Amniotic membrane use and indication in ophthalmology in detail and easy to understand language
Reading File
Finding Sources
Finding Sources
Searching the Web
amniotic membrane transplantation ophthalmology indications uses 2024
Reading Web Page
https://eyewiki.org/Amniotic_Membrane_Transplant
Finding Sources
Finding Sources
Reading File
Reading File
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK567771
I now have comprehensive information to write a thorough, easy-to-understand answer. Let me compile everything.
Amniotic Membrane in Ophthalmology: A Complete Guide
What Is the Amniotic Membrane?
The amniotic membrane (AM) is the innermost layer of the placenta - the thin sac that surrounds a baby during pregnancy. It is harvested in a sterile environment during elective cesarean sections, from donors who are screened for infectious diseases (HIV, hepatitis, syphilis, etc.).
Think of it as nature's own "bandage" - it has been used by the body for 9 months to protect a growing baby, and it turns out to be remarkably useful for protecting and healing the eye too.
Structure: What Is It Made Of?
The amniotic membrane has three layers:
| Layer | What It Does |
|---|---|
| Epithelium | The inner facing cells |
| Basement membrane | A scaffold similar to the conjunctiva and cornea of the eye |
| Stroma | Contains growth factors, anti-inflammatory proteins, and collagen |
This structure is similar in composition to the conjunctiva (the clear membrane lining the eye), which is one reason it works so well in eye surgery.
How It Works (Mechanism of Action)
The amniotic membrane promotes healing through several powerful biological actions:
1. Promotes Epithelial Healing
The basement membrane acts as a scaffold - it supports the growth of new surface cells (epithelial cells) over damaged areas, similar to how a plaster supports skin healing.
2. Anti-Scarring (Anti-Fibrotic)
The stromal layer stops normal fibroblasts (repair cells) from turning into "scar-forming" myofibroblasts. This means wounds heal with less scarring, which is vital for preserving clear vision.
3. Anti-Inflammatory
It contains proteins that suppress inflammation and block destructive enzymes (proteases) that break down healthy tissue. This is why it works in chemical burns and inflammatory eye conditions.
4. Supports Stem Cells
The membrane provides a nurturing environment for limbal stem cells - the special cells at the edge of the cornea that continuously regenerate the corneal surface. Without them, the cornea loses its clarity.
5. Anti-Vascular (Anti-Angiogenic)
It inhibits abnormal blood vessel growth into the cornea (corneal neovascularization), which would otherwise cloud vision.
6. Antimicrobial Properties
It has some natural antimicrobial effects, reducing infection risk at the surgical site.
Forms Available
| Form | Description |
|---|---|
| Cryopreserved (e.g., AmnioGraft) | Stored frozen; retains structural and biological properties |
| Dehydrated (e.g., BioDOptix) | Dried form; easier to store at room temperature |
| Prokera | A self-retaining ring device with AM - can be placed in the office without surgery |
The development of Prokera was a major advance - it allows AM treatment to be placed in the eye clinic (no operating room needed), much like a contact lens.
