Clubbing
Reading File
Finding Sources
Searching PubMed
finger clubbing causes mechanisms
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of Digital Clubbing from the major medical textbooks:
Digital Clubbing
Definition
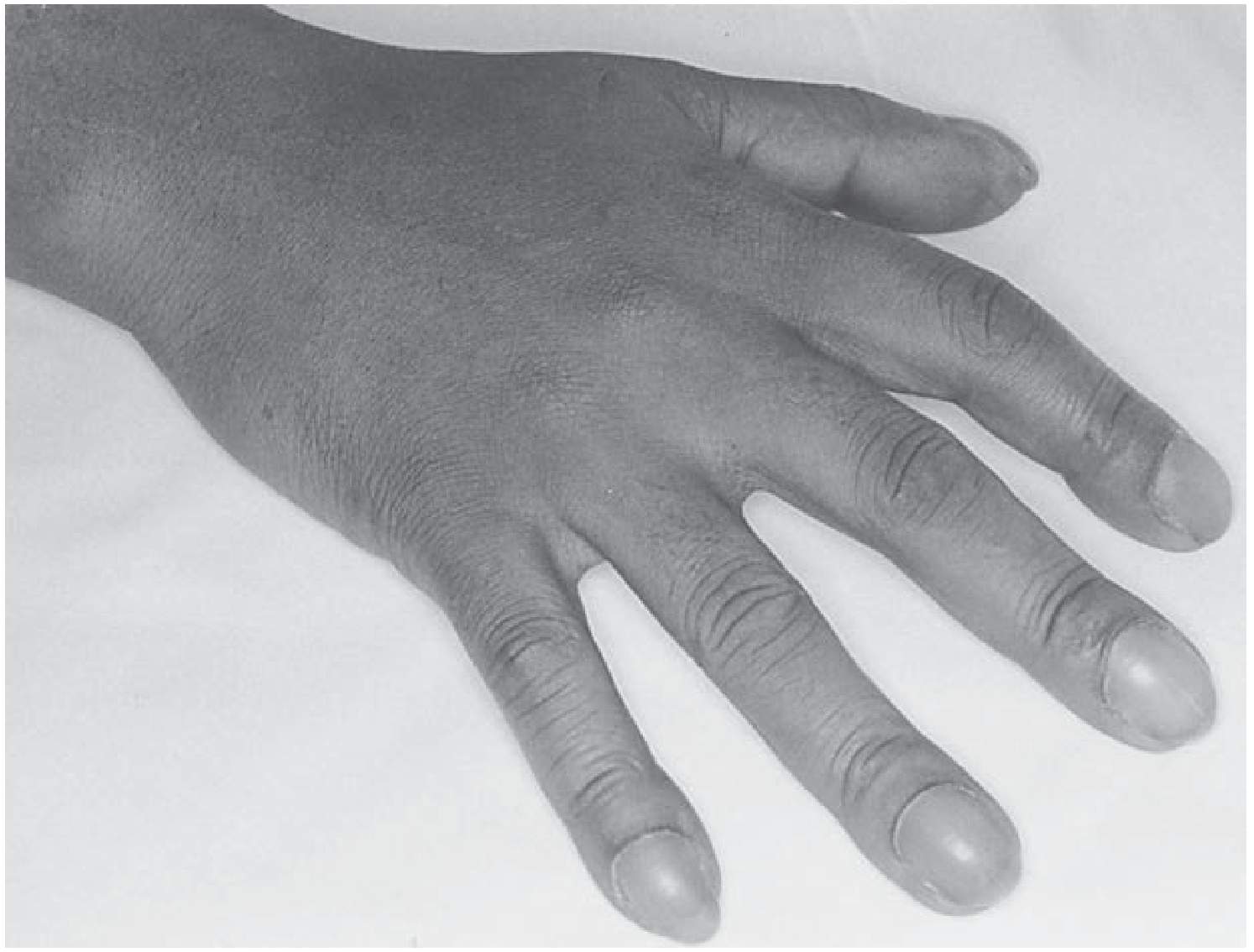
Clubbing is the selective bulbous enlargement of the distal segments of the digits (fingers and toes) due to proliferation of connective tissue - particularly on the dorsal surface - along with increased sponginess of the soft tissue at the nail base.
