contact granuloma of vocal cord in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
"contact granuloma" AND "vocal cord"
Reading File
Finding Sources
Reading Article
PMID: 42140868
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"laryngeal contact granuloma" AND treatment
Loading Image
Loading Image
Reading Article
PMID: 38206391
Reading Article
PMID: 37125377
CONTACT GRANULOMA OF THE VOCAL CORD
A Comprehensive 50-Mark Answer | RGUHS University Standard
DEFINITION AND SYNONYMS
Contact granuloma (CG) is a benign inflammatory lesion that arises from the medial surface of the arytenoid cartilage, specifically from the vocal process, characterized by proliferation of granulation tissue with epithelial hyperplasia.
Synonyms (all refer to the same lesion):
- Contact ulcer or granuloma
- Vocal process granuloma (VPG)
- Intubation granuloma (when post-intubation)
- Contact pachydermia
- Peptic granuloma
- Arytenoid granuloma
(Scott-Brown's Otorhinolaryngology, 8th ed.; Cummings Otolaryngology, 7th ed.)
ANATOMY OF RELEVANCE
POSTERIOR LARYNX - KEY STRUCTURES
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
┌─────────────────────────────────────┐
│ ARYTENOID CARTILAGE │
│ │
│ ┌─────────────┐ │
│ │ Vocal Process│ ← Site of CG │
│ │ (Cartilaginous│ │
│ │ Glottis) │ │
│ └─────────────┘ │
│ │
│ Covered by: THIN MUCOPERICHONDRIUM │
│ (only 2-3 cell layers thick) │
│ → Highly susceptible to trauma │
└─────────────────────────────────────┘
Glottis = Membranous (ant 3/5) + Cartilaginous (post 2/5)
Contact granuloma arises at the CARTILAGINOUS GLOTTIS
(vocal process of arytenoid = junction of posterior 1/3
of vocal fold)
The vocal process is covered by thin mucoperichondrium with minimal submucosa, making it susceptible to repeated mechanical trauma and ulceration. (Dhingra's Diseases of ENT Head & Neck Surgery)
HISTORICAL BACKGROUND
- 1928: Jackson - first described "contact ulcer of the larynx" in men with vocally demanding occupations
- 1978: Goldberg, Noyek, Pritzker - established link with gastroesophageal reflux (laryngeal granuloma secondary to GER)
- 1985: Ward & Hanson - elucidated role of LPR in etiopathogenesis
- 2026: Wang et al. (Expert Consensus China) - Delphi consensus established LPR + mechanical injury as main causes; biopsy generally not required (PMID 42140868)
EPIDEMIOLOGY
| Feature | Contact Granuloma | Intubation Granuloma |
|---|---|---|
| Sex | Predominantly males | More common in females |
| Age | 30-60 years | Any age |
| Occupation | Voice professionals, executives | Post-surgical/ICU patients |
| Side | Usually unilateral (right > left) | Often bilateral |
- Represents ~1-2% of all benign laryngeal lesions
- Men develop granulomas secondary to hyperfunction; women develop them more commonly after intubation
- Psychological stress is also implicated in some patients
(Cummings Otolaryngology, 7th ed., p. 1125; Scott-Brown's, 8th ed.)
