CN you explain about ulcerative colitis and other
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ulcerative colitis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full answer.
Ulcerative Colitis (UC) - Comprehensive Overview
What Is It?
Ulcerative colitis is a chronic idiopathic inflammatory disease of the colon, most commonly affecting adults in their third to fourth decades of life. It is characterized by a lifelong relapsing and remitting course. Unlike Crohn disease, it is confined exclusively to the colon and rectum, and the inflammation is continuous (no skip lesions) and mucosal/superficial (not transmural).
- Yamada's Textbook of Gastroenterology, p. 1248
Epidemiology
- Peak age of onset: 20-40 years, with a smaller second peak beyond age 70
- Equal sex distribution (F:M = 1:1)
- Highest incidence: Western Europe, North America
- Still rising in Eastern Europe, Asia, and the developing world
- About 15% of patients ultimately require colectomy for medically refractory disease or colorectal cancer
Phenotypes by Extent (Montreal Classification)
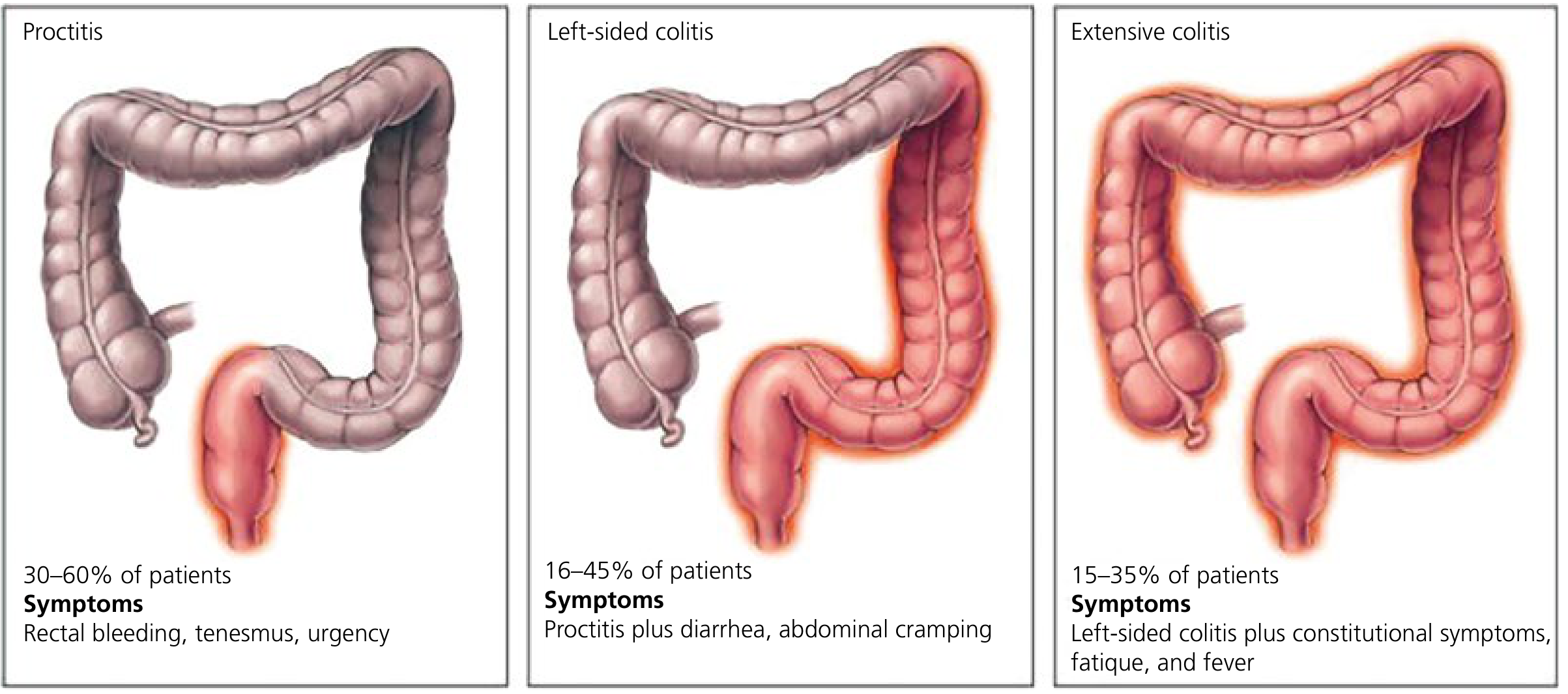
Figure: Ulcerative colitis phenotypes by the Montreal Classification - Yamada's Textbook of Gastroenterology
| Phenotype | % of Patients | Symptoms |
|---|---|---|
| Proctitis (rectum only) | 30-60% | Rectal bleeding, tenesmus, urgency |
| Left-sided colitis (to splenic flexure) | 16-45% | Above + diarrhea, abdominal cramping |
| Extensive/Pancolitis | 15-35% | Above + constitutional symptoms, fatigue, fever |
Pathogenesis
UC is multifactorial, involving:
- Genetic predisposition - multiple susceptibility loci identified