- Harrison's Principles of Internal Medicine 22E, p. 2602
Clinical Features (How to Recognize It)
Four hallmarks:
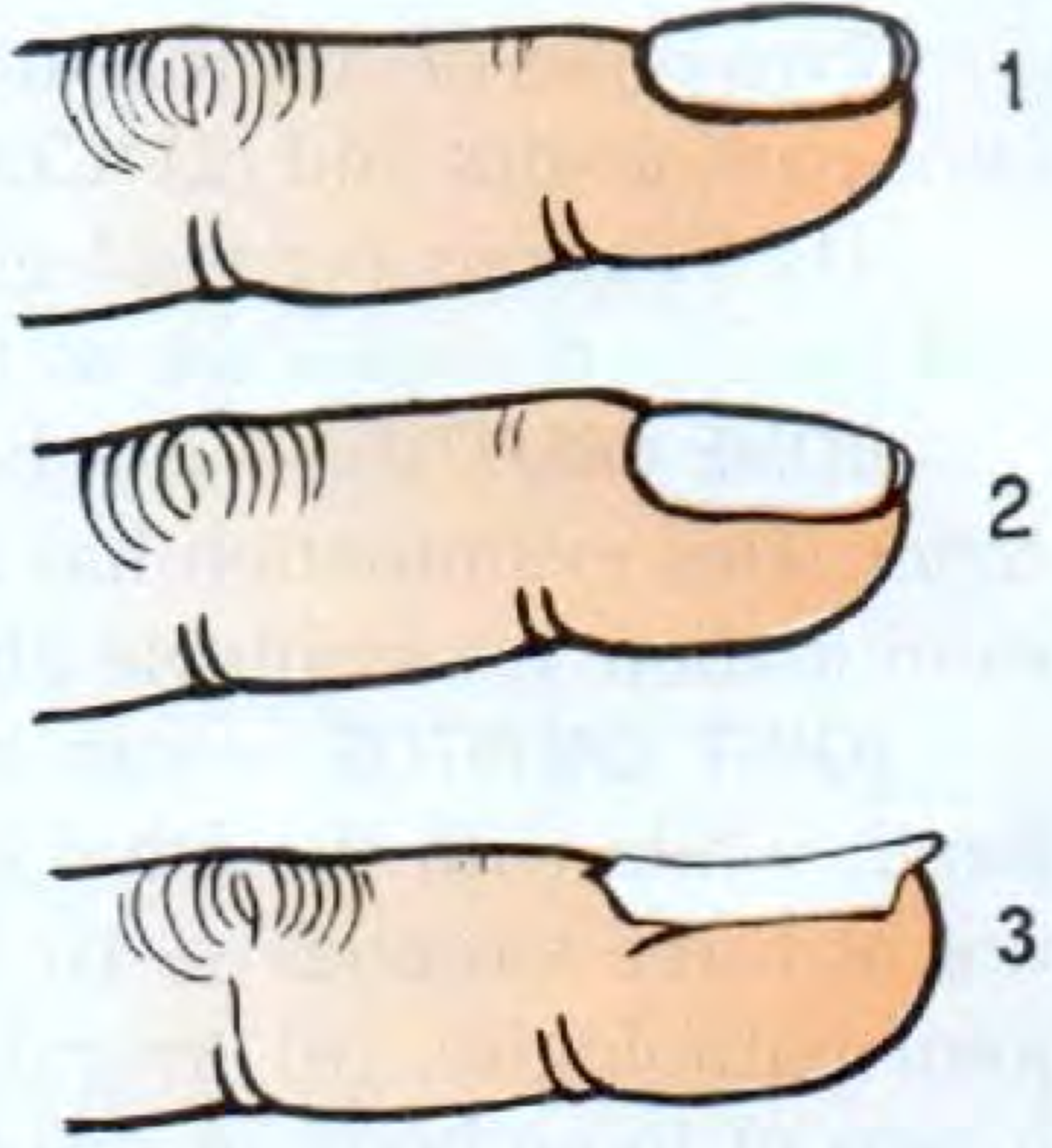
- Increased Lovibond angle - the normal ~165° angle between the nail plate and proximal nail fold flattens and exceeds 180°
- Nail base softening and sponginess - the nail appears to "float," perilingual erythema may be present
- Bulging/enlargement of the distal phalanx - may be warm and erythematous
- Nail curvature - nails curve in both longitudinal and coronal planes (drumstick appearance)
The straightening of the nail-cuticle angle is the most sensitive early sign.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 3782
Pathogenesis
The exact mechanism is unknown, but the leading theory involves vasodilation of vessels in the fingertip with arteriovenous connections, raising hydrostatic pressure in capillaries and venules, which drives fluid into the interstitium causing soft tissue swelling.
