Um, I'm going to study acute lymphoblastic leukemia from, uh, Robbins. I want you to give me something to read before I start it, uh, so that I can understand it while reading it.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have everything I need. Here is your pre-reading primer on ALL before you open Robbins:
Pre-Reading Primer: Acute Lymphoblastic Leukemia/Lymphoma (ALL)
This is a conceptual roadmap so that every sentence in Robbins lands with meaning rather than just memorized text.
1. The Big Picture: What Is ALL?
ALL is a cancer of immature lymphoid cells - specifically lymphoblasts that are "frozen" at an early stage of development and can no longer mature. Because they are blocked from maturing, they accumulate in enormous numbers and crowd out the normal bone marrow.
The word "leukemia" means the immature cells flood into the blood. The word "lymphoma" means they form a solid mass (like in the thymus). ALL can be either or both - hence "leukemia/lymphoma." This dual nomenclature is something Robbins uses consistently for lymphoid tumors, and it simply means the same disease can present differently depending on where the cells pile up.
2. Two Flavors: B-ALL vs. T-ALL
To understand ALL, you first need to know where B and T cells come from. Here is the diagram from Robbins itself (Fig. 13.5), which is the single most important image to have in your head before reading:
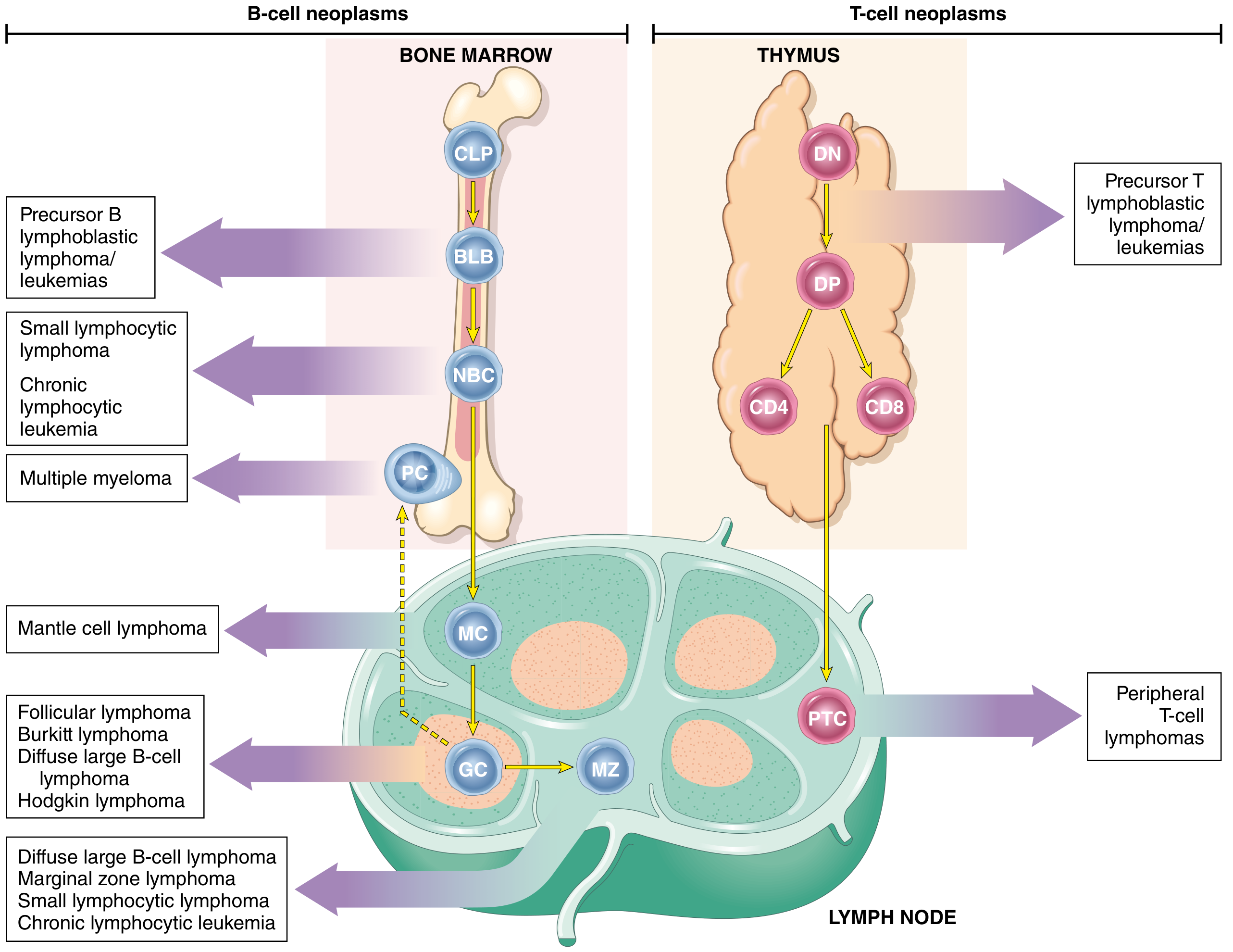
Fig. 13.5, Robbins: The stage at which normal lymphocyte development is "arrested" determines the type of lymphoid tumor.
