Importance of Fasting n post prandial insulin levels
Reading File
Finding Sources
Finding Sources
Searching PubMed
"fasting insulin" AND "postprandial insulin" AND clinical significance
Finding Sources
Finding Sources
Searching PubMed
"insulin resistance" AND "fasting insulin" AND diabetes
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have rich content from multiple authoritative textbooks. Here is a comprehensive answer:
Fasting and Postprandial Insulin Levels: Clinical Importance
1. Normal Insulin Physiology
Insulin is secreted by pancreatic beta cells and is the primary anabolic hormone governing glucose homeostasis. Its secretion is tightly regulated to maintain stable blood glucose during both fasting and feeding states, achieved through the coordinated interplay of circulating nutrients, GI hormones (incretins), pancreatic counter-regulatory hormones, and the autonomic nervous system.
Key synthesis facts:
- Synthesized as preproinsulin → processed to proinsulin → cleaved into insulin + C-peptide (secreted in equimolar amounts)
- Insulin half-life: 5-6 minutes (extensive hepatic and renal clearance); ~60% removed in the first pass through the liver
- C-peptide half-life: ~30 minutes - used clinically to assess beta-cell secretion and distinguish endogenous from exogenous insulin
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
2. Fasting Insulin Levels
Normal Values
- Healthy, non-obese adults after an overnight fast: 12-150 pmol/L (2-25 µIU/mL)
- With more specific assays (minimal proinsulin cross-reactivity): < 60 pmol/L (< 10 µIU/mL)
- Fasting insulin is higher in obese, non-diabetic individuals and lower in trained athletes
- Tietz Textbook of Laboratory Medicine, 7th Edition
Fasting State Physiology
In the fasting state, declining glucose concentrations inhibit insulin release, which results in:
- Increased glycogenolysis and gluconeogenesis in the liver
- Release of glucose into the circulation to maintain euglycemia
- At very low insulin concentrations: inhibition of lipolysis and ketone production is lifted, enabling fatty acid mobilization for energy
When insulin deficiency occurs (absolute or relative), unrestrained hepatic glucose production leads to fasting hyperglycemia - the hallmark of early type 2 diabetes. Even at the lowest concentrations, basal insulin continues to inhibit lipolysis, preventing excessive ketosis.
- Goldman-Cecil Medicine, 26th Edition
3. Postprandial Insulin Response
The Biphasic Pattern
A rapid rise in blood glucose (as after a meal) triggers two distinct phases of insulin secretion:
| Phase | Timing | Source | Significance |
|---|---|---|---|
| First phase | Peaks within 2-5 minutes | Preformed insulin granules at the plasma membrane | Immediate suppression of hepatic glucose output |
| Second phase | Sustained as long as glucose remains elevated | Newly synthesized + mobilized granules | Drives peripheral glucose uptake |
The earliest pathophysiologic indicator of defective beta-cell function is loss of first-phase insulin secretion - this precedes overt glucose intolerance or diabetes by years.
- Goldman-Cecil Medicine; Tietz Textbook of Laboratory Medicine
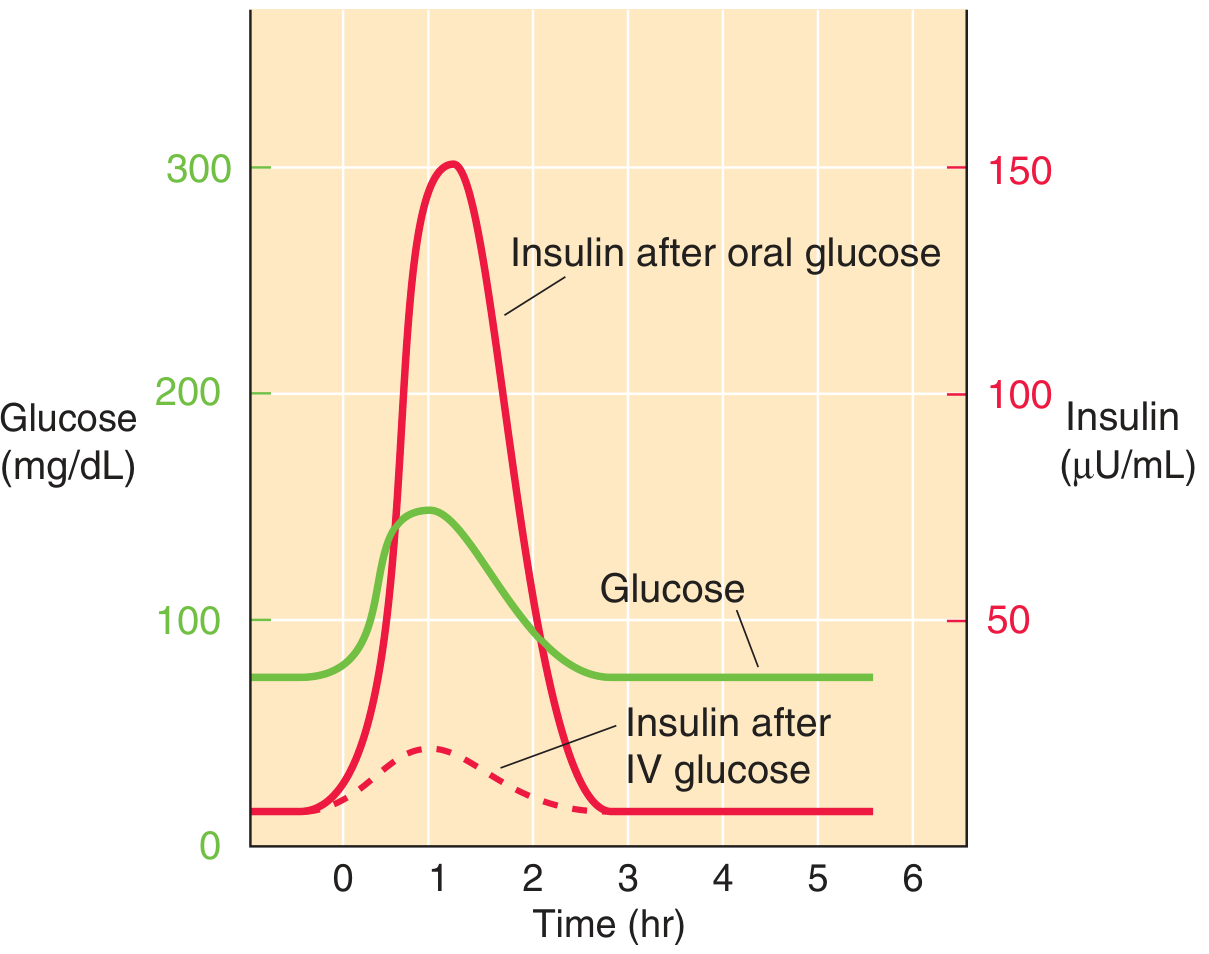
The graph shows that oral glucose triggers a much larger postprandial insulin response than the same glucose dose given intravenously - this is the incretin effect. Postprandial insulin peaks around 1 hour after oral glucose ingestion and returns to baseline by 2-3 hours.
The Incretin Effect
Oral glucose produces substantially greater insulin secretion than the same amount given intravenously - the "incretin effect." This is due to gut-derived hormones:
- GLP-1 (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide) account for up to 70% of postprandial insulin secretion
- These hormones are secreted from the duodenum and proximal jejunum in response to food
The blunted incretin effect in type 2 diabetes is a therapeutic target: GLP-1 receptor agonists and DPP-4 inhibitors exploit this pathway.
- Tietz Textbook of Laboratory Medicine; Goldman-Cecil Medicine
Postprandial Insulin Actions
After meals, insulin concentration rises progressively, with sequential metabolic effects:
- Lowest concentrations: Inhibit lipolysis, suppress ketone production
- Moderate rise: Lower hepatic glucose production by inhibiting glucagon; stop further glucose rise
- Further increase: Drive peripheral glucose uptake into skeletal muscle and adipose tissue; promote protein and triglyceride synthesis
- Highest concentrations: Stimulate hepatic glycogen synthesis and amino acid uptake
- Goldman-Cecil Medicine, Table 210-2
4. Clinical Importance of Fasting Insulin
A. Marker of Insulin Resistance
Fasting insulin concentration serves as a surrogate marker of insulin resistance. A high fasting insulin alongside normal or borderline-high fasting glucose signals the body is compensating via hyperinsulinemia. This is measured by the HOMA-IR (Homeostasis Model Assessment of Insulin Resistance):
HOMA-IR = [Fasting Glucose (mmol/L) × Fasting Insulin (µIU/mL)] ÷ 22.5
A simpler and clinically accessible tool than the euglycemic clamp, though with limitations in precision.