ETIOPATHOGENESIS
FLOWCHART 1: Pathogenesis of Contact Granuloma
ETIOLOGICAL FACTORS
│
├──────────────────────────────────────┐
│ │
MECHANICAL TRAUMA LARYNGOPHARYNGEAL REFLUX (LPR)
│ │
┌────┴────┐ Acid pepsin → posterior larynx
│ │ (especially during sleep/recumbent)
Vocal Intubation │
Abuse Trauma Mucosa pH imbalance
│ │ Impaired mucosal defense
└────┬────┘ │
│ │
▼ ▼
High-velocity impact Inflammation of mucoperichondrium
of vocal processes │
("Glottal stroke" / hard attack) │
│ │
└──────────────┬───────────────────────┘
│
▼
MUCOSAL ULCERATION of vocal process
│
▼
REPAIR RESPONSE
│
┌────────────┴────────────┐
│ │
Granulation tissue Fibrous tissue
proliferation deposition
│
▼
CONTACT GRANULOMA
(± epithelial hyperplasia)
│
▼
Repeated trauma prevents healing
→ Ulcer persists or granuloma enlarges
→ May become pedunculated
→ Eventually spontaneous detachment (3-6 months)
Mechanical Factors (Vocally Induced):
- Hard glottal attack - forceful apposition (slamming) of arytenoids at onset of phonation
- Habitual low-pitch speech - creaky hyperfunctional voice
- Chronic throat clearing and coughing - repeated high-velocity impact
- Glottal incompetence - vocal fold atrophy with compensatory hyperfunction
LPR / Chemical Factors:
- Acid pepsin reflux inflames posterior larynx
- May directly prevent mucosal healing
- Stimulates throat clearing, creating a vicious cycle
- Effective even without symptomatic heartburn (silent LPR)
(Scott-Brown's, 8th ed., p. 7387-7392; Cummings, 7th ed., p. 1125; K.J. Lee's, 10th ed., p. 923)
PATHOLOGY
Gross Appearance:
- Early stage: Depressed, ulcerated area with whitish exudate on vocal process
- Established: Sessile or bilobed heaped-up lesion, typically at vocal process
- Mature: Pedunculated, lobulated mass - may flip above and below vocal fold plane with breathing
- Resolving: Base shows characteristic "bruise" after spontaneous detachment
Microscopy:
- Surface: Ulcerated or covered by squamous epithelium showing hyperplasia
- Core: Proliferating granulation tissue with:
- Fibroblasts and capillaries
- Inflammatory cells (lymphocytes, plasma cells, neutrophils)
- Fibrinous exudate on ulcerated surface
- Base: Dense fibrous tissue attached to perichondrium
- NO giant cells (distinguishes from true granulomatous diseases)
- May show arytenoid cartilage sclerosis on CT in long-standing cases
(Cummings, 7th ed., p. 1125; Stell and Maran's Head & Neck Surgery)
CLINICAL FEATURES
Symptoms:
- Pain/Discomfort - localized to posterosuperior larynx, worse on phonation
- Referred otalgia - ipsilateral ear pain (via Arnold's nerve, CN X)
- Foreign body sensation in throat
- Hoarseness - mild, often only when lesion is very large (membranous folds unaffected)
- Vocal fatigue - especially in voice professionals
- Chronic throat clearing - both symptom and perpetuating factor
- LPR symptoms - sour taste, morning voice changes, choking episodes
- Stridor - only in large lesions causing significant posterior glottic obstruction
Important Note:
"The speaking voice of a patient with a contact ulcer or granuloma may sound normal or only slightly husky." - Cummings Otolaryngology, 7th ed.
The patient often speaks with a held-back vocal quality, habitual throat clearing, and overly low, monotone voice.
DIAGNOSIS
FLOWCHART 2: Diagnostic Algorithm
SUSPECTED CONTACT GRANULOMA
Patient: Often male, voice professional
Symptoms: Throat pain, referred otalgia, throat clearing
│
▼
DETAILED HISTORY
├─ Voice use patterns (occupation, habits)
├─ Intubation history
├─ LPR symptoms (caffeine, alcohol, late meals)
├─ Psychological stress
└─ Previous treatment
│
▼
LARYNGEAL EXAMINATION
│
┌────┴────┐
│ │
Indirect Flexible
Laryngoscopy Nasopharyngolaryngoscopy
│ │
└──────┬────────┘
│
▼
VIDEOENDOSTROBOSCOPY
┌──────────────────────────┐
│ - Bilobed/heaped lesion │
│ - At vocal process │
│ - Erythema around base │
│ - Assess VF mobility │
│ - Rule out glottal incomp│
└──────────────────────────┘
│
┌────────┴──────────┐
│ │
CLASSIC APPEARANCE ATYPICAL/
(No biopsy needed) SUSPICIOUS
│ │
▼ ▼
CONSERVATIVE MICROLARYNGOSCOPY
MANAGEMENT + BIOPSY
(Rule out malignancy,
TB, specific granulomas)
│
▼
ADDITIONAL TESTS
├─ 24-hr pH monitoring/Impedance
├─ Reflux Finding Score (RFS)
├─ CT larynx (cartilage sclerosis)
├─ Voice analysis (acoustic, aerodynamic)
└─ Laryngeal EMG (if VF immobility)
Laryngoscopic Features:
- Bilobed, heaped-up lesion at vocal process of arytenoid
- At glottal closure: opposite vocal process fits into the cleft of bilobed granuloma
- Surrounding erythema on vocal process and medial arytenoid surface
- Mature lesion: pedunculated, flips above/below vocal fold with respiration
Videoendostroboscopy:
- Vocal fold mucosal wave - normal (membranous folds unaffected)
- Can detect glottal incompetence (atrophy with posterior gap)
- Assess lesion mobility and attachment
(Cummings, 7th ed.; K.J. Lee's, p. 923)
LARYNGOSCOPIC IMAGES FROM TEXTBOOKS
Fig 1: Contact Granuloma - Cummings Otolaryngology
(A) Right posterior vocal fold bilobed granuloma with surrounding erythema. (B) Same patient at phonatory contact - left arytenoid process fitting into the cleft.