B-ALL (~85% of all ALL cases):
- Cell of origin: pre-B lymphoblast in the bone marrow
- Peak age: ~3 years (because pre-B cells are most numerous in early childhood)
- Presentation: classic leukemia (pancytopenia, blasts in marrow/blood)
T-ALL (~15% of cases):
- Cell of origin: precursor T cell in the thymus
- Peak age: adolescent males
- Presentation: anterior mediastinal (thymic) mass, ± leukemic picture
Both share the same underlying logic: a block in differentiation + uncontrolled proliferation.
3. Why Does the Block in Differentiation Happen? (Pathogenesis in Plain Language)
Normal B and T cells require specific transcription factors (master switches) to mature. In ALL, these master switches are disrupted by chromosomal mutations. When you lose the ability to differentiate, cells stay stuck as blasts.
Key mutations to know before reading Robbins:
| Subtype | Mutation | What it disrupts |
|---|---|---|
| B-ALL (most common) | t(12;21) - ETV6::RUNX1 | Transcription factors for B-cell maturation |
| B-ALL (adult / bad prognosis) | t(9;22) - BCR::ABL1 (Philadelphia chromosome) | Tyrosine kinase - makes cells grow uncontrollably |
| B-ALL | PAX5, TCF3, KMT2A mutations | Various transcription factors |
| T-ALL | NOTCH1 mutations (50-70%) | Key switch for T-cell development |
The Philadelphia chromosome (t(9;22)) deserves special attention. In ALL it produces a 190 kDa BCR-ABL protein (stronger kinase than the 210 kDa form in CML). This is directly targetable with tyrosine kinase inhibitors (e.g., imatinib), and Robbins will discuss this as a major therapeutic advance. When you read about "Ph+ ALL," this is what it means.
The core concept: fewer than 10 total driver mutations are enough to produce full-blown ALL. The transcription factor mutation does the "differentiation block," while complementary mutations (like RAS signaling or tyrosine kinase activation) drive the proliferation.
4. What Happens to the Patient? (Clinical Logic)
Once you understand the mechanism, the symptoms make perfect sense:
Bone marrow failure - Blasts crowd out normal precursors:
- Anemia (low RBCs) → fatigue, pallor
- Thrombocytopenia (low platelets) → easy bruising, bleeding
- Neutropenia (low neutrophils) → infections
Mass effects - Blasts accumulate in organs:
- Lymphadenopathy, splenomegaly, hepatomegaly
- T-ALL specifically: anterior mediastinal mass (may compress airways - a pediatric emergency)
- Bone pain (marrow expansion)
- CNS involvement - lymphoblasts can infiltrate meninges (this is why CNS prophylaxis/treatment matters)
5. Key Concepts Table from Robbins (Memorize This Logic)
| Feature | B-ALL | T-ALL |
|---|---|---|
| % of ALL | ~85% | ~15% |
| Typical patient | Child <15 yrs | Adolescent male |
| Cell of origin | Pre-B (bone marrow) | Pre-T (thymus) |
| Classic mutation | t(12;21) ETV6::RUNX1 | NOTCH1 mutation |
| Key targetable mutation | BCR::ABL1 (Ph+) | - |
| Typical presentation | Leukemia (marrow/blood) | Thymic mass ± leukemia |
| Prognosis | Generally good in children | Aggressive |
6. Three Concepts That Will Make Robbins Click
A. "Maturation arrest" is the universal theme. Every lymphoid neoplasm in Robbins can be understood by asking: at what stage of development did the cell get stuck? B-ALL = stuck at pre-B stage. T-ALL = stuck at pre-T stage. This same logic applies to CLL, follicular lymphoma, plasma cell myeloma, etc.