Indications in Ophthalmology
1. CORNEAL DISEASES
a) Persistent Epithelial Defects (PED)
- When the surface of the cornea (epithelium) fails to heal despite standard treatment
- Causes: neurotrophic keratopathy (loss of corneal sensation), dry eye, diabetes, previous infection
- AM acts as a bandage, protecting the area and actively promoting healing
b) Corneal Ulcers and Stromal Melting
- Deep ulcers that threaten to perforate the cornea
- AM is placed as a graft (inlay) to fill in thinned areas and prevent perforation
- It reduces the inflammation that is "melting" the cornea
- Can be used in single or multi-layer stacking for deep defects
c) Chemical and Thermal Burns (Ocular Surface Burns)
- One of the most time-critical uses - ideally applied within 2 weeks of the burn
- Chemical burns (acid or alkali) cause massive inflammation and scarring
- AM dramatically reduces scarring, symblepharon formation (eyelids sticking to eyeball), and conjunctival destruction
- The 2024 American Academy of Ophthalmology assessment confirmed the efficacy of AMG in chemical/thermal burns
d) Bullous Keratopathy
- When the cornea swells and blisters form on its surface causing severe pain
- AM is used as a bandage to relieve pain and promote healing while awaiting corneal transplant
e) Infectious Keratitis
- Severe bacterial, fungal, or viral (herpes) corneal infections with large ulcers
- AM helps by reducing inflammation and creating favorable conditions for healing alongside antimicrobial treatment
f) Corneal Perforations (Small)
- Small corneal holes (e.g., from ulcers or trauma) can be patched with layered AM
- Important: AM cannot provide tectonic support for large perforations - that requires a corneal transplant
g) Recurrent Corneal Erosion
- Condition where the corneal surface repeatedly breaks down (often after an old corneal scratch)
- AM overlay can help restore the basement membrane and stop recurrences
2. CONJUNCTIVAL DISEASES
a) Pterygium Surgery
- Pterygium = a fleshy, wedge-shaped growth of conjunctiva that grows onto the cornea
- After surgical removal, AM is used to cover the raw area where tissue was removed
- Reduces recurrence rates and provides a better cosmetic outcome
- Alternative to conjunctival autograft (taking tissue from another part of the same eye)
b) Symblepharon Lysis
- Symblepharon = scar tissue causing the eyelid to stick to the eyeball
- After releasing these adhesions surgically, AM is placed to prevent them from reforming
- Used in conditions like Stevens-Johnson Syndrome, chemical burns, ocular cicatricial pemphigoid
c) Stevens-Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN)
- Severe drug reaction causing widespread skin and eye surface destruction
- One of the most important uses - AM should be applied urgently (ideally within 72 hours of onset)
- Applied over the palpebral and bulbar conjunctiva, eyelid margins, and into the fornix
- Early AM grafting greatly improves visual prognosis
- Wills Eye Manual specifically recommends suturing AM over the eyelid margin, palpebral conjunctiva, and fornix in severe hyperacute cases (<72 hours)
d) Conjunctival Reconstruction
- After removal of large conjunctival tumors
- Mucous membrane autografting or amniotic membrane transplantation for conjunctival resurfacing and fornicial restoration (Kanski's Clinical Ophthalmology)
e) Ocular Cicatricial Pemphigoid (OCP)
- Autoimmune condition causing progressive scarring of the conjunctiva
- AM helps in reconstruction of the fornix and bulbar conjunctiva
3. LIMBAL STEM CELL DEFICIENCY (LSCD)
This is one of the most exciting and advanced uses of AM.
Background: Limbal stem cells live at the edge (limbus) of the cornea and are responsible for keeping the corneal surface clear. When they are destroyed (by chemical burns, radiation, chronic contact lens wear, genetic conditions), the cornea becomes opaque and vascularized - causing blindness.
How AM helps:
- AM serves as the substrate (scaffold/bed) on which limbal stem cells are grown and then transplanted back onto the eye
- Two main approaches:
| Technique | Description |
|---|---|
| CLET (Cultivated Limbal Epithelial Transplantation) | Limbal cells grown in a lab on AM, then transplanted |
| SLET (Simple Limbal Epithelial Transplantation) | Small piece of limbal tissue placed directly on AM on the cornea - no lab needed |
SLET is particularly promising in developing countries as it removes the need for expensive cell culture laboratories.