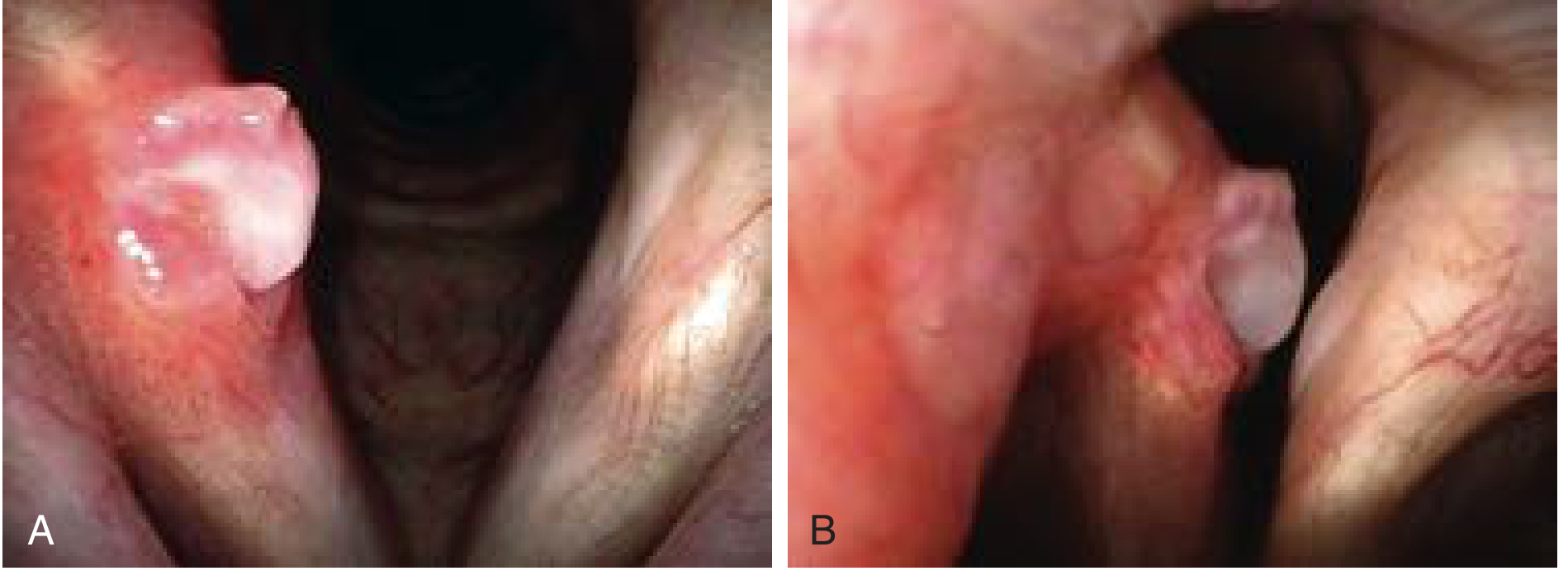
Fig 2: Granuloma Evolution - Maturation and Spontaneous Detachment
(A) Large bilobed pedunculated granuloma. (B) Inferior lobule has detached - single spherical granuloma remains. (C) Remaining granuloma detached - characteristic bruise at base persists.

Fig 3: Intubation Granuloma
(A) Bilateral granulomas with posterior commissure pressure necrosis divots. (B) Same patient months later - spontaneous detachment leaving the divots visible.
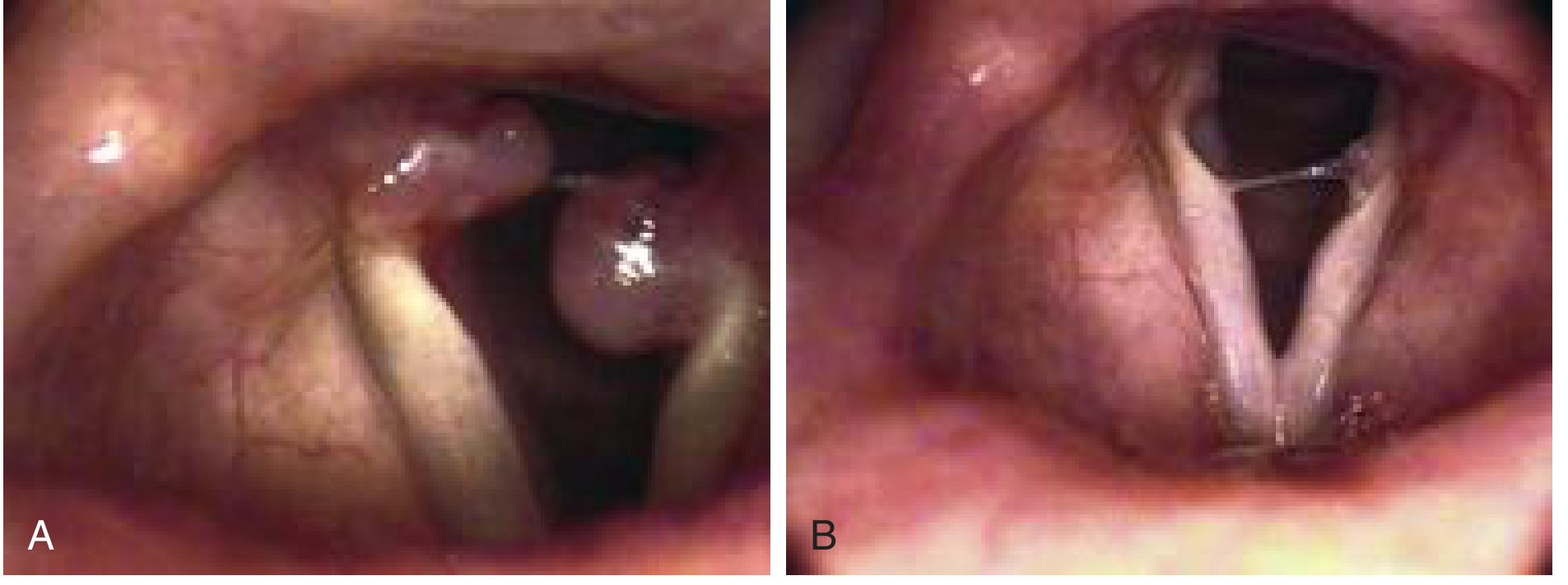
Fig 4: Arytenoid Granuloma - Scott-Brown's

DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Features |
|---|---|
| Malignancy (SCC) | Hard, irregular, bleeds easily; biopsy mandatory |
| Vocal nodules | At ant 1/3 - post 2/3 junction, bilateral, soft |
| Specific granulomas (TB, Syphilis, Wegener's) | Systemic signs, culture, biopsy with giant cells |
| Amyloidosis | Submucosal, homogeneous, Congo Red staining |
| Pachydermia laryngis | Diffuse thickening, no discrete lesion |
| Pyogenic granuloma | Post-traumatic/surgical; more vascular |
| Papilloma | Multiple, irregular, HPV-related |
| Teflon granuloma | History of VF injection |
(Dhingra's ENT; Hazarika's ENT)
MANAGEMENT
FLOWCHART 3: Management Protocol
CONTACT GRANULOMA - MANAGEMENT ALGORITHM
│
▼
CONSERVATIVE TREATMENT FIRST
(3-6 months trial in ALL patients)
│
┌───────────┴────────────┐
│ │
TREAT REFLUX VOICE THERAPY
(ALWAYS - even + VOCAL HYGIENE
without symptoms)
│ │
├─ Lifestyle changes ├─ Raise habitual pitch
├─ Diet modification ├─ Eliminate throat clearing
├─ PPI (high dose, ├─ Reduce vocal force
│ BID x 3-6 months) ├─ Vocal rest
├─ Avoid: caffeine, ├─ Hydration
│ alcohol, late meals └─ Treat any hyperfunction
├─ Head-end elevation
└─ Smoking cessation
│
▼
REASSESS at 6-8 weeks
│
┌─────────┴──────────┐
│ │
IMPROVING NOT IMPROVING
Continue Rx │
3-6 months ▼
INTRALESIONAL STEROID
INJECTION
(Triamcinolone, depot,
in clinic videoscopy)
OR
INHALED STEROIDS
(Triamcinolone/Mometasone)
│
▼
REASSESS 6-8 weeks
│
┌─────────┴──────────┐
│ │
RESOLVED REFRACTORY
│
▼
BOTULINUM TOXIN INJECTION
(Thyroarytenoid-LCA complex)
- Chemical denervation
- Reduces arytenoid impact force
- 2.5-5 IU per side
- Expect temporary dysphonia
│
▼
REASSESS
│
┌────────────┴──────────┐
│ │
RESOLVED PERSISTENT
────────────────
SURGERY (LAST RESORT)
Microlaryngoscopy + Excision
├─ Cold steel (preferred)
├─ CO2 laser / KTP / PDL
├─ Leave BASE/PEDICLE intact
├─ Concurrent steroid injection
└─ Continue anti-reflux therapy
│
▼
HIGH RECURRENCE RATE
Continue PPIs + voice Rx
post-operatively
1. CONSERVATIVE MANAGEMENT
A. Antireflux Treatment (MANDATORY in ALL cases)
- Lifestyle: Avoid caffeine, alcohol, carbonated drinks, spicy/fatty foods, late night meals; head-end elevation during sleep; smoking cessation
- Proton Pump Inhibitors (PPIs): High dose, twice daily (e.g., Omeprazole 40 mg BD or Rabeprazole 20 mg BD) for minimum 3-6 months
- Effective even in patients with no symptomatic GERD (silent LPR)
- Barium swallow and pH monitoring remain controversial for routine use
B. Voice Therapy and Vocal Hygiene
- Eliminate hard glottal attack - use breathy voice onset
- Raise habitual speaking pitch (low creak voice is a major cause)
- Eliminate throat clearing and voluntary coughing
- Adequate hydration (minimum 8 glasses/day)
- Amplification devices for vocally demanding professions
- Voice rest (relative, not absolute)
Natural History: Maturation and spontaneous resolution in 3-6 months is common; hence conservative management is attempted first.
2. INTRALESIONAL CORTICOSTEROID INJECTION
- Depot corticosteroid (triamcinolone acetonide) injected directly into the lesion and base
- Can be done in the videoendoscopy clinic (no GA required)
- Reduces granuloma size, relieves symptoms
- Inhaled steroids (triamcinolone, mometasone) as alternative - avoids systemic effects
- Recent evidence (Qiang et al., Eur Arch ORL 2024): Hormone injection + acid suppression shows significantly higher curative ratio and shorter healing time than acid suppression alone (P=0.018) (PMID 38206391)
3. BOTULINUM TOXIN INJECTION
- Injection into thyroarytenoid-lateral cricoarytenoid (TA-LCA) muscle complex on ipsilateral side
- Reduces adduction force, prevents repeated trauma to vocal process
- Dose: 2.5-5 IU per side
- Patient must be counseled about temporary dysphonia (significant, expected side effect)
- Indicated for: refractory cases, adjunct to surgery, recurrent granuloma
- Recent evidence (Pan et al., Am J Otolaryngol 2022): Thyroarytenoid botulinum toxin injection effective for refractory CG (PMID 35567839)
- 2023 study (Woo et al.): 5/5 patients with botulinum toxin had complete remission (PMID 37125377)
4. SURGICAL MANAGEMENT
Indications:
- Symptomatic lesion not responding to 3-6 months of conservative therapy
- Large obstructing granuloma causing airway compromise
- Suspicion of malignancy / atypical features requiring biopsy
Principles:
- LAST RESORT - high post-operative recurrence is predictable
- Microlaryngoscopy under GA
- Instruments: cold steel cup forceps (preferred), CO2 laser, KTP laser, PDL, Thulium laser
- Remove lesion but leave the base/pedicle undisturbed to minimize re-ulceration
- Concurrent intralesional steroid injection at the base
- Continue antireflux therapy and voice therapy post-operatively
Recurrence: Very high (up to 50-90% without addressing underlying etiology); recurrent lesions are often more recalcitrant (K.J. Lee's, p. 923)
INTUBATION GRANULOMA - SPECIAL CONSIDERATIONS
| Feature | Contact Granuloma | Intubation Granuloma |
|---|---|---|
| Sex | Predominantly male | More common in female |
| Cause | Voice abuse + LPR | ET tube trauma |
| Laterality | Usually unilateral | Often bilateral |
| Natural history | Longer course | Spontaneously resolves faster |
| Response to PPI+SI | Slower, less responsive | Better response, shorter treatment |
| Arytenoid sclerosis | Less common | Common on CT |
- Occurs 4-6 weeks after intubation (brief or prolonged)
- May be associated with posterior glottic incompetence (tissue loss) or arytenoid fixation in severe cases
- For recent injuries with normal VF motion → conservative approach (antireflux + inhaled steroids)
- For impaired VF motion → direct microlaryngoscopy with excision + steroid injection
- Study (Woo et al. 2023): IG more responsive to PPI + steroid inhalation; shorter treatment duration than contact granuloma (PMID 37125377)
PROGNOSIS AND FACTORS AFFECTING OUTCOME
FLOWCHART 4: Prognostic Factors
PROGNOSIS OF CONTACT GRANULOMA
│
┌────────┴──────────┐
│ │
FAVORABLE POOR
PROGNOSIS PROGNOSIS
│ │
├─ Intubation type ├─ Idiopathic/voice abuse type
├─ Female sex ├─ Male sex
├─ Smaller size ├─ Large lesion (lobulated)
├─ Unlobulated ├─ Bilaterality
├─ Early treatment ├─ Continued voice abuse
├─ Good compliance ├─ Uncontrolled LPR
└─ Short duration ├─ Delayed/inadequate treatment
└─ Surgical excision (high recurrence)
Pan et al. (Laryngoscope Investig ORL, 2022) developed
the RCGSG score for prognosis prediction:
Reflux / Coughing / Granuloma size / Sex / Globus
(PMID 36544923)
COMPLICATIONS
- Airway compromise - large posterior granuloma may obstruct glottis, cause stridor
- Recurrence - especially post-surgical, even more refractory
- Arytenoid perichondritis - in severe, untreated cases
- Posterior glottic stenosis - rare, following repeated trauma/surgery
- Voice deterioration - persistent dysphonia
- Bilateral involvement - may occur simultaneously or after treatment of one side
RECENT ADVANCES (2020-2026)
1. Objective LPR Assessment
- Lee et al. (Laryngoscope, 2026): Objective assessment of LPR using hypopharyngeal multichannel intraluminal impedance (HMII) - more accurate than RFS for predicting LCG prognosis (PMID 41614236)
2. Expert Consensus on Management
- Wang et al. (J Voice, 2026): First Delphi consensus on LCG - LPR + mechanical injury = main causes; lifestyle modification = foundation; voice therapy reduces recurrence; surgery NOT first-line due to high recurrence (PMID 42140868)
3. Botulinum Toxin - Expanding Role
- Intralesional injection directly into granuloma base (in addition to TA muscle injection)
- Effective for refractory cases as reported by Wang et al. (CJEORL, 2024) (PMID 39449596)
4. Arytenoid Cartilage Calcification as Prognostic Marker
- Zhang et al. (J Voice, 2024): CT detection of arytenoid cartilage calcification predicts prognosis - greater calcification correlates with poorer response to conservative treatment (PMID 34629228)
5. RCGSG Prognostic Scoring
- Pan et al. (2022) developed and validated the RCGSG score incorporating Reflux, Coughing, Granuloma size, Sex, Globus - helps predict treatment outcomes and guide individualized therapy (PMID 36544923)
6. Treatment Sequence - Hormone Injection Superior
- Qiang et al. (Eur Arch ORL, 2024): Intralesional hormone injection + acid suppression > acid suppression alone (higher curative ratio, shorter healing time) (PMID 38206391)
7. Post-Radiotherapy LCG
- Mo et al. (Ann Transl Med, 2023): CG can occur after radiotherapy for nasopharyngeal carcinoma - new etiology being recognized; LPR exacerbated by radiation mucositis (PMID 36819488)
8. Laser Options
- KTP (532 nm), PDL (pulsed dye laser), CO2, Thulium lasers - all acceptable
- Awake unsedated laser laryngeal surgery now an option for selected cases (Scott-Brown's)
COMPARISON ACROSS STANDARD TEXTBOOKS
| Aspect | Dhingra/Hazarika | Cummings | Scott-Brown | K.J. Lee |
|---|---|---|---|---|
| Definition emphasis | Voice abuse + LPR | Behavioral + acid reflux | LPR + hyperfunction | All causes |
| Primary Rx | Voice rest + PPIs | Antireflux empirically | Reduce irritants + voice Rx | PPIs + vocal hygiene |
| Steroid injection | Yes (intralesional) | Depot + inhaled | Mentioned | Recommended |
| BoTox | Mentioned | Office procedure | Mentioned | First-line for refractory |
| Surgery | Last resort | Last resort; leave base | High recurrence | Last resort |
| Stroboscopy | Recommended | Essential | Essential | Helpful |
SUMMARY TABLE (Quick Revision)
| Feature | Details |