- Dysregulated immune response - predominantly Th17 and Th2 activation; up to 75% of UC patients have perinuclear antineutrophil cytoplasmic antibodies (p-ANCA)
- Epithelial barrier dysfunction - loss of mucosal barrier integrity
- Gut microbiome dysbiosis - reduced microbial diversity and altered microbial populations
- Environmental triggers - infectious enteritis may precede disease onset in some cases
Robbins notes that all current IBD therapies (from corticosteroids to biologics) target the immune system. Therapies effective in Crohn disease are generally also effective in UC.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 747
- Goldman-Cecil Medicine, p. 1481
Gross and Histological Pathology
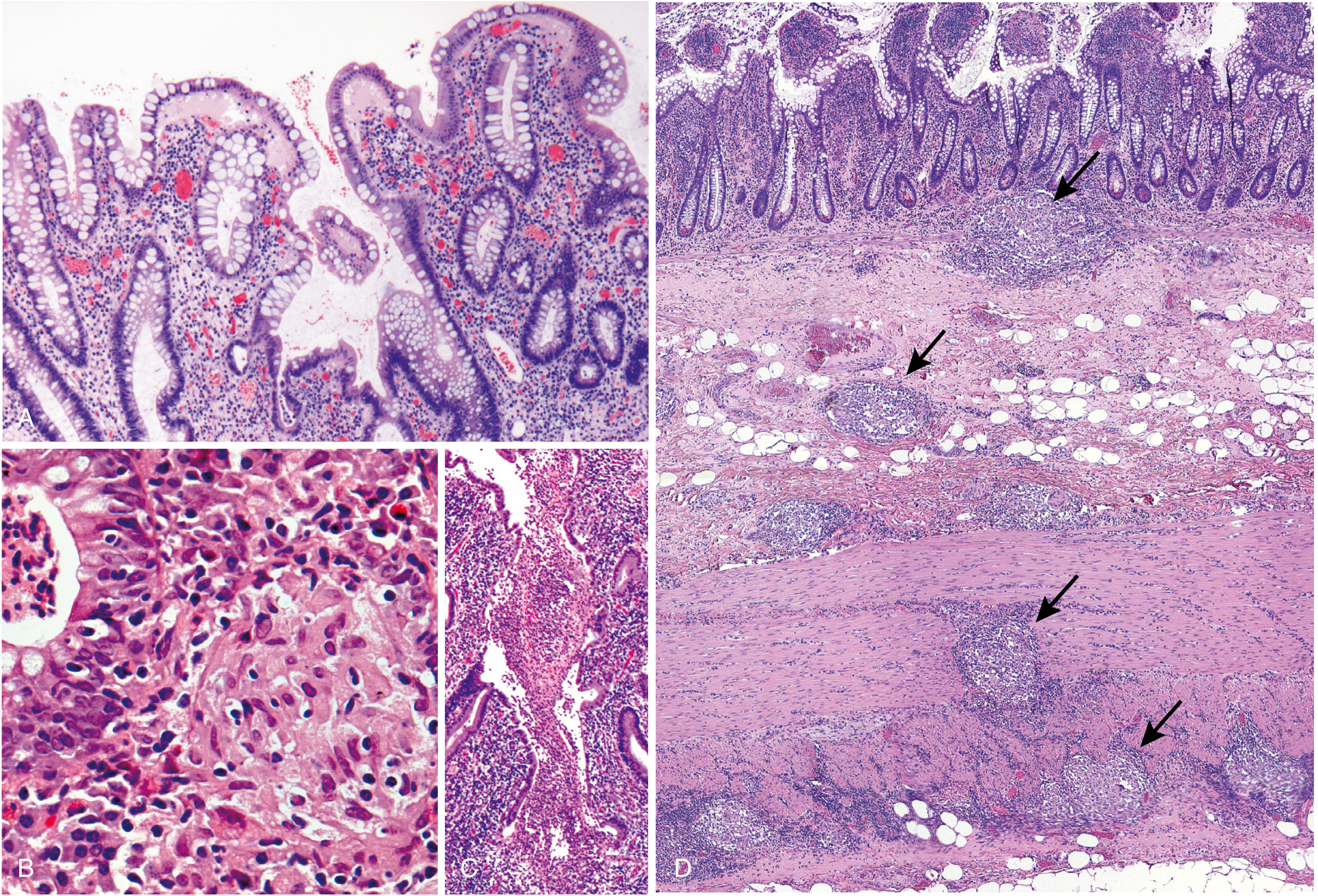
Microscopic pathology of IBD: (A) Haphazard crypt organization, (B) Noncaseating granuloma (Crohn only), (C) Active disease with ulceration, (D) Transmural inflammation in Crohn disease (arrows) - Robbins Pathology
Gross Findings:
- Always involves the rectum, extends proximally in a continuous fashion
- Ranges from red, granular mucosa to extensive broad-based ulcers
- Pseudopolyps form from regenerating mucosa (marker of more severe disease)
- No skip lesions, no transmural thickening, no serosal involvement
- Chronic disease: mucosal atrophy, colon shortening, loss of haustra ("lead pipe" appearance)
- Backwash ileitis: mild terminal ileal inflammation in severe pancolitis (not true ileal disease)
Histological Findings:
Early/Acute:
- Epithelial necrosis
- Acute inflammatory infiltrate in the lamina propria
- Cryptitis and crypt abscesses
Chronic:
-
Predominant lymphocytic infiltrate
-