- Oral mucosal cells can also be grown on AM as an alternative (COMET - Cultivated Oral Mucosal Epithelial Transplantation) - useful when both eyes are affected
4. SOCKET RECONSTRUCTION
- After removal of an eye (enucleation) or in contracted eye socket cases
- AM helps reconstruct conjunctival lining of the socket for prosthetic eye fitting
5. GLAUCOMA SURGERY (Adjunct Use)
- AM can be used as a covering over trabeculectomy blebs (drainage sites) that are leaking or failing
- Helps reduce scarring of the filtration bleb
6. DRY EYE DISEASE
- AM suspensions and dehydrated AM (e.g., Prokera device) are used for severe dry eye
- The Prokera device sits in the eye like a contact lens for several days, delivering the anti-inflammatory and healing benefits
- Particularly useful in severe, treatment-resistant dry eye
How Is It Applied? (Techniques)
| Method | Used For |
|---|---|
| Sutures (absorbable or non-absorbable) | Surgical placement in operating room |
| Fibrin glue | Quicker, sutureless fixation; increasingly popular |
| Self-retaining ring (Prokera) | In-office, no surgery needed |
| Conformer-held | In chemical burns - spread across entire surface and held by a plastic conformer |
Orientation matters:
- Epithelial side UP = acts as a replacement surface (graft/onlay)
- Stromal side DOWN on wound = anti-scar, anti-inflammatory effects are maximized (inlay)
- The stromal side is identified by its stickiness
Contraindications and Limitations
| Limitation | Explanation |
|---|---|
| Large corneal perforations | AM cannot provide structural support - needs corneal transplant |
| Active infection | Should be treated first; AM alone won't clear infection |
| Repeat use from same donor | Risk of hypersensitivity reactions - use different donor each time |
| Potential complication | Hypopyon (pus in anterior chamber) has been reported - usually sterile, responds to steroids |
Summary: Quick Reference Table
| Indication | Role of AM |
|---|---|
| Persistent epithelial defect | Bandage - promotes healing |
| Corneal ulcer/melting | Graft - fills defect, anti-inflammatory |
| Chemical/thermal burns | Bandage + anti-scar - urgent application |
| SJS/TEN | Anti-scar, prevents symblepharon - apply <72hrs |
| Pterygium excision | Graft - covers raw area, reduces recurrence |
| LSCD | Substrate for stem cell transplantation |
| Symblepharon | Prevents re-formation after lysis |
| Socket reconstruction | Provides conjunctival lining |
| Dry eye (severe) | Prokera device - anti-inflammatory |
| Bullous keratopathy | Pain relief bandage |
Key Points to Remember
- AM is the innermost layer of the placenta, harvested from consented donors during C-sections
- It works by promoting healing, reducing scarring, suppressing inflammation, and supporting stem cells
- It can be used as a graft (to fill/replace tissue) or as a bandage (to protect and promote healing)
- Prokera allows in-office use without surgery
- Chemical burns and SJS are time-critical indications - early application (<2 weeks and <72 hours respectively) improves outcomes significantly
- It is a substrate for limbal stem cell transplantation - a potential cure for corneal blindness from LSCD
- It cannot replace the cornea structurally - large perforations need corneal transplants
Sources: Wills Eye Manual; Kanski's Clinical Ophthalmology (10th ed.); StatPearls - Amniotic Membrane Graft (NCBI, updated 2023); EyeWiki - Amniotic Membrane Transplant; AAO Ophthalmic Technology Assessment 2024 (Chemical/Thermal Burns)
Corneal graft rejection :clinical features and management
Finding Sources
Finding Sources
Searching the Web
corneal graft rejection clinical features management keratoplasty 2024
Reading File
Reading File
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK519043
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer. Let me compile it.
Corneal Graft Rejection: Clinical Features and Management
What Is Corneal Graft Rejection?
A corneal transplant (keratoplasty) works because the cornea is an immunologically privileged site - it has no blood vessels or lymphatics, and very few antigen-presenting cells. This means the immune system normally "ignores" a donor cornea.
Rejection happens when this privilege is lost. The host immune system recognizes the donor cornea as "foreign" and mounts an attack against it. This is a type IV (cell-mediated) hypersensitivity reaction - primarily T-lymphocytes are responsible.
Key point: Graft rejection can only occur in a graft that has previously been clear for at least 2 weeks after surgery. Before that, other causes of cloudiness (primary graft failure, surgical trauma) are more likely.
Immunological Background
The cornea loses its immune privilege when:
- Neovascularization grows into the cornea (new blood vessels carry immune cells)
- Lymphatic vessels develop in the limbal area
- Inflammation is present (pre- or post-op)
Once sensitized, host T-cells recognize HLA (Human Leukocyte Antigen) donor proteins on the graft and destroy the tissue - predominantly the endothelium, which is the most critical single layer.