Histochemically, clubbed digits show increases in:
- Vascular endothelial growth factor (VEGF)
- Platelet-derived growth factor (PDGF)
- Hypoxia-inducible factor-1α and -2α
- Microvessel density in the stroma
A popular theory is that a humoral substance escapes normal deactivation in the pulmonary capillaries (or hepatic circulation), explaining the link to lung disease, cyanotic heart disease, and hepatic cirrhosis. Shunting of blood past the capillary bed of the lung or liver appears to be a common denominator.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 3782; Fishman's Pulmonary Diseases, p. 4210
Causes
Pulmonary (most common):
- Lung cancer (primary or metastatic) - most important cause to exclude
- Bronchiectasis
- Cystic fibrosis
- Lung abscess / empyema
- Pulmonary fibrosis / asbestosis
- Sarcoidosis
- Tuberculosis
- Mesothelioma
- NOT caused by COPD - clubbing in a COPD patient should raise suspicion for a second process (usually lung cancer)
Cardiac:
- Cyanotic congenital heart disease (right-to-left shunts)
- Infective / subacute bacterial endocarditis
Gastrointestinal:
- Inflammatory bowel disease (Crohn's disease, ulcerative colitis)
- Hepatic cirrhosis
- Gastrointestinal neoplasms
- Polyposis of the colon
Other:
-
HIV in children
-
Hepatopulmonary syndrome
-
Benign asbestos pleural disease
-
Chronic mountain sickness
-
Occupational (jackhammer operators)
-
Hereditary / idiopathic / familial (dominant inheritance)
-
Drug-induced (e.g., voriconazole)
-
Harrison's Principles 22E, p. 2602; Fishman's Pulmonary Diseases, p. 4203; S Das Manual, p. 742
Special Distributions
| Pattern | Cause to Consider |
|---|---|
| Bilateral symmetric (hands + feet) | Usual pattern |
| Toes only | Patent ductus arteriosus with reversed shunt |
| One hand only | Ipsilateral pulmonary sulcus tumor, hemiplegia |
| Single finger | Local injury, median nerve injury |
Association with Hypertrophic Osteoarthropathy (HOA)
Clubbing can be accompanied by HOA - subperiosteal formation of new bone at the distal diaphyses of long bones (radius, ulna, tibia, fibula), causing painful swollen joints resembling arthritis affecting shoulders, knees, ankles, wrists, and elbows. HOA is most strongly linked to:
- Bronchogenic carcinoma (~5% incidence; small-cell carcinoma rarely involved)
- Other intrathoracic malignancies
- Cystic fibrosis
- Bronchiectasis, empyema, lung abscess
Diagnosis of HOA is confirmed by plain radiograph or MRI showing periosteal new bone formation.
- Fishman's Pulmonary Diseases, p. 4215-4219; Harrison's 22E, p. 2604
Clinical Significance
-
New-onset clubbing always warrants a chest radiograph and, if unrevealing, a CT scan to exclude a pulmonary neoplasm
-
Clubbing was found in 1% of all internal medicine admissions and was associated with serious disease in 40% of those patients
-
Clubbing can develop rapidly (~2 weeks in new-onset empyema) and can also reverse - for example, after corrective cardiac surgery or lung transplantation for cystic fibrosis
-
Murray & Nadel's, p. 3784; Harrison's 22E, p. 2606
This is a shared conversation. Sign in to Orris to start your own chat.