Crypt architectural distortion
-
Paneth cell metaplasia, pseudopyloric metaplasia
-
Inflammation generally limited to mucosa and superficial submucosa
-
No granulomas (granulomas = Crohn disease)
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 747-748
-
Goldman-Cecil Medicine, p. 1481
Clinical Manifestations
Symptoms:
- Bloody diarrhea (cardinal symptom)
- Stringy mucoid material in stool
- Lower abdominal cramping, temporarily relieved by defecation
- Tenesmus (urgent, painful urge to defecate)
- Constitutional symptoms (fever, fatigue, weight loss) in severe disease
Disease Severity:
- More than half of patients have clinically mild disease
- Almost all experience at least one relapse within 10 years
- The initial attack may occasionally be a medical/surgical emergency
Diagnosis
Endoscopy (Gold Standard):
- Diffuse mucosal erythema with loss of normal vascular pattern
- Granular, edematous, friable mucosa (bleeds on contact)
- Ulceration in severe disease
- Findings start in the rectum and extend proximally in a continuous pattern
Histopathology:
- Crypt distortion + continuous mucosal inflammation from rectum
- Absence of granulomas
- Absence of small bowel disease
Lab Findings:
- Anemia - from blood loss, chronic disease, or nutritional deficiency (iron, folate, B12)
- Elevated WBC, ESR, and CRP in active disease
- Fecal calprotectin - elevated in active disease, lower in remission
- Hypoalbuminemia in severe/active disease
Serologic Markers:
| Marker | UC | Crohn's Disease |
|---|---|---|
| p-ANCA | 55% | 20% |
| ASCA (IgA + IgG) | <15% | 40-70% |
pANCA-positive + ASCA-negative favors UC; the reverse favors Crohn disease.