Risk Factors
Pre-Operative (Host Eye Factors)
| Factor | Why It Increases Risk |
|---|---|
| Corneal vascularization | Most important risk factor - provides route for immune cells |
| Previous keratoplasty (repeat graft) | Host is already sensitized |
| Large graft (>8 mm diameter) | Closer to vascular limbus |
| Eccentric graft placement | Closer to limbal vessels |
| Previous herpetic infection | Immune activation; HSV can reactivate |
| Active pre-op inflammation | Primes the immune response |
| Glaucoma | Associated with poor prognosis |
| Young recipient age | More vigorous immune system |
Donor Factors
- Male donor to female recipient - Gender incompatibility has emerged as a significant risk factor. A female donor cornea can go to either sex; a male donor cornea should NOT be given to a female recipient (HLA-Y antigen mismatch)
- Large donor button
- HLA mismatch (minor beneficial effect of HLA matching)
Post-Operative Factors
- Loose or broken sutures (induce vascularization)
- Steroid non-compliance (most preventable cause!)
- Secondary infection (especially herpes)
- Uncontrolled IOP
- Missed follow-up appointments
Timing
- Can occur days to years after keratoplasty (even reported 20 years later)
- Most common in the first year after surgery
- Incidence is highest at ~12 months post-op
Types of Corneal Graft Rejection
The rejection can affect each layer of the cornea separately, or in combination.
| Type | Frequency | Timing | Key Sign |
|---|---|---|---|
