Acute ischemia of lower limb
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute limb ischemia" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
acute limb ischemia lower extremity clinical presentation pallor
Reading File
Reading File
I have comprehensive information to write a detailed answer. Let me now compile everything.
Acute Ischemia of the Lower Limb
Definition
Acute limb ischemia (ALI) is defined as a sudden loss of limb perfusion (arterial occlusion with symptoms present for <2 weeks) resulting in a potential threat to limb viability. Irreversible muscle and nerve injury can occur after 6 hours of severe arterial insufficiency. The incidence is approximately 1.5 cases per 10,000 persons/year, with perioperative mortality of 20–40% and limb loss rates of 12–50%.
— Sabiston Textbook of Surgery, p. 2326
Etiology
1. Embolism (~80% of emboli originate in the heart)
| Cardiac Sources | Extracardiac Sources |
|---|---|
| Atrial fibrillation (most common) | Aortic/femoral/popliteal aneurysms |
| Acute MI / ventricular aneurysm | Atherosclerotic plaque rupture (microemboli) |
| Dilated cardiomyopathy | Paradoxical embolus via PFO |
| Prosthetic heart valves (0.6–2.3%/year) | — |
| Endocarditis, atrial myxoma | — |
Emboli lodge preferentially at arterial bifurcations where vessel caliber decreases. In the lower extremity, the order of frequency is: common femoral artery > iliac artery > aortic bifurcation (saddle embolus) > popliteal/tibioperoneal arteries.
2. In-situ Thrombosis
Occurs most commonly in:
- Pre-existing atherosclerotic vessels (at the site of plaque/stenosis)
- Thrombosed arterial bypass grafts (now the most common etiology overall, due to increased use of prosthetic conduits)
- Arterial aneurysms with mural thrombus
- Hypercoagulable states (polycythemia, antiphospholipid syndrome)
3. Other causes
- Arterial trauma / iatrogenic (catheter-related dissection or arterial puncture)
- Aortic dissection (intimal flap obstruction)
- Popliteal artery entrapment syndrome
- Low-flow states (shock, vasopressors)
Key distinction: A patient with NO prior PAD history and normal contralateral pulses → likely embolic. A patient with prior claudication, bypass surgery, or contralateral PAD → likely in-situ thrombosis. This distinction drives management.
— Goldman-Cecil Medicine; Harrison's 22e, p. 2218
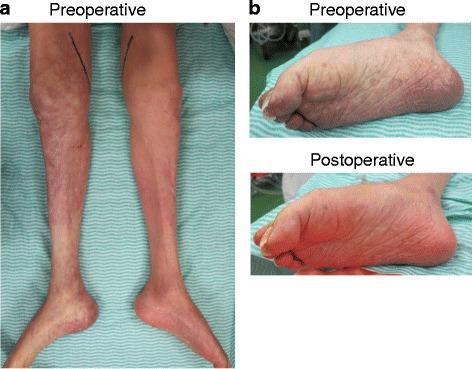
Clinical Features — The "6 Ps"
| Sign | Details |
|---|---|
| Pain | Sudden, severe; most common presenting symptom |
| Pallor | Cool, white/mottled skin |
| Pulselessness | Absent pulses distal to occlusion |
| Paresthesia | Early neurological sign — sensory loss in digits/foot |
| Paralysis | Late/severe sign — motor deficit; indicates urgent revascularization |
| Poikilothermia ("Perishing cold") | Limb temperature matches environment |
Onset is typically within 1 hour of the occlusion event. Paralysis and complete anesthesia indicate severe ischemia.
Rutherford Classification (Grading Severity)
| Category | Description | Sensory Loss | Motor Loss | Arterial Doppler | Venous Doppler |
|---|---|---|---|---|---|
| I — Viable | Not immediately threatened | None | None | Audible | Audible |
| IIa — Marginally threatened | Salvageable if promptly treated | Minimal (toes only)/none | None | Absent | Audible |
| IIb — Immediately threatened | Needs immediate revascularization | More than toes + rest pain | Mild–moderate | Absent | Audible |
| III — Irreversible | Major tissue loss/permanent nerve damage | Profound, anesthetic | Profound paralysis (rigor) | Absent | Absent |
— Sabiston Textbook of Surgery, Table 103.4
Category III (irreversible): Primary amputation is indicated. Revascularizing a non-viable limb in rigor risks reperfusion injury → multisystem organ failure and death.