B. The leukemia vs. lymphoma distinction is clinical, not biological. The same transformed clone can behave as leukemia (blood/marrow dominant) or lymphoma (mass dominant) based on its traffic patterns. ALL and lymphoblastic lymphoma are the same disease; the distinction is made by whether >25% of marrow is involved.
C. Genetics drive prognosis and treatment. In ALL, cytogenetics and molecular markers are not just academic - they directly determine treatment intensity and which targeted drugs to add. When Robbins discusses chromosomal translocations, connect each one to its prognostic implication.
7. Vocabulary to Know
- Lymphoblast: an immature lymphoid precursor - this is the tumor cell in ALL
- TdT (terminal deoxynucleotidyl transferase): an enzyme expressed only in precursor lymphoid cells; its positivity on immunohistochemistry is the hallmark marker of ALL (distinguishes it from AML)
- CD10 (CALLA): common ALL antigen, expressed on most B-ALLs; useful immunophenotypic marker
- CD19, CD20: B-cell antigens; expressed in B-ALL (CD19 is targeted by CAR-T cell therapy)
- CD3, CD7: T-cell markers; expressed in T-ALL
- Hyperdiploidy vs. hypodiploidy: having extra chromosomes (>50) = good prognosis in B-ALL; having fewer chromosomes = poor prognosis
- CAR-T cells: chimeric antigen receptor T cells directed at CD19 - Robbins mentions this as a major therapeutic advance with impressive responses but significant toxicity and cost
8. How Robbins Structures the Chapter
When you open the chapter, you will see it flows as:
- Definition and epidemiology
- Pathogenesis (transcription factor mutations → differentiation block; tyrosine kinase mutations → proliferation)
- Morphology and immunophenotype (what the blasts look like and what markers they express)
- Clinical features (symptoms of marrow failure + mass effects)
- Prognosis (stratified by cytogenetics)
- Key Concepts box (a summary Robbins always provides)
Having this skeleton in mind means you will never lose the thread of the argument.
Bottom line before you start reading: ALL is what happens when a lymphoid progenitor cell (B or T) acquires mutations that block its ability to mature, while simultaneously acquiring mutations that make it proliferate. The immature blasts pile up in the marrow and blood (and sometimes form masses), causing pancytopenia and organ infiltration. The specific mutation determines prognosis and targeted therapy options. TdT positivity identifies the tumor as a lymphoblast, not a myeloblast.
Good luck with Robbins! - Robbins, Cotran & Kumar, Pathologic Basis of Disease, pp. 556-558
I want you to give me this, uh, in point forms. And, uh, the pathogenesis in flowchart form.
Here is the full primer in point form, with the pathogenesis as a flowchart.
Pre-Reading Primer: ALL (Point Form)
1. What Is ALL?
- Cancer of immature lymphoid cells (lymphoblasts)
- Cells are "frozen" at an early developmental stage - cannot mature
- Blasts accumulate and crowd out normal bone marrow
- "Leukemia" = blasts flood the blood; "Lymphoma" = blasts form a solid mass
- ALL can be either or both → hence the name leukemia/lymphoma
2. Two Types: B-ALL vs. T-ALL
B-ALL (~85%)
- Cell of origin: pre-B lymphoblast in bone marrow
- Peak age: ~3 years (pre-B cells most numerous in early childhood)
- Presentation: classic leukemia (pancytopenia, blasts in marrow/blood)
T-ALL (~15%)
- Cell of origin: precursor T cell in the thymus
- Peak age: adolescent males
- Presentation: anterior mediastinal (thymic) mass ± leukemic picture
3. Pathogenesis - Flowchart
NORMAL LYMPHOID PROGENITOR (B or T cell precursor)
│
▼
┌─────────────────────────────────────────────────────────┐
│ HIT 1: Transcription Factor Mutation │
│ (master switches for maturation are disrupted) │
│ │
│ B-ALL: PAX5, TCF3, ETV6, RUNX1, KMT2A, PBX1 │
│ T-ALL: NOTCH1 (50–70% of T-ALLs) │
└─────────────────────────────────────────────────────────┘
│
▼
DIFFERENTIATION BLOCK
(cell cannot mature → stays as a blast)