| Endothelial | 50% - Most common | Any time | Khodadoust line |
| Mixed | ~30% | Variable | Multiple signs |
| Subepithelial | Variable | ~3 months avg | Krachmer spots |
| Epithelial | ~2% - Least common | Early | Epithelial rejection line |
| Stromal | Less common | Variable | Stromal haze/infiltrate |
Clinical Features
Symptoms (What the Patient Feels)
Mnemonic: RSVP
- Redness
- Sensitivity to light (photophobia)
- Vision decrease (blurred vision)
- Pain (mild to moderate)
Important: Many cases are asymptomatic and detected only on routine slit-lamp follow-up. This is why regular post-keratoplasty review is critical.
Signs (What You See on Slit Lamp)
1. Endothelial Rejection - THE MOST IMPORTANT
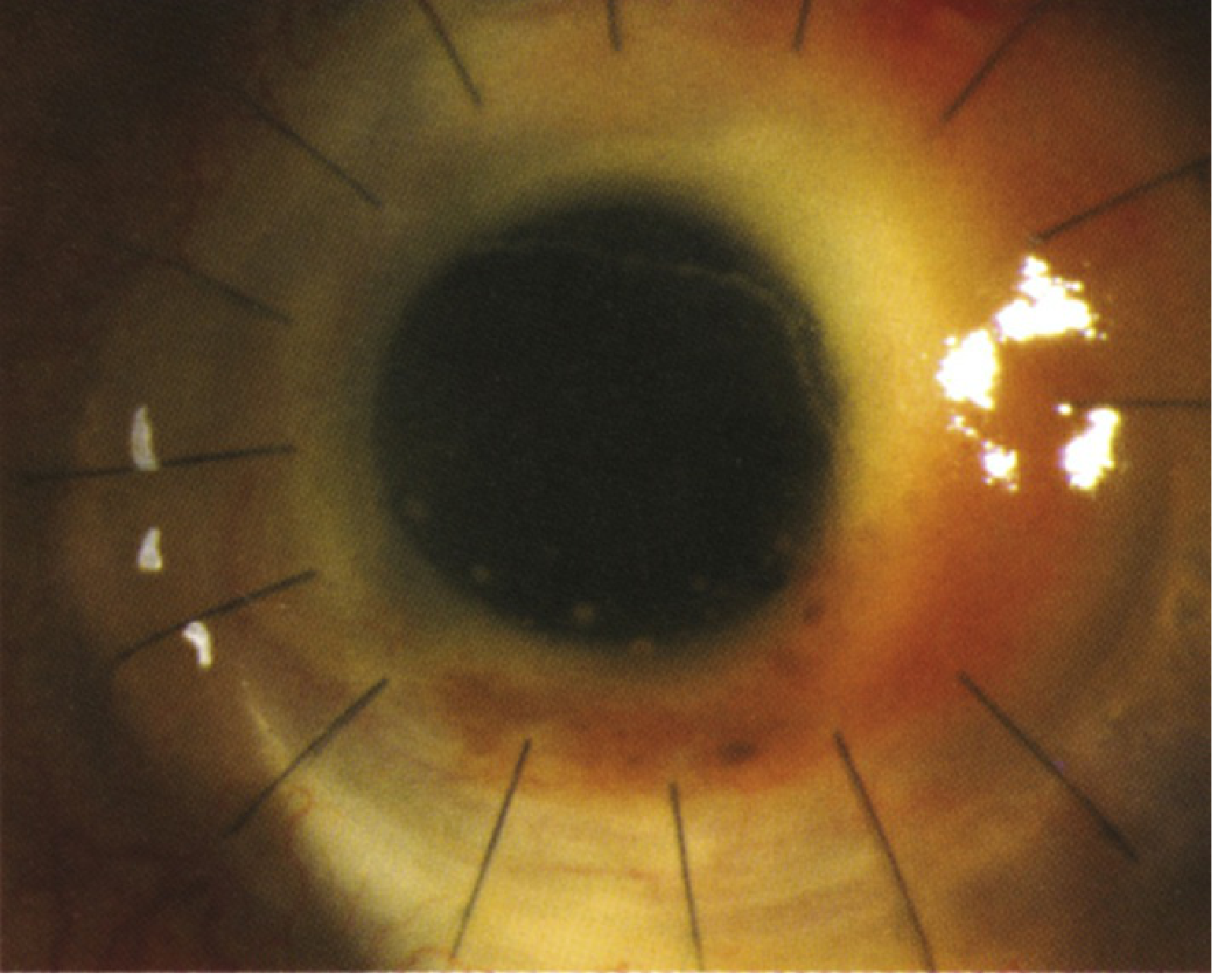
The Khodadoust Line - the hallmark sign:
- A linear row of keratic precipitates (KPs) marching across the donor endothelium
- Starts at the graft-host interface inferiorly and moves superiorly
- Represents the advancing front of immune destruction
- To one side of the line: endothelium is destroyed - cornea is edematous (cloudy)
- To the other side: endothelium still intact - cornea is clear
- Associated with ciliary injection (redness around the cornea) and anterior chamber cells
Other endothelial signs:
- KPs localized only to donor endothelium (not on recipient) - this distinction from uveitis is critical
- Diffuse stromal and epithelial edema (graft becomes hazy/white)
- If early: AC cells without graft changes
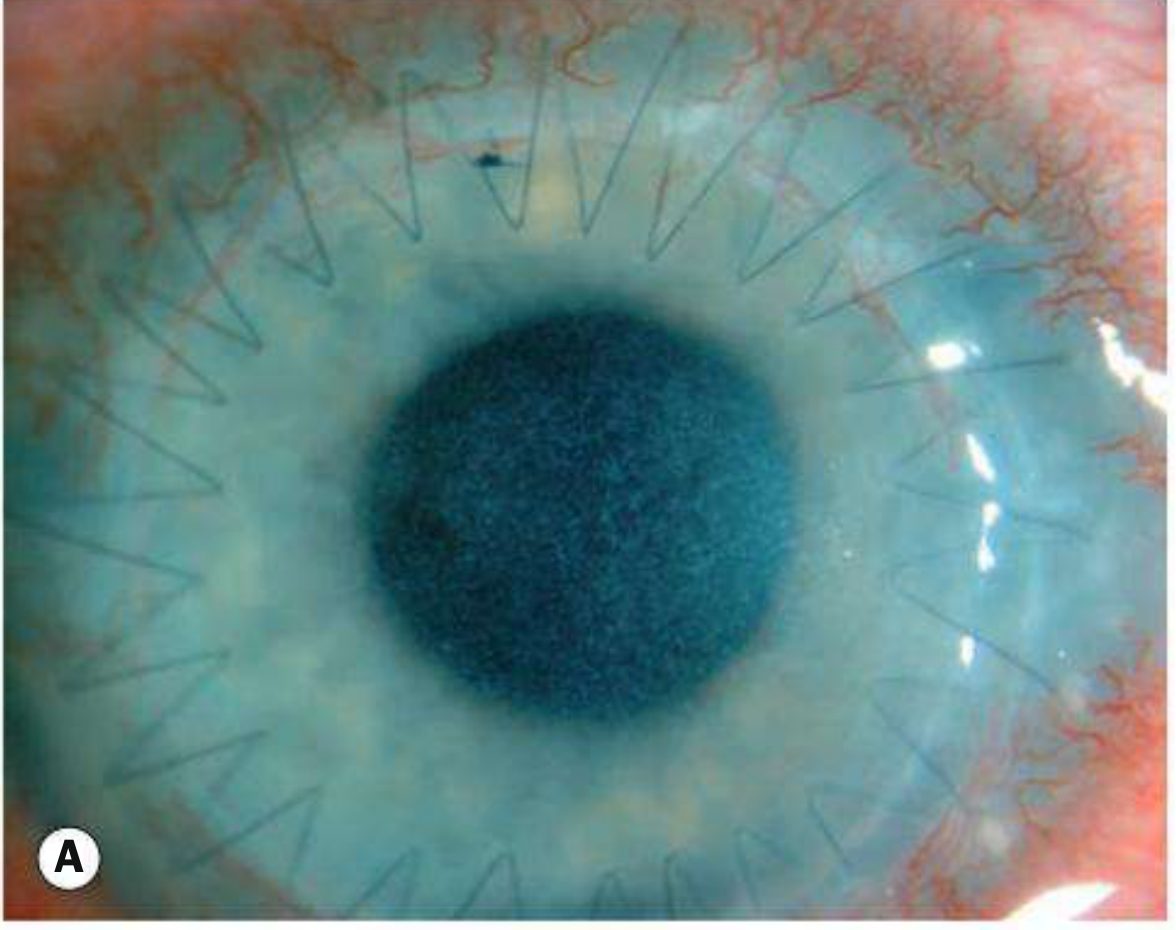
2. Epithelial Rejection