- Goldman-Cecil Medicine, p. 1483-1484
Treatment
Mild-Moderate UC:
| Drug Class | Examples | Use |
|---|---|---|
| 5-Aminosalicylates (5-ASA) | Mesalamine, sulfasalazine | First-line for mild-moderate UC; induction & maintenance |
| Corticosteroids | Prednisone, budesonide | Induction of remission; NOT for maintenance |
| Immunomodulators | Azathioprine (2-3 mg/kg/day), 6-mercaptopurine, methotrexate | Maintenance of remission (slow onset, months to work) |
Moderate-Severe UC (Biologics):
| Drug | Class | Mechanism |
|---|---|---|
| Infliximab, adalimumab | Anti-TNF-α | Inhibit TNF-mediated inflammation |
| Vedolizumab | Anti-α4β7-integrin | Blocks gut lymphocyte trafficking |
| Ustekinumab | Anti-IL-12/23 | Inhibits Th1 and Th17 activation |
| Risankizumab | Anti-IL-23 | Inhibits Th17 pathway |
| Tofacitinib | JAK inhibitor | Disrupts cytokine signaling |
Up to 50% of patients ultimately become unresponsive to their first anti-TNF biologic and may require a switch.
Surgery:
-
Colectomy is curative for intestinal disease in UC (unlike Crohn disease)
-
Indicated for: medically refractory disease, colorectal cancer, toxic megacolon, perforation
-
~15% of patients require colectomy
-
Note: extraintestinal manifestations may persist even after colectomy
-
Goldman-Cecil Medicine, p. 1484-1487
Complications
Local Complications:
| Complication | Notes |
|---|---|
| Toxic megacolon | Severe life-threatening dilation of colon; ~2-5% of patients with severe colitis |
| Perforation | Uncommon; associated with toxic megacolon |
| Massive hemorrhage | From severe mucosal ulceration |
| Strictures | Rare (unlike Crohn disease); any stricture in UC must be biopsied to rule out cancer |
| Colorectal cancer | Risk increases with duration and extent of disease; begins after 8-10 years of disease |
Colorectal Cancer Risk:
- Risk is elevated with: pancolitis, longer disease duration, concurrent primary sclerosing cholangitis
- Surveillance colonoscopy is recommended starting 8 years after diagnosis
- Dysplasia on biopsy is the key surveillance target
Extraintestinal Manifestations (EIM):
These can precede intestinal symptoms and may persist even after colectomy:
| System | Manifestations |
|---|---|
| Joints | Migratory polyarthritis, sacroiliitis, ankylosing spondylitis |
| Eyes | Uveitis, episcleritis |
| Skin | Erythema nodosum, pyoderma gangrenosum |
| Liver/Biliary | Primary sclerosing cholangitis (PSC) - most strongly associated with UC (~5% of UC patients have PSC; conversely, the majority of PSC patients have UC) |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 747-748
UC vs. Crohn Disease - Key Differences
| Feature | Ulcerative Colitis | Crohn Disease |
|---|---|---|
| Location | Colon and rectum ONLY | Esophagus to anus |
| Pattern | Continuous, no skip lesions | Skip lesions |
| Depth | Mucosal/superficial | Transmural |
| Ulcer type | Continuous | Discrete/serpentine |
| Fistulas | Rare/absent | Common |
| Strictures | Rare | Common |
| Granulomas | Absent | Present (noncaseating) |
| Perianal disease | Absent | Common |
| p-ANCA | 55% positive | 20% positive |
| ASCA | <15% | 40-70% |
| PSC association | Strong (~5%) | Weaker |
| Curative surgery | YES (colectomy) | NO |
Summary
Ulcerative colitis is a chronic, relapsing inflammatory disease of the colon with a continuous pattern starting from the rectum. It is diagnosed by endoscopy and histology (crypt abscesses, no granulomas), managed with a step-up approach from 5-ASAs to biologics, and carries a real risk of colorectal cancer requiring long-term surveillance. Unlike Crohn disease, it can be cured by colectomy, though extraintestinal manifestations may persist.
- Goldman-Cecil Medicine International Edition, p. 1481-1488
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 746-749
- Yamada's Textbook of Gastroenterology, 7th ed., p. 1248-1293
This is a shared conversation. Sign in to Orris to start your own chat.