Menstrual physiology after abortion
Reading File
Finding Sources
Finding Sources
Searching PubMed
menstrual recovery after abortion
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Searching the Web
menstrual physiology after abortion first period ovulation timing endometrial recovery
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC3443686
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full response:
Menstrual Physiology After Abortion
1. The Hormonal Trigger: Why the Cycle Restarts
During pregnancy, the trophoblast secretes human chorionic gonadotropin (hCG), which rescues and sustains the corpus luteum. The corpus luteum continues producing estrogen and progesterone, which suppress the hypothalamic-pituitary-ovarian (HPO) axis - specifically, they suppress GnRH pulsatility and inhibit FSH/LH secretion.
After abortion (whether surgical, medical, or spontaneous), the source of hCG is abruptly removed. Consequently:
- hCG levels fall rapidly (half-life ~24-36 hours for the beta subunit)
- Corpus luteum support withdraws
- Estrogen and progesterone levels plummet
- The HPO axis is disinhibited
This hormonal withdrawal from the endometrium triggers the cascade that leads to menstruation and cycle restart - essentially the same mechanism as corpus luteum demise at the end of a non-conception cycle. - Berek & Novak's Gynecology, Chapter 7
2. Hormonal Recovery: The FSH Rise and Folliculogenesis
With the fall of estrogen, progesterone, and inhibin A, pituitary FSH secretion rises. As described in Berek & Novak's:
"With the demise of the corpus luteum, FSH levels begin to rise, and a cohort of growing follicles is recruited. These follicles each secrete increasing levels of estrogen as they grow in the follicular phase."
This mirrors exactly what happens at the start of every normal cycle. After abortion, the same sequence unfolds:
- FSH rises as inhibitory signals (estrogen, progesterone, inhibin) disappear
- A new cohort of antral follicles is recruited
- A dominant follicle is selected
- Rising estradiol from the dominant follicle stimulates endometrial proliferation
- An LH surge triggers ovulation (24-36 hours later)
- Corpus luteum forms and secretes progesterone
- If no implantation occurs, luteolysis leads to menses
3. The Menstrual Cycle Diagram
The diagram below shows the normal interplay of hormones, ovarian histology, and endometrial changes across a 28-day cycle - the same pattern that resumes after abortion:
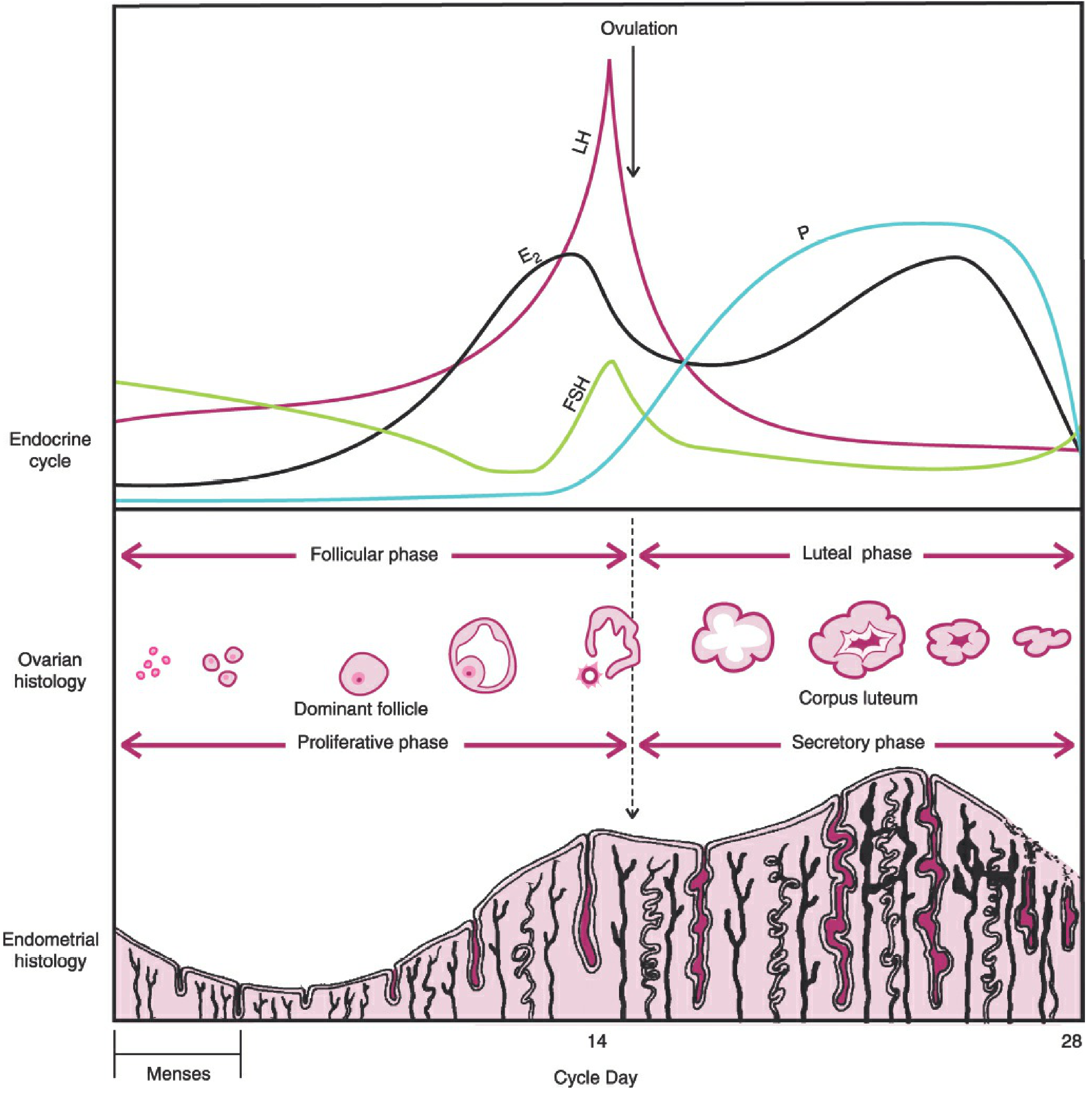
Fig 7-9, Berek & Novak's Gynecology - FSH, LH, estradiol (E2), and progesterone (P) variations correlated with follicular/luteal and proliferative/secretory phases
4. Timing of Ovulation After Abortion
This is clinically important - ovulation almost always precedes the first post-abortion period:
| Type | Mean Time to Ovulation | Range |
|---|---|---|
| Surgical abortion (first trimester) | ~20-29 days | 16-37 days |
| Medical abortion (mifepristone + misoprostol) | ~20.6 days | 8-36 days |
| Spontaneous abortion | ~20-29 days (median day 20) | 13-103 days |
| Second trimester abortion | Longer, ~>25 days | Variable |
Key findings from PMC research (PMID 21757051):
- 91% of women ovulate before their first menses after surgical abortion
- 83-100% ovulate before first menses after medical or spontaneous abortion
- By 3 weeks post-abortion: ~34% have already ovulated
- By 6 weeks post-abortion: ~78% have ovulated
- Surgical vs. medical abortion: no statistically significant difference in time to ovulation
Clinical implication: A woman can conceive before she even experiences her first post-abortion period. Contraception should be initiated immediately or within days if desired.
5. Endometrial Recovery
The endometrium undergoes rapid repair after abortion. Berek & Novak describes the cyclic histologic changes as two layers:
- Stratum functionale (superficial two-thirds): shed during menstruation and during/after abortion; regenerates each cycle under estrogen stimulation
- Stratum basale (deep one-third): retained; serves as the regenerative stem cell source
After abortion, residual decidualized or secretory endometrium is shed. Once estrogen rises from the new cohort of growing follicles, the basalis regenerates the functionale layer:
- Proliferative phase: Estrogen drives endometrial proliferation - straight glands become taller, stroma is compact, mitoses are visible
- Secretory phase (post-ovulation): Progesterone transforms endometrium - glands become tortuous and secretory, subnuclear vacuoles appear, stroma becomes edematous
- Menstrual phase: Luteolysis causes estrogen/progesterone withdrawal, prostaglandin-mediated vasospasm, and endometrial shedding
6. Timing of First Period After Abortion
| Situation | Expected First Period |
|---|---|
| First trimester abortion (surgical) | 4-6 weeks |
| First trimester abortion (medical) | 6-8 weeks |
| Women with normally irregular cycles | Up to 12 weeks |
| Second trimester abortion | Typically longer |
If no period by 8 weeks, evaluation is warranted to rule out retained products of conception, Asherman's syndrome (intrauterine adhesions from curettage), or ongoing pregnancy.
7. Character of First Post-Abortion Period
After surgical abortion (vacuum aspiration/D&C):
- Typically lighter than normal (endometrial cavity was evacuated, less tissue to shed)
- May be shorter in duration
- Risk of intrauterine adhesions (Asherman's syndrome) with aggressive curettage - can cause hypomenorrhea or amenorrhea
After medical abortion (mifepristone/misoprostol):
- Typically heavier than normal - residual decidua and products are shed with the first period
- May contain clots and tissue
- More pronounced cramps are common
Both types:
- The first 1-2 cycles may be irregular or differ from baseline
- Cycles typically normalize within 2-3 months
- Preceding contraceptive use, gestational age, and baseline cycle regularity all influence recovery timeline
8. Complications That Alter Menstrual Physiology
| Complication | Menstrual Effect |
|---|---|
| Retained products of conception | Prolonged bleeding, delayed cycle return |
| Intrauterine adhesions (Asherman's) | Hypomenorrhea, amenorrhea |
| Endometritis/infection | Irregular/heavy bleeding, cycle disruption |
| Luteal phase defect (rