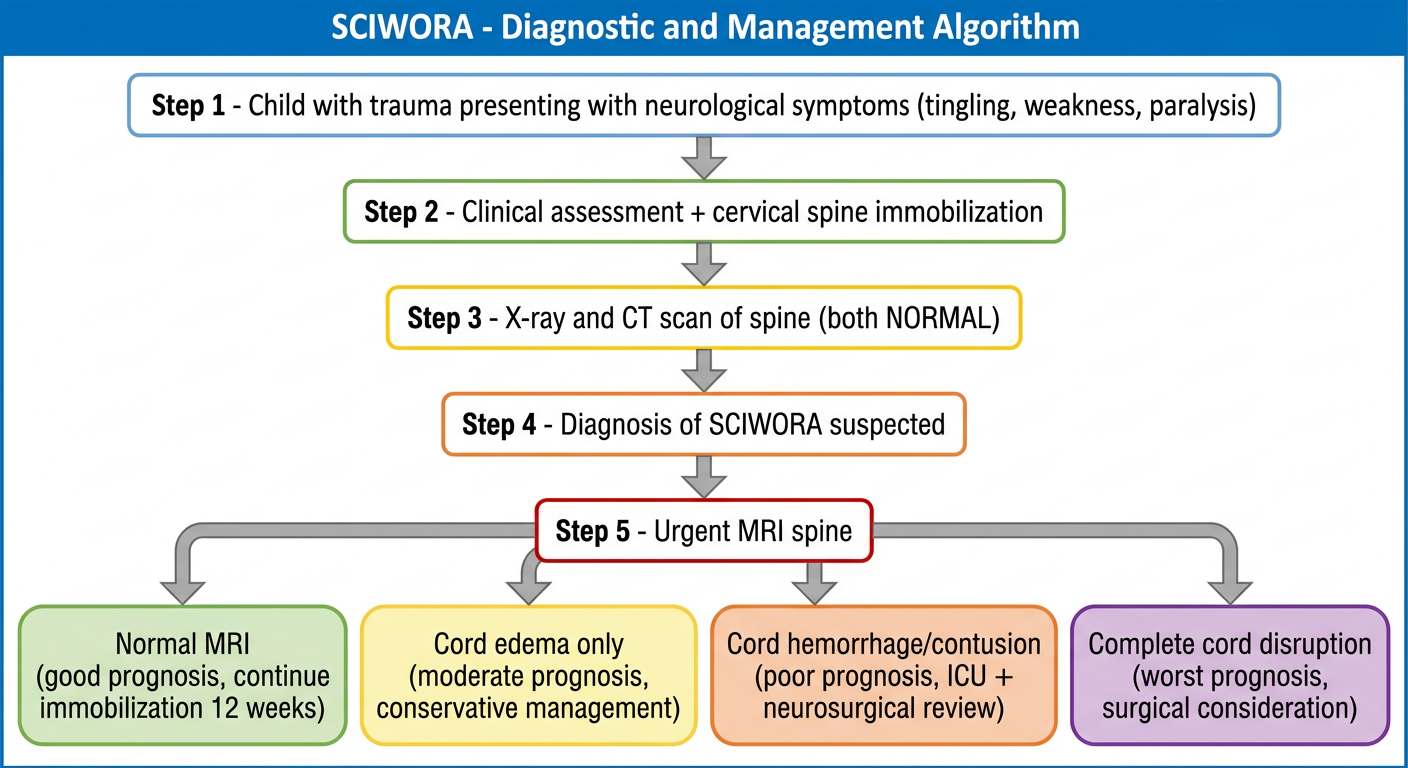
Medical flowchart titled "SCIWORA - Diagnostic and Management Algorithm" showing: Step 1 - Child with trauma presenting with neurological symptoms (tingling, weakness, paralysis); Step 2 - Clinical assessment + cervical spine immobilization; Step 3 - X-ray and CT scan of spine (both NORMAL); Step 4 - Diagnosis of SCIWORA suspected; Step 5 - Urgent MRI spine; branching into 4 MRI outcome paths: Normal MRI (good prognosis, continue immobilization 12 weeks), Cord edema only (moderate prognosis, conservative management), Cord hemorrhage/contusion (poor prognosis, ICU + neurosurgical review), Complete cord disruption (worst prognosis, surgical consideration). Clean clinical flowchart style with color coding.
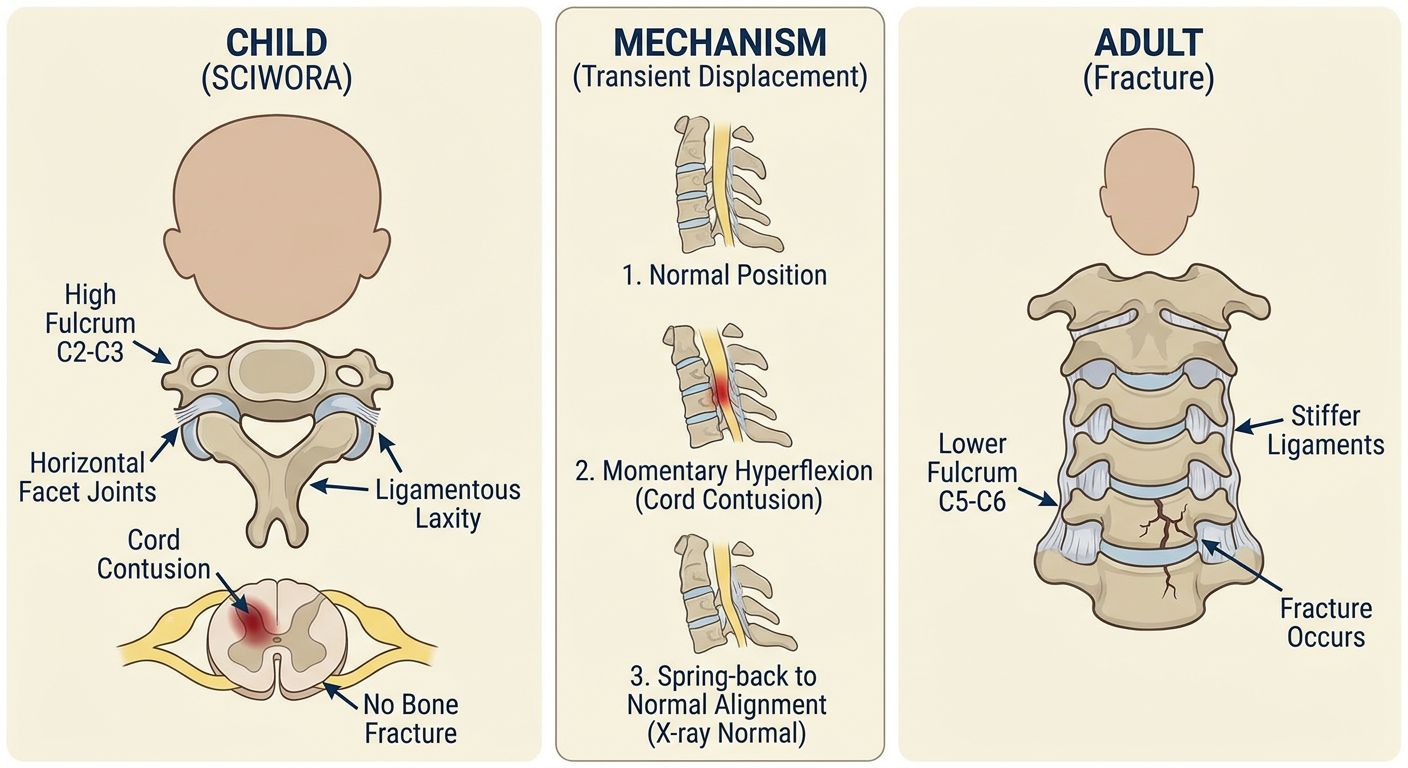
Medical educational illustration showing SCIWORA (Spinal Cord Injury Without Radiographic Abnormality) pathophysiology in children vs adults. Left panel shows child spine anatomy: large head causing high fulcrum at C2-C3, horizontal shallow facet joints, ligamentous laxity allowing temporary displacement then spontaneous reduction, cord contusion without bone fracture. Right panel shows the same mechanism in adult (lower fulcrum at C5-C6, stiffer ligaments, fracture occurs with injury). Central panel shows spine in 3 stages: normal position, momentary hyperflexion with cord contusion, then spring-back to normal alignment explaining why X-ray appears normal. Labeled anatomical diagram style, medical textbook quality.
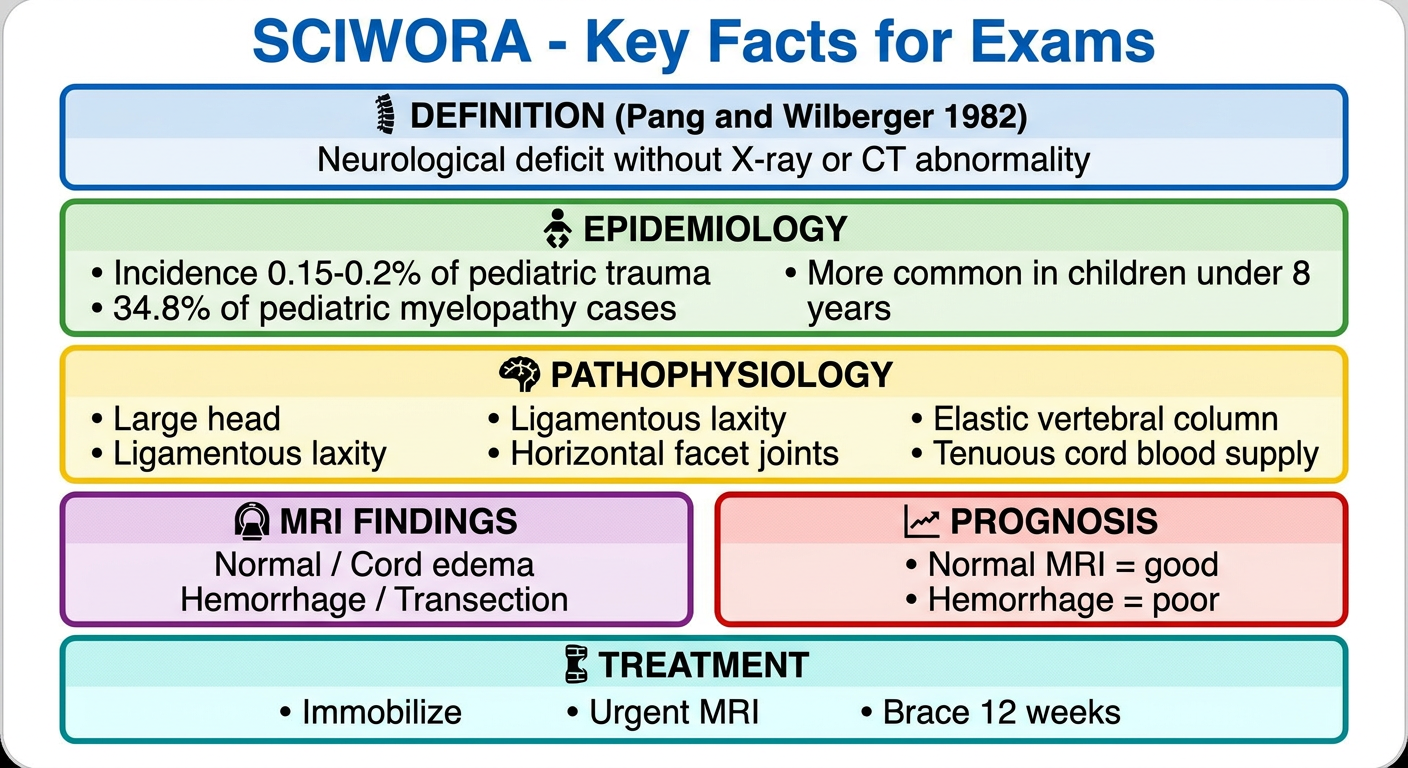
Medical educational poster titled "SCIWORA - Key Facts for Exams" with the following sections arranged in a clean grid layout: Top box - Definition by Pang and Wilberger 1982: neurological deficit without X-ray or CT abnormality. Second row: Epidemiology box showing incidence 0.15-0.2% of pediatric trauma, 34.8% of pediatric myelopathy cases, more common in children under 8 years. Third row: Pathophysiology box with bullet points - large head, ligamentous laxity, horizontal facet joints, elastic vertebral column, tenuous cord blood supply. Fourth row: two boxes - MRI findings (normal / cord edema / hemorrhage / transection) and Prognosis (normal MRI = good, hemorrhage = poor). Bottom row: Treatment box - immobilize, urgent MRI, brace 12 weeks. Color coded sections, professional medical study card style.
SCIWORA - Spinal Cord Injury Without Radiographic Abnormality
(10 Mark Answer)
1. Definition
- Originally coined by Pang and Wilberger in 1982 (before the MRI era)
- Modern definition: Normal X-ray + Normal CT = SCIWORA (MRI may still show cord signal changes)
- Excludes: penetrating trauma, electric shock, obstetric complications, congenital spinal abnormalities
The cord is injured because the vertebral column is more elastic than the spinal cord - it springs back to normal position after momentary displacement, leaving no radiographic trace but causing cord injury.
2. Why it Happens - Pathophysiology in Children
| Anatomical Feature | Why it Predisposes to SCIWORA |
|---|---|
| Large head-to-body ratio | Creates fulcrum at C2-C3 (vs C5-C6 in adults); greater force transmitted to upper cord |
| Ligamentous laxity | Allows large vertebral displacement without permanent malalignment - "springs back" |
| Horizontal shallow facet joints | Permits anterior-posterior slipping without dislocation |
| Elastic vertebral column | Absorbs and transmits forces without fracture |
| Tenuous spinal cord blood supply | Cord ischaemia from temporary vertebral artery occlusion |
| Weak paravertebral muscles | Less dynamic muscular protection |
| Anterior wedging of vertebrae | Increases flexion injury susceptibility |
3. Epidemiology
- Incidence: 0.15% to 0.2% of all pediatric trauma patients
- Comprises 4.5% to 35% of pediatric spinal injuries
- 34.8% of traumatic myelopathy in children aged 1-17 years
- Almost exclusively in children (rare in adults due to stiffer spine)
- Boys > Girls
- Most common mechanism: Motor vehicle crash > Falls > Sports/Diving
- Children < 8 years → Upper cervical (C1-C4) - due to large head / high fulcrum
- Children > 9 years → Lower cervical (C5-C7) - fulcrum descends as head-body ratio normalizes
4. Clinical Features
- Transient paraesthesia / numbness / weakness (may be only symptom initially)
- Myelopathy - motor and sensory loss below injury level
- Bowel and bladder dysfunction
- "Latent SCIWORA" - deficit appearing hours after injury (beware delayed presentation)
- Spectrum from mild tingling to complete cord injury (ASIA A)
5. Diagnosis
Imaging Protocol
| Modality | SCIWORA Finding | Role |
|---|---|---|
| X-ray | NORMAL - no fracture, no malalignment | First-line screening |
| CT scan | NORMAL - no bony injury confirmed | Confirms no fracture/dislocation |
| MRI | Variable - may be normal OR show pathology | Investigation of choice - mandatory |
- Normal - best prognosis; full recovery expected
- Cord edema only - intermediate prognosis; partial recovery
- Cord contusion / hemorrhage - poor prognosis; permanent deficits likely
- Complete cord transection - worst prognosis; no recovery
MRI should be obtained in any child with:
- Objective neurological deficit after trauma
- History of transient limb numbness or paralysis
- Persistent neck pain after normal X-ray/CT
6. Diagnostic and Management Flowchart (Generated)
7. Treatment
- Immediate cervical spine immobilization - blocks, tapes, cervical collar (never remove until MRI done)
- Urgent MRI spine - defines injury, guides management, provides prognosis
- Bracing / immobilization for up to 12 weeks (ligament healing and prevention of recurrent injury)
- ICU monitoring for high cervical injuries:
- Cardiovascular: hypotension (vasopressors), bradycardia (atropine)
- Respiratory: ventilatory support if needed
- Neurosurgical review if MRI shows surgical pathology (disc herniation, epidural hematoma)
- Do NOT apply traction in hyperflexion-hyperextension variants
- Special spinal board for children: elevate torso 2-3 cm to compensate for large head and maintain inline cervical alignment
8. Prognosis
| MRI Finding | Prognosis |
|---|---|
| Normal MRI | Best - full recovery expected |
| Cord edema only | Moderate - partial recovery |
| Cord hemorrhage | Poor - permanent deficits |
| Complete disruption | Worst - no recovery |
9. Quick-Reference Summary Card (Generated)
10. Key Exam Points (One-Liners)
| Question | Answer |
|---|---|
| Who coined SCIWORA? | Pang and Wilberger, 1982 |
| What does SCIWORA mean? | SCI with normal X-ray and CT |
| Is MRI normal in SCIWORA? | Not always - may show cord edema/hemorrhage |
| Most common age group? | Children < 8 years (upper cervical) |
| Most common site? | Cervical spine |
| Investigation of choice? | MRI spine |
| Duration of bracing? | 12 weeks |
| Prognosis marker? | MRI signal change |
| Why more common in children? | Ligamentous laxity + large head + elastic column + tenuous cord supply |
| What is "latent SCIWORA"? | Neurological deficit appearing hours after the initial injury |