Varicella pneumonia full details for md exams 10 marks answer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"varicella pneumonia" AND pathogenesis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough, MD-exam-quality answer.
Varicella Pneumonia - Comprehensive MD Exam Answer (10 Marks)
1. Introduction / Definition
Varicella pneumonia is the most serious pulmonary complication of primary varicella-zoster virus (VZV) infection. While chickenpox is a benign, self-limited illness in healthy children, pneumonia is the major severe complication in adults, where it occurs with an estimated 25-fold higher frequency than in children. It complicates approximately 1 in 400 cases of adult chickenpox infections.
2. Aetiology / Causative Agent
- Pathogen: Varicella-zoster virus (VZV) - a double-stranded DNA virus belonging to the Herpesviridae family (Human Herpesvirus 3)
- Primary VZV infection produces varicella (chickenpox); reactivation produces herpes zoster (shingles)
- The virus is highly contagious; transmitted by respiratory droplets and direct contact with skin lesions
3. Epidemiology & Risk Factors
| Risk Group | Details |
|---|---|
| Healthy adults | ~1 in 400 chickenpox cases; smoking is an independent risk factor |
| Pregnant women | Third trimester carries highest risk; pre-antiviral mortality 35-40% |
| Immunocompromised | HIV/AIDS, leukaemia, lymphoma, transplant recipients - greatest risk of visceral dissemination |
| Smokers | Significant independent risk factor |
| Children with malignancy | Before effective antivirals, ~7% of children with cancer died from VZV complications |
- HIV/AIDS patients with chickenpox are at especially high risk for varicella pneumonia
- Pre-vaccine era: 15-30% of invasive group A streptococcal infections were associated with varicella
4. Pathogenesis
VZV spreads initially via the respiratory tract. After primary replication in the nasopharynx, the virus undergoes two rounds of viremia:
- Primary viremia - virus disseminates from infected lymphocytes/monocytes
- Secondary viremia - more extensive dissemination producing the characteristic rash
Pulmonary involvement occurs via haematogenous seeding of the lungs, producing:
- Multicentric haemorrhage and necrosis centred on airways
- Focal areas of necrosis with intranuclear inclusion bodies (Cowdry type A inclusions) in pneumocytes
- Interstitial pneumonitis with mononuclear cell infiltration
- Fibrin-rich oedema fluid filling alveolar spaces
- Multinuclear giant cells (especially in immunocompromised hosts)
In immunocompromised patients: continued viral replication and prolonged viremia lead to more extensive visceral involvement.
5. Clinical Features
Onset: 1 to 6 days after appearance of the varicella rash (occasionally concurrent with rash)
Symptoms (in order of frequency):
- Cough (often dry, non-productive initially)
- Dyspnoea and tachypnoea
- High fever - can persist or worsen despite skin lesion resolution
- Pleuritic chest pain
- Haemoptysis (may be present)
- Cyanosis (indicates severe disease)
Key exam point: "The severity of symptoms usually exceeds the physical findings" - physical examination of the chest may be relatively normal despite severe radiological changes.
Signs:
- Tachycardia, tachypnoea