- An elevated, irregular, winding line of abnormal epithelium
- Crosses the graft from periphery to center
- Eye is relatively quiet (mildly inflamed or even white)
- Occurs at average of 3 months post-op
- Best prognosis of all types - responds readily to treatment
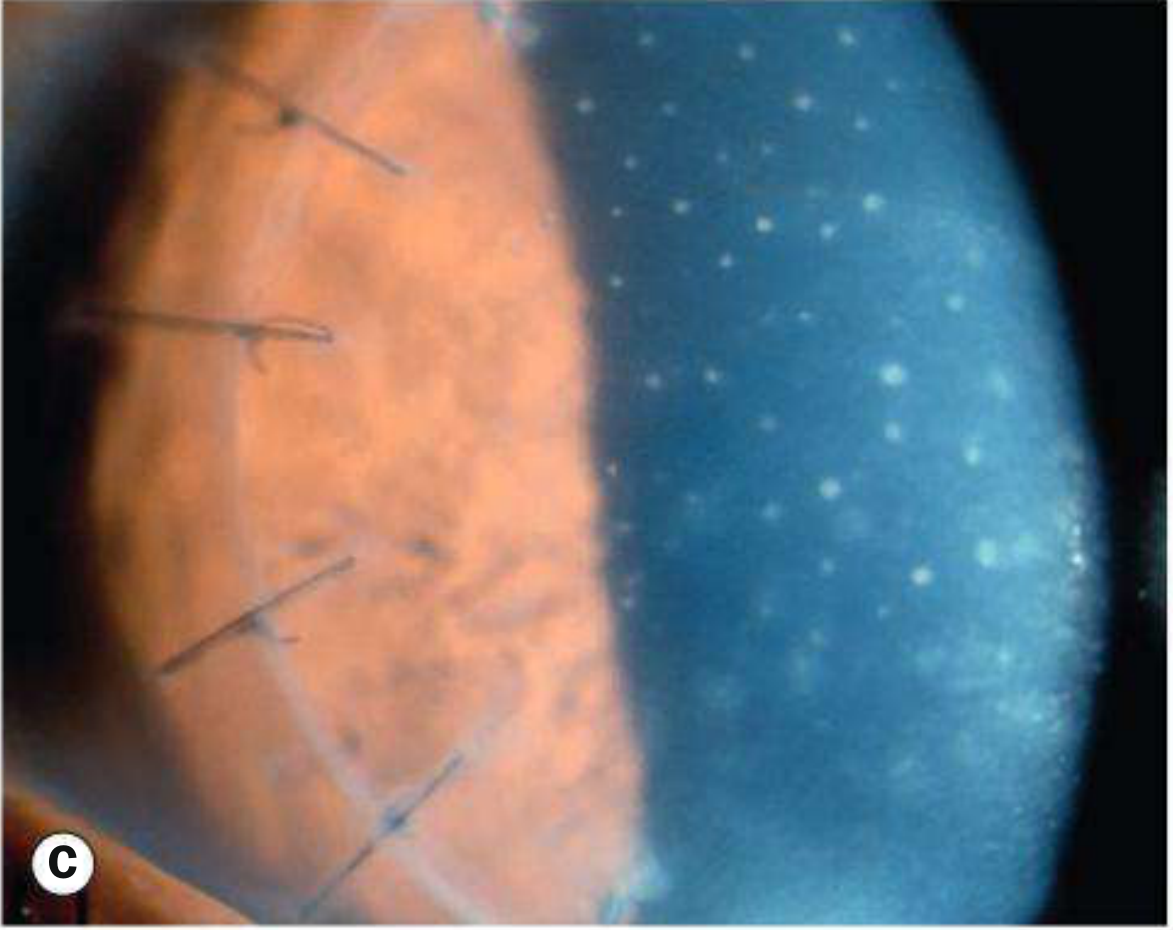
3. Subepithelial Rejection (Krachmer Spots)
- Multiple round, white subepithelial infiltrates scattered across the donor cornea
- Look similar to adenoviral keratoconjunctivitis (important differential)
- Located only on the donor tissue
- Associated with mild stromal involvement in severe cases
4. Stromal Rejection
- Deep stromal haze or infiltrate in the graft
- Can be chronic (slowly progressive) or hyperacute (rapid onset, often with endothelial involvement)
- Stromal neovascularization may be seen at the graft margin
5. Ciliary Injection
- Earliest, non-specific sign - redness concentrated around the corneal limbus
- Usually the first thing the patient notices
Progression of Endothelial Rejection (Timeline on Slit Lamp)
| Stage | What You See |
|---|---|
| Very early | AC cells and flare only; graft looks normal |
| Early | KPs on graft endothelium; mild stromal haze |
| Established | Khodadoust line; localized graft edema adjacent to line |
| Advanced | Diffuse graft edema; graft fully opaque |
| Irreversible failure | Total opacification; no response to treatment after 2 months |
Key concept: Every visible KP on the endothelium represents a focal, irreversible area of endothelial cell death. This is why speed of treatment matters enormously.