- Tietz Textbook of Laboratory Medicine; Brenner & Rector's The Kidney
B. Elevated Fasting Insulin in Type 2 Diabetes
- Type 2 diabetics can have elevated fasting insulin due to higher fasting glucose levels and peripheral insulin resistance
- Up to 10-20% of measurable plasma insulin is actually proinsulin in type 2 diabetics (vs. 2-4% in healthy subjects) - proinsulin has attenuated glucose-lowering effect, so absolute insulin values overestimate functional capacity
- Progressive beta-cell failure eventually causes fasting insulin to fall, marking disease progression
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
C. Metabolic Syndrome Diagnosis
The insulin resistance syndrome (Metabolic Syndrome / Syndrome X) is identified by the cluster of:
- Hyperinsulinemia (elevated fasting insulin)
- Obesity (especially central/visceral)
- Dyslipidemia (high triglycerides, low HDL)
- Hypertension
- Elevated fasting plasma glucose (≥100 mg/dL)
Individuals with this syndrome have a significantly increased cardiovascular disease risk.
- Tietz Textbook of Laboratory Medicine
5. Clinical Importance of Postprandial Insulin
A. Diagnosing Beta-Cell Dysfunction Early
Loss of first-phase postprandial insulin secretion is the earliest detectable sign of beta-cell failure and insulin secretory abnormality, appearing years before clinical diabetes. This can be assessed by IV glucose tolerance test or OGTT-derived insulin indices.
B. Role in Postprandial Hyperglycemia
Insufficient postprandial insulin response has two mechanisms leading to high postprandial glucose:
- Inadequate peripheral glucose uptake (predominantly skeletal muscle) - main driver
- Impaired suppression of hepatic glucose production (hepatic insulin resistance) - also contributes
- Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine
C. Reactive (Postprandial) Hypoglycemia
Delayed timing of insulin release after a meal can cause reactive hypoglycemia: beta cells release too much insulin too late, causing blood glucose to initially spike then fall rapidly. This can be an early sign of metabolic dysfunction and may herald the development of diabetes mellitus.
- Medical Physiology (Boron & Boulpaep)
D. Insulin Resistance Pattern Recognition
| Tissue | Effect of Insulin Resistance | Consequence |
|---|---|---|
| Liver | Failure to inhibit gluconeogenesis | High fasting blood glucose |
| Skeletal muscle | Low glucose uptake and glycogen synthesis | High postprandial blood glucose |
| Adipose tissue | Failure to inhibit hormone-sensitive lipase | Excess FFAs → worsens insulin resistance + dyslipidemia |
- Robbins & Kumar Basic Pathology
6. Summary of Clinical Applications
| Parameter | What It Reflects | Clinical Use |
|---|---|---|
| Fasting insulin (elevated) | Insulin resistance / early compensation | HOMA-IR, metabolic syndrome screening |
| Fasting insulin (low) | Beta-cell failure or type 1 DM | Insulin deficiency assessment |
| Postprandial insulin (blunted 1st phase) | Early beta-cell dysfunction | Early T2DM detection |
| Postprandial insulin (delayed/excess) | Reactive hypoglycemia risk | Functional glucose dysregulation |
| C-peptide (fasting/stimulated) | Endogenous beta-cell secretion | Distinguish T1 vs T2 DM; assess residual beta-cell mass |
Key takeaways:
- Fasting insulin reflects the basal state of insulin resistance and hepatic glucose regulation; elevated fasting insulin is the hallmark of compensated insulin resistance
- Postprandial insulin reflects beta-cell secretory capacity and incretin response; its loss (especially first-phase) is the earliest indicator of impending diabetes
- Both measurements together, particularly in the OGTT context, give a more complete picture of beta-cell reserve and peripheral sensitivity than either alone
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Tietz Textbook of Laboratory Medicine, 7th Ed.; Medical Physiology (Boron & Boulpaep); Goldman-Cecil Medicine, 26th Ed.; Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.