|---|---|
| Site | Vocal process of arytenoid cartilage |
| Histology | Granulation tissue + epithelial hyperplasia |
| Common in | Men (vocal abuse); Women (intubation) |
| Main causes | LPR + mechanical trauma (vocal abuse/intubation) |
| Key symptom | Posterolateral throat pain + referred otalgia |
| Laryngoscopy | Bilobed heaped-up lesion at vocal process |
| Diagnosis | Clinical + videoendostroboscopy |
| Biopsy | Only if atypical/suspicious |
| Natural history | Spontaneous resolution in 3-6 months possible |
| First-line Rx | PPIs (high dose) + Voice therapy |
| Second-line | Intralesional steroid injection |
| Third-line | Botulinum toxin TA injection |
| Last resort | Microlaryngoscopy + excision (leave base) |
| Key complication | High post-surgical recurrence |
REFERENCES
- Cummings CW et al. Cummings Otolaryngology Head and Neck Surgery, 7th ed. Elsevier, 2021. pp. 1124-1126. [Contact Ulcer or Granuloma; Intubation Granuloma]
- Gleeson MJ et al. Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th ed. CRC Press, 2018. pp. 7372-7420. [Arytenoid Granuloma]
- Lee KJ. Essential Otolaryngology, 10th ed. McGraw-Hill, 2019. pp. 922-923. [Contact Ulcer and Vocal Fold Granuloma]
- Dhingra PL. Diseases of ENT Head & Neck Surgery, 7th ed. Elsevier, 2018.
- Hazarika P. Textbook of ENT Head & Neck Surgery, 2nd ed.
- Stell PM, Maran AGD. Stell and Maran's Head and Neck Surgery, 4th ed. Butterworth-Heinemann.
- Wang J, Nie Q, Li J et al. Expert Consensus of China on Laryngeal Contact Granuloma: A Modified Delphi Study. J Voice 2026. [PMID 42140868]
- Qiang Y, Liu XH, Zhang QQ et al. The effectiveness of various treatment approaches for laryngeal contact granulomas. Eur Arch Otorhinolaryngol 2024;281(4). [PMID 38206391]
- Woo JH, Oh JH, Lim BW, Kim DY. Treatment Results of Vocal Process Granuloma: Intubation versus Contact Granuloma. Int Arch Otorhinolaryngol 2023;27:261-267. [PMID 37125377]
- Pan Y, Li J, Wang X et al. Prognosis of patients with laryngeal contact granuloma: Development and validation of RCGSG score. Laryngoscope Investig Otolaryngol 2022. [PMID 36544923]
- Pan Y, Li J, Zhang J et al. Thyroarytenoid botulinum toxin injection for refractory laryngeal contact granuloma. Am J Otolaryngol 2022. [PMID 35567839]
- Zhang S, Liu W, Zheng M. Noninvasive Detection of Arytenoid Cartilage Calcification using CT and Prediction of Prognosis in Laryngeal Contact Granuloma. J Voice 2024. [PMID 34629228]
- Lee HJ, Son SY, Kim SI et al. Objective Assessment of Laryngopharyngeal Reflux in Laryngeal Contact Granuloma. Laryngoscope 2026. [PMID 41614236]
RGUHS Examination Tip: For a 50-mark answer, cover: Definition + Synonyms (2 marks), Anatomy (3 marks), Etiopathogenesis with flowchart (8 marks), Histopathology (5 marks), Clinical features (5 marks), Diagnosis with diagnostic algorithm (8 marks), Laryngoscopy images/description (4 marks), Differential diagnosis (4 marks), Management with flowchart (10 marks), Recent advances (5 marks), and References (2 marks). Always draw the pathogenesis flowchart, the management algorithm, and the anatomy of the posterior larynx for maximum marks.
This is a shared conversation. Sign in to Orris to start your own chat.