Is operation necessary in de quervein tenosynovitis
Reading File
Searching PubMed
de Quervain tenosynovitis treatment conservative surgery
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is the full, evidence-based answer:
Is Operation Necessary in De Quervain Tenosynovitis?
No - surgery is not necessary in the majority of cases. It is reserved only for patients who fail conservative management. The standard approach is stepwise, starting with the least invasive treatments.
Understanding the Condition
De Quervain tenosynovitis (DQT) is a stenosing tenosynovitis of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons within the first dorsal extensor compartment at the radial styloid. It most commonly affects women aged 30-50, new mothers (from repetitive ulnar deviation in newborn care), and racket-sport athletes. Women are affected 6-10 times more frequently than men.
Key clinical features:
- Pain and tenderness at the radial styloid
- Palpable thickening of the fibrous sheath
- Positive Finkelstein test (most pathognomonic objective sign)
Treatment Algorithm
The treatment follows a clear stepwise approach:
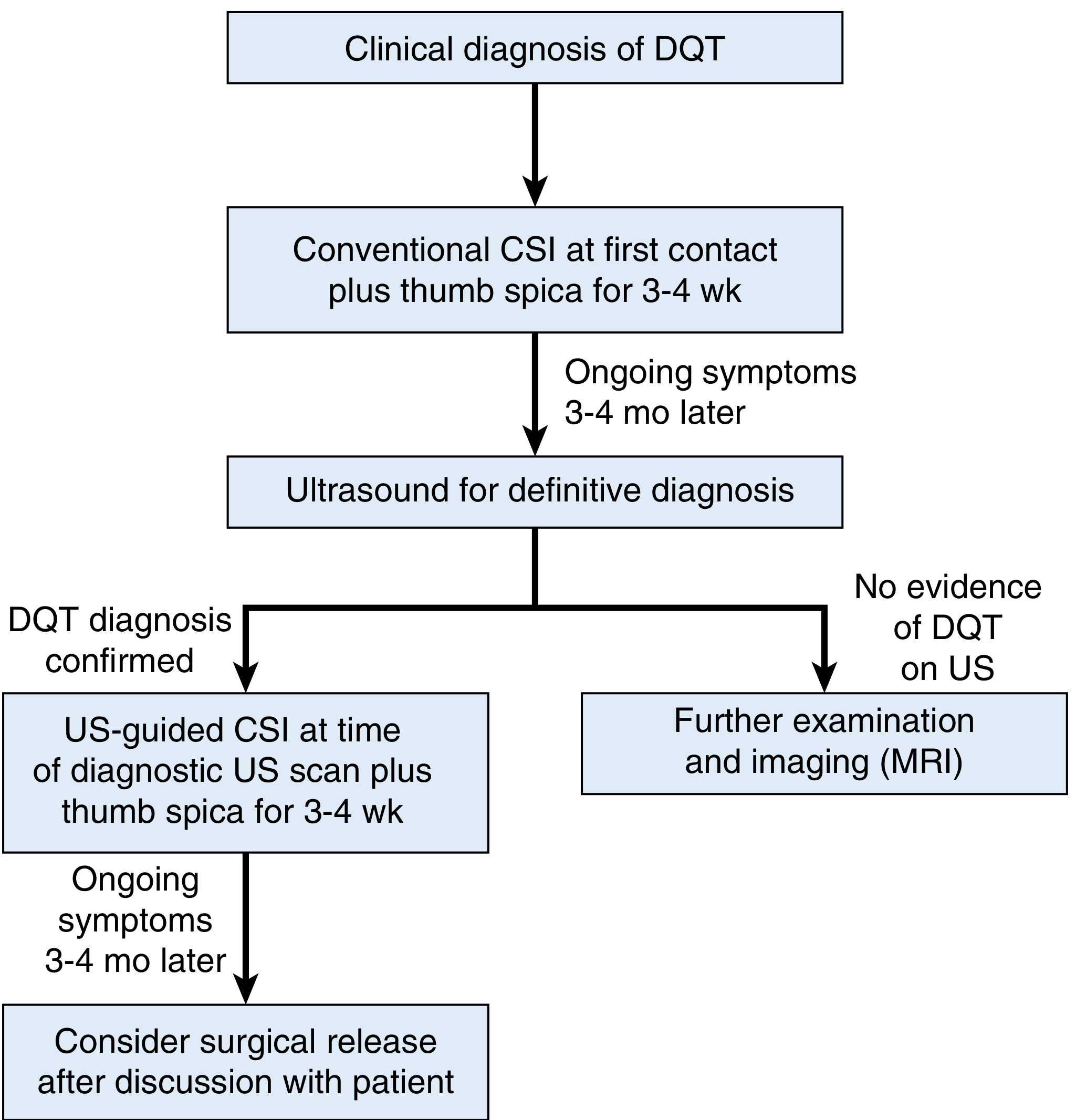
Step 1: Conservative (Non-operative) Treatment
This is always the first line:
| Measure | Details |
|---|---|
| Activity modification | Avoid repetitive gripping/ulnar deviation |
| Thumb spica splinting | Immobilizes the first dorsal compartment |
| NSAIDs | Reduces inflammation and pain |
| Corticosteroid injection | Most effective conservative option |
Corticosteroid injection is highly effective: Initial steroid injection yields complete pain relief in >70% of patients (Campbell's Operative Orthopaedics), with some studies reporting success in >80% (Miller's Review of Orthopaedics). A 2024 systematic review and meta-analysis (PMID: 38642740) confirms corticosteroid injection as superior to immobilisation alone.
A recent RCT (PMID: 39773153, 2025) found platelet-rich plasma (PRP) to be equivalent to corticosteroid injection, offering an alternative for patients in whom steroids are contraindicated (e.g., those with osteoporosis or prior adverse response).
Step 2: When Conservative Fails - Surgery
Surgery is indicated only when non-operative management fails, typically after 3-4 months of persistent symptoms despite adequate conservative treatment, including at least one corticosteroid injection.
The procedure is:
Surgical release of the first dorsal extensor compartment - the dorsal retinaculum is incised to decompress the APL and EPB tendons.
Important anatomical note:
Anatomic variations are common and must be addressed at surgery:
- Separate sub-compartments in 21-85% of cases
- Duplicated/multiple APL slips in >50% of patients
- EPB absent in ~5% of wrists
- Failure to identify and release separate EPB sub-compartment is the most common reason for surgical failure
Surgical outcomes:
- Generally excellent when performed correctly
- Complications are uncommon but include: iatrogenic injury to the superficial branch of the radial nerve (SBRN), tendon subluxation (if dorsal retinaculum not preserved), complex regional pain syndrome (CRPS), and recurrence from incomplete release
Summary: Is Operation Necessary?
| Scenario | Surgery Required? |
|---|---|
| Newly diagnosed, mild-moderate | No - try splinting + NSAIDs first |
| Persistent after 4-6 weeks conservative | No - corticosteroid injection |
| Failed 1-2 injections, 3-4 months of symptoms | Consider surgery |
| Recalcitrant / failed all conservative | Yes - surgical release indicated |
| Infection as cause | Never inject; may need surgical drainage |
Surgery is not the first step, but it is highly effective when properly indicated and has a low complication rate. The vast majority of patients are successfully managed non-operatively.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, p. 4494; Miller's Review of Orthopaedics 9th Ed, p. 672; Swanson's Family Medicine Review; PMID 38642740 (Systematic Review & Meta-Analysis, 2024); PMID 39773153 (RCT, 2025)
This is a shared conversation. Sign in to Orris to start your own chat.