Differential Diagnosis
| Condition | How to Distinguish |
|---|---|
| Uveitis | KPs not limited to graft only; spread to recipient endothelium; history of uveitis |
| Infective keratitis | Corneal infiltrate ± hypopyon; discharge; cultures positive |
| Raised IOP | Epithelial edema only; no KPs; clears when IOP controlled |
| Epithelial downgrowth | Advancing smooth/scalloped line; does NOT respond to steroids |
| Primary graft failure | Occurs in first 2 weeks; never had a clear period |
| HSV recurrence | Dendritic ulcer; pseudodendrites; known history |
| Recurrent disease | Same original disease (e.g., dystrophy) recurring in graft |
Workup
- Detailed history - Date of transplant, indication for transplant, current steroid regimen, compliance, recent steroid taper, history of HSV
- Slit lamp examination - Systematic inspection of epithelium, stroma, endothelium; look for KPs, rejection lines, subepithelial infiltrates, neovascularization
- IOP measurement - Mandatory (steroids can raise IOP; raised IOP itself causes edema)
- Specular microscopy - To assess endothelial cell count and early cellular changes
Management
The Golden Rule:
"Early intensive treatment greatly improves the likelihood of reversing the rejection" - Kanski's Clinical OphthalmologyDo not delay. Treat the same day.
Step 1: Endothelial Rejection (Most Urgent)
This requires the most aggressive treatment - every hour lost = more endothelial cells permanently destroyed.
Topical Steroids (First Line - Always):
- Prednisolone acetate 1% every 1 hour while awake
- OR Difluprednate 0.05% every 2 hours while awake
- Add dexamethasone 0.1% ointment at bedtime
- Taper very slowly over weeks to months once improvement is noted
Systemic Steroids (For Severe/Recurrent/Resistant Cases):
- Oral prednisone 40-80 mg/day for 1-2 weeks, then tapered
- OR IV methylprednisolone 500 mg/day for 1-3 consecutive days (pulse therapy)
- Most effective when given within 8 days of symptom onset
- Can suppress the rejection AND reduce the risk of future episodes
- Subconjunctival injection: Betamethasone 3 mg in 0.5 mL or dexamethasone 4 mg/mL
Adjunct Treatment:
- Cycloplegic (e.g., cyclopentolate 1% three times daily, or homatropine 2% twice daily) - relieves ciliary spasm, prevents synechiae formation
- IOP control - timolol 0.5% or other glaucoma drops if pressure is elevated
- Topical cyclosporine 0.05-2% twice to four times daily - adjunct; slower onset but useful for prevention and recurrence
Hospitalization:
- Severe rejection cases: admit for IV steroids + close monitoring
Step 2: Epithelial and Stromal Rejection (Less Urgent, but Act Promptly)
- Double the current topical steroid dose, or use prednisolone acetate 1% four times daily (whichever is more frequent)
- Add cycloplegic agent and IOP control
- Topical cyclosporine as adjunct
- These types have a higher reversibility rate than endothelial rejection
Step 3: Follow-Up After Starting Treatment
- Review every 3-7 days initially
- Once improvement confirmed: slowly taper steroids (over weeks to months)
- Some patients need low-dose maintenance steroids for months to years
- Regularly check IOP in anyone on long-term topical steroids (risk of steroid-induced glaucoma)
If Treatment Fails (Irreversible Rejection)
- A graft is labeled immunologically failed if rejection does not clear after 2 months of intensive treatment
- At this point, a repeat corneal transplant is the only option
- Note: repeat grafts have a significantly higher rejection risk
Prevention of Rejection
| Strategy | Detail |
|---|---|
| Steroid compliance | Most important preventable factor - must never skip drops |
| Patient education | Teach RSVP symptoms; instruct to seek urgent care immediately if symptoms arise |
| Long-term low-dose steroids | High-risk patients maintained on prednisolone 1% four times daily indefinitely |
| Topical cyclosporine | Helpful in prevention for high-risk cases |
| Avoid male donor to female recipient | Gender-matched grafting where possible |
| Anti-VEGF pre-treatment | Bevacizumab injections pre-op to reduce corneal vascularization in high-risk eyes |
| HLA matching | Minor benefit; used in high-risk cases in some centers |
| Suture management | Remove loose/broken sutures promptly - prevents vascularization |
| Lamellar keratoplasty | DSEK/DMEK instead of PKP where possible - much lower rejection rates |
Rejection Rates by Graft Type
| Procedure | Rejection Rate | Notes |
|---|---|---|
| PKP (full thickness) | Highest (~10-30% in 5 yrs, higher in high-risk eyes) | All layers exposed to immune system |
| DALK (deep anterior lamellar) | 1-24% | No endothelial cells transplanted; endothelial rejection impossible |
| DSEK/DSAEK | ~10% rejection; ~5% primary failure | Endothelial rejection possible; slower onset than PKP |
| DMEK | ~1.9% rejection - lowest | Thinnest tissue transplanted; better immune tolerance |
This is one reason the field is shifting toward lamellar (partial-thickness) grafts - significantly lower rejection risk than full-thickness PKP.
Summary: Quick Reference
| Feature | Detail |
|---|---|
| Most common type | Endothelial (50%) |
| Hallmark sign | Khodadoust line - linear KPs on donor endothelium |
| Other signs | Krachmer spots, epithelial rejection line, stromal haze, ciliary injection |
| Symptoms | Redness, photophobia, blurred vision, pain (RSVP) - often asymptomatic |
| Treatment - mild | Topical prednisolone 1% hourly |
| Treatment - severe | IV methylprednisolone 500 mg x 1-3 days + topical hourly steroids |
| Adjuncts | Cycloplegic, IOP control, topical cyclosporine |
| Follow up | Every 3-7 days; taper steroids slowly |
| Irreversible failure | No response after 2 months = repeat graft |
| Most preventable cause | Steroid non-compliance |
Sources: Kanski's Clinical Ophthalmology - A Systematic Approach, 10th Ed.; Wills Eye Manual, Chapter 4.28; EyeWiki - Corneal Allograft Rejection and Failure; StatPearls - Corneal Graft Rejection (NCBI, 2023)
This is a shared conversation. Sign in to Orris to start your own chat.