- Bilateral crackles on auscultation
- Typical varicella rash in various stages ("dewdrops on rose petals" - vesicles to pustules to crusts simultaneously present)
- The intensity of the rash does not necessarily correlate with severity of pneumonia
6. Investigations
A. Chest X-Ray
- Diffuse peribronchial nodular densities throughout both lung fields
- Concentrating in the perihilar regions and at the lung bases
- Bilateral infiltrates; hilar adenopathy may be present
- Pleural effusions can occur
B. HRCT Chest (most sensitive)
Thin-section CT reflects multicentric haemorrhage and necrosis centred on airways:
- Numerous nodular opacities, 5-10 mm diameter, bilateral and randomly distributed
- Some nodules have a surrounding halo of ground-glass opacity
- Patchy ground-glass opacities
- Coalescence of nodules forming areas of consolidation
- Miliary distribution may occur
- Late/healed stage: well-defined, randomly scattered 2-3 mm densely calcified nodules (pathognomonic late finding)
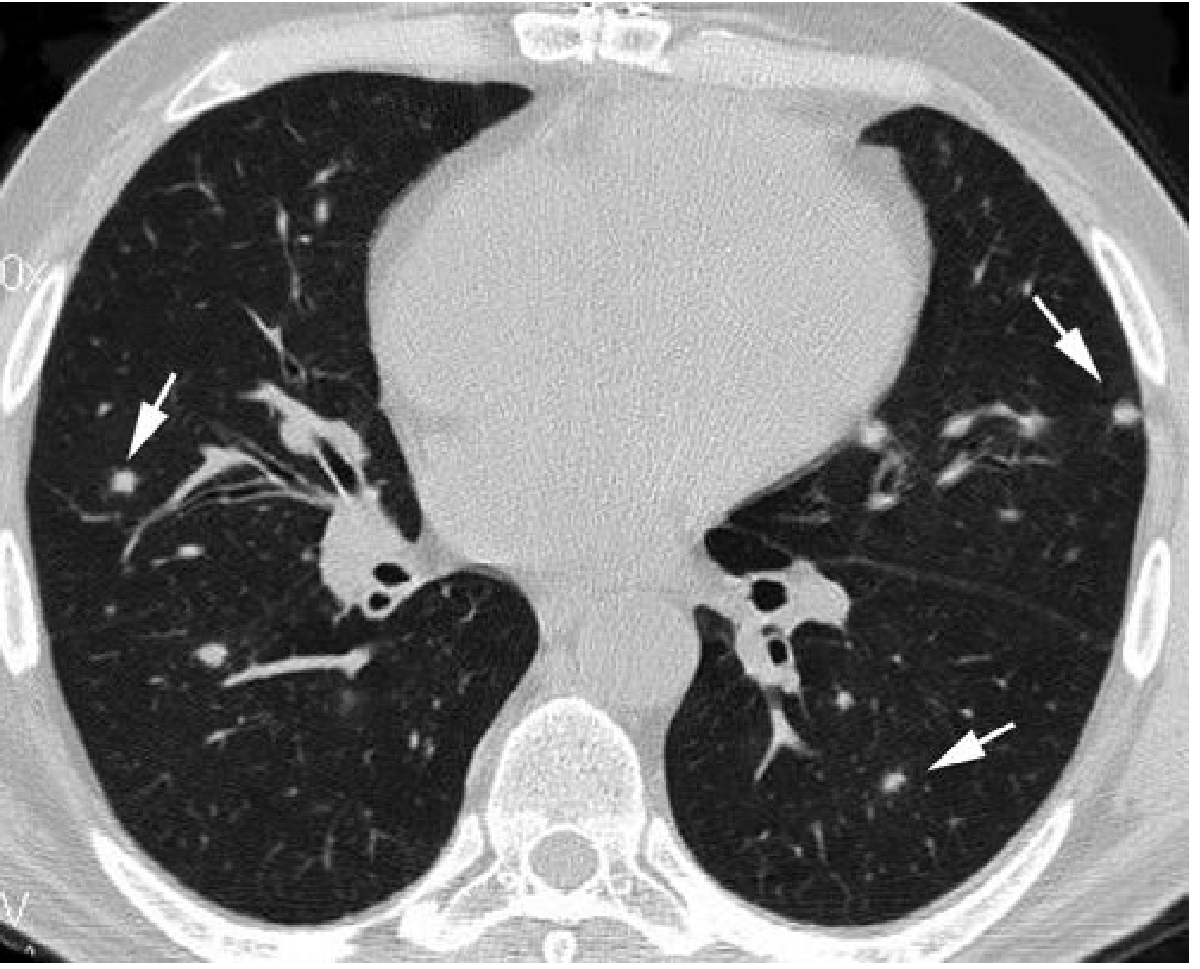
CT of the lower lobes in a 30-year-old man with lymphoma and varicella showing multiple bilateral randomly distributed well-defined small pulmonary nodules - from Grainger & Allison's Diagnostic Radiology
C. Pulmonary Function Tests
- Normal spirometric values but decreased carbon monoxide diffusing capacity (DLCO) - may persist for months after resolution
D. Laboratory Tests
- VZV PCR (blood, BAL fluid, skin lesion scraping - Tzanck smear)
- Serology: VZV IgM (acute), IgG (immunity)
- ABG: hypoxaemia (PaO2 reduced)
- FBC, LFTs (hepatitis may coexist in immunocompromised)
E. Bronchoscopy/BAL
- For diagnosis in immunocompromised or ventilated patients
- Cytology may show multinuclear giant cells with intranuclear inclusions
7. Histopathology
- Intranuclear inclusion bodies (Cowdry type A) in infected pneumocytes and alveolar macrophages
- Focal areas of necrobiosis (necrosis with surrounding inflammation)
- Alveolar haemorrhage and fibrin deposition
- Interstitial mononuclear cell infiltration
- Hyaline membrane formation in severe cases (diffuse alveolar damage pattern)
- Multinuclear giant cells with intranuclear inclusions (in immunocompromised)
8. Complications & Prognosis
| Complication | Notes |
|---|---|
| Respiratory failure / ARDS | Life-threatening; may require mechanical ventilation |
| Pulmonary infarction | May complicate the clinical picture |
| Secondary bacterial pneumonia | Staphylococci or Streptococci |
| Persistent DLCO reduction | Can persist months after clinical recovery |
| Late pulmonary calcification | Miliary calcified nodules - characteristic late CT finding |
Mortality:
- Healthy adults without treatment: 10-30%
- With prompt acyclovir therapy in immunocompetent adults: <10%
- Pregnant women (pre-antiviral era): 35-40%; reduced to 11-14% with acyclovir
- Immunocompromised patients: up to 50%
- Murray & Nadel quotes: "Mortality rate ranges from 11% in healthy adults to approximately 50% in pregnant women and immunocompromised persons"
9. Management
A. Antiviral Therapy (cornerstone)
IV Acyclovir is the standard of care for varicella pneumonia:
- Dose: 10 mg/kg every 8 hours IV (for 7-10 days or until clinical improvement)
- Initiated within 36 hours of hospitalisation - reduces fever, tachypnoea, and improves oxygenation