│
▼
┌─────────────────────────────────────────────────────────┐
│ HIT 2: Complementary Proliferation Mutations │
│ (drive uncontrolled growth) │
│ │
│ • Tyrosine kinase activation │
│ → t(9;22) BCR::ABL1 [Philadelphia chromosome] │
│ - Produces 190 kDa BCR-ABL (stronger than CML) │
│ - TARGET of TKIs (imatinib, dasatinib) │
│ • RAS signaling mutations │
└─────────────────────────────────────────────────────────┘
│
▼
INCREASED SELF-RENEWAL + STEM CELL-LIKE PHENOTYPE
│
▼
< 10 TOTAL DRIVER MUTATIONS SUFFICIENT
│
▼
┌─────────────────────────────────────────────────────────┐
│ RESULT: FULL-BLOWN ALL │
│ • Blasts accumulate in marrow, blood, organs │
│ • Normal hematopoiesis is suppressed │
│ • ~90% of ALLs carry cytogenetically detectable │
│ chromosomal abnormalities │
└─────────────────────────────────────────────────────────┘
Key mutations at a glance:
| Mutation | Subtype | Note |
|---|---|---|
| t(12;21) ETV6::RUNX1 | B-ALL | Most common; 25% of cases; good prognosis |
| t(9;22) BCR::ABL1 (Ph+) | B-ALL | Adults/poor prognosis; targetable with TKIs |
| KMT2A rearrangements | B-ALL | Infants; poor prognosis |
| Hyperdiploidy (>50 chr) | B-ALL | Good prognosis |
| Hypodiploidy (<44 chr) | B-ALL | Poor prognosis |
| NOTCH1 mutation | T-ALL | 50-70% of T-ALL cases |
4. Clinical Features (Why the Patient Feels Sick)
Bone marrow failure (blasts crowd out normal cells):
- Low RBCs → fatigue, pallor, anaemia
- Low platelets → bruising, bleeding
- Low neutrophils → recurrent infections
Mass effects (blasts accumulate in organs):
- Lymphadenopathy, hepatomegaly, splenomegaly
- Bone pain (marrow expansion)
- T-ALL: anterior mediastinal mass → may compress trachea/SVC (emergency)
- CNS infiltration → meningismus, cranial nerve palsies (reason CNS treatment is given)
5. Diagnosis - Key Markers
- TdT (terminal deoxynucleotidyl transferase) - positive in ALL; the single most important marker distinguishing lymphoblasts from myeloblasts
- CD10 (CALLA) - expressed in most B-ALLs
- CD19, CD20 - B-cell markers; CD19 is the target of CAR-T therapy
- CD3, CD7 - T-cell markers; expressed in T-ALL
6. Treatment Highlights
- Intensive multi-drug chemotherapy is curative in most children
- Ph+ ALL (t(9;22)): add BCR-ABL TKI (e.g., imatinib) to chemo → dramatically improved outcomes
- CAR-T cells targeting CD19 - effective in relapsed/refractory B-ALL; high cost + serious toxicities
- Adults tolerate intensive regimens poorly → worse prognosis than children
- CNS prophylaxis/treatment is always included (intrathecal chemo ± cranial radiation)
7. Prognosis Principles
- Children: generally excellent (>90% long-term cure with modern therapy)
- Favorable markers: hyperdiploidy, t(12;21)
- Unfavorable markers: hypodiploidy, t(9;22) (Ph+), KMT2A rearrangements, age <1 yr or >10 yrs
- Adults: significantly worse outcomes than children
8. Three Concepts That Make Robbins Click
- Maturation arrest is the universal lymphoid tumor theme - ask "at what stage did the cell get stuck?" for every lymphoid neoplasm
- Leukemia vs. lymphoma is a clinical distinction, not biological - same clone, different presentation based on where blasts accumulate (>25% marrow involvement = leukemia)
- Genetics drive everything - cytogenetics determine prognosis AND which targeted drugs to add
9. Vocabulary Cheat Sheet
| Term | Meaning |
|---|---|
| Lymphoblast | Immature lymphoid precursor = the tumor cell in ALL |
| TdT | Enzyme in precursor lymphoid cells; positivity = ALL |
| CALLA / CD10 | Common ALL antigen; marker for B-ALL |
| Ph chromosome | t(9;22); BCR::ABL1; targetable with TKIs |
| Hyperdiploidy | >50 chromosomes; good prognosis |
| Hypodiploidy | <44 chromosomes; poor prognosis |
| CAR-T | Engineered T cells targeting CD19 in B-ALL |
| TdT | Distinguishes ALL from AML on IHC |
Source: Robbins, Cotran & Kumar, Pathologic Basis of Disease, pp. 556-558
This is a shared conversation. Sign in to Orris to start your own chat.