Diagnosis
Clinical Assessment
- Compare with the contralateral limb
- Temperature demarcation line indicates level of occlusion
- Continuous-wave Doppler: absent arterial signal + audible venous → threatened but salvageable
- Palpable femoral pulse + absent distal pulses: occlusion at/below common femoral bifurcation
- Absent bilateral femoral pulses: saddle embolus at aortic bifurcation
Imaging
| Modality | Role |
|---|---|
| CTA | Fastest; guides open vs. endovascular approach; first-line in most centers |
| Duplex ultrasound | Confirms graft occlusion; no contrast; less useful for diffuse disease |
| Catheter arteriography | Gold standard; allows simultaneous intervention (CDT) |
| MRA | Alternative when contrast contraindicated |
Workup for Etiology
- ECG: Atrial fibrillation
- Echocardiogram (TTE/TEE): Cardiac thrombus, valvular disease, intracardiac shunt
- CT chest/abdomen/pelvis: Aortic aneurysm/dissection as embolic source
- Bubble echo: Paradoxical embolus via PFO
Management
Immediate: Anticoagulation
As soon as ALI is suspected → IV unfractionated heparin bolus 75–100 units/kg, then infusion at 15–18 units/kg/min.
- Prevents thrombus propagation
- Maintains collateral vessel patency
- Alternative (if heparin contraindicated): direct thrombin inhibitors (argatroban [hepatic metabolism] or lepirudin [renal metabolism])
Revascularization Strategy
Three primary approaches — no high-quality evidence demonstrates superiority of one over another (Sabiston):
1. Catheter-Directed Thrombolysis (CDT) / Endovascular
- Indications: Rutherford I or IIa; high surgical risk; thrombotic etiology; distal emboli (normal femoral pulse, absent distal pulses)
- Agents: recombinant tPA, reteplase, tenecteplase
- Most effective when arterial occlusion is of recent onset
- Advantage: Can treat underlying stenosis found after clot lysis
- Disadvantage: Slower reperfusion; bleeding risk
- Absolute contraindications: Active bleeding, stroke or neurosurgery within 3 months, malignant intracranial tumor, hemorrhagic stroke history, recent GI bleed
2. Open Surgical Thromboembolectomy (Fogarty catheter)
- Indications: Rutherford IIb (immediately threatened limb)
- Balloon-tipped Fogarty catheters passed proximally and distally
- In pure embolic events, extraction may reveal a widely patent system
- In thrombotic disease: residual stenosis must be addressed (angioplasty, endarterectomy, or bypass)
3. Hybrid Approaches
- Combination of open embolectomy and intraoperative CDT/angioplasty
- Useful when multilevel disease or distal thrombus persists after surgical thrombectomy
Fasciotomy
Four-compartment fasciotomy of the lower leg should always be considered after revascularization, especially if ischemia time >6 hours, to prevent compartment syndrome from reperfusion edema.
Primary Amputation
Indicated for:
- Rutherford Category III (irreversible ischemia, rigor)
- Devastating tissue loss combined with non-ambulatory status or poor overall health
Embolism vs. Thrombosis — Key Differences
| Feature | Embolism | Thrombosis |
|---|---|---|
| Onset | Acute, sudden | Acute-on-chronic |
| Prior PAD history | Absent | Present |
| Contralateral pulses | Normal | Abnormal |
| Cardiac history (AF, MI) | Common | Less common |
| Management | Fogarty embolectomy | Thrombolysis + treat underlying lesion |
| Collaterals | Poor (no time to develop) | Better (pre-existing) |
Complications
| Complication | Mechanism |
|---|---|
| Reperfusion injury | ROS release, Ca²⁺ influx, inflammatory cascade |
| Compartment syndrome | Reperfusion edema → elevated intracompartmental pressure |
| Hyperkalemia / myoglobinuria / AKI | Rhabdomyolysis from ischemic muscle necrosis |
| Multisystem organ failure | Revascularizing irreversible ischemia |
| Amputation | 12–50% in lower extremity ALI |
| Death | 20–40% perioperative mortality |
Recent Evidence (2025–2026)
Two recent systematic reviews and meta-analyses inform current practice:
- Endovascular vs. open surgery [PMID 41232816, J Vasc Surg 2026]: Endovascular approach in ALI — systematic review comparing outcomes between approaches.
- Thrombolytic vs. surgical [PMID 40428785, Medicina 2025]: Meta-analysis comparing thrombolytic therapy to open surgical interventions for ALI.
These reinforce that no single approach is universally superior — individualized decision-making based on Rutherford category, etiology, ischemia duration, and patient comorbidities remains the standard.
Sources: Sabiston Textbook of Surgery, 21st ed., pp. 2325–2328 | Harrison's Principles of Internal Medicine, 22e, pp. 2218–2219 | Goldman-Cecil Medicine, 27e | Schwartz's Principles of Surgery, 11th ed., pp. 980–982
This is a shared conversation. Sign in to Orris to start your own chat.