- All gravidas with varicella pneumonia should be aggressively treated with IV acyclovir and admitted to ICU
Oral antivirals (for uncomplicated adult varicella, not pneumonia):
- Acyclovir 800 mg 5x daily for 5-7 days
- Valacyclovir 1000 mg every 8 hours (more convenient)
- Famciclovir 500 mg every 8 hours
B. Supportive Care
- Hospitalisation - mandatory for varicella pneumonia
- Supplemental oxygen / High-flow oxygen
- ICU admission if hypoxaemia, respiratory failure, or need for mechanical ventilation
- Chest physiotherapy
- Monitor ABG, O2 saturation
C. Specific Situations
- Pregnant women: IV acyclovir + ICU admission; varicella-zoster immune globulin (VZIG) for post-exposure prophylaxis within 96 hours of exposure
- Immunocompromised: IV acyclovir within 72 hours of rash onset; controlled trials show decreased visceral complications; switch to oral therapy when new lesions stop appearing
D. Prophylaxis
- VZIG (Varicella-zoster immune globulin): Susceptible high-risk individuals (pregnant, immunocompromised) within 96 hours of exposure; reduces but does not abolish risk of infection
- Varicella vaccine (live attenuated): Pre-exposure prophylaxis in seronegative individuals; contraindicated in pregnancy and immunocompromised patients
E. Corticosteroids
- Data conflicting; cohort studies and literature reviews have not shown clear benefit and may cause harm - generally not recommended
10. Special Considerations
Varicella Pneumonia in Pregnancy
- Most dangerous in the third trimester
- Prior to acyclovir: maternal mortality 35-40% (vs. 11-17% in non-pregnant adults)
- Fetus at risk of: premature delivery, intrauterine death, congenital varicella syndrome (if maternal varicella occurs in first 20 weeks - risk ~1-2%)
- Perinatal varicella (within 10 days of birth) is particularly dangerous for the neonate
- Management: IV acyclovir + ICU monitoring; VZIG for exposed susceptible gravidas
Varicella Pneumonia in Immunocompromised
- Higher risk of visceral dissemination - prolonged fever, recurrent crops of lesions are warning signs
- Pneumonia, hepatitis, encephalitis, haemorrhagic complications may all co-occur
- Purpura fulminans with DIC is a feared complication
- Higher VZV viral loads; potentially resistant strains may emerge in severely immunosuppressed
Summary Table for Quick Revision
| Feature | Key Point |
|---|---|
| Causative agent | VZV (HHV-3), DNA virus, herpesviridae |
| Incidence in adults | 1 in 400 chickenpox cases |
| Onset after rash | 1-6 days |
| Hallmark symptom | Dyspnoea + cough with minimal chest signs |
| CXR finding | Diffuse peribronchial nodular densities, perihilar & basal |
| CT finding | 5-10 mm nodules ± GGO halo; late: calcified miliary nodules |
| PFT finding | Normal spirometry but reduced DLCO |
| Treatment | IV Acyclovir 10 mg/kg q8h |
| Mortality (adult, treated) | <10% |
| Mortality (pregnant, untreated) | 35-40% |
| Prophylaxis | VZIG within 96 hrs; vaccine contraindicated in pregnancy |
Sources: Fishman's Pulmonary Diseases and Disorders | Fitzpatrick's Dermatology | Grainger & Allison's Diagnostic Radiology | Murray & Nadel's Textbook of Respiratory Medicine | Creasy & Resnik's Maternal-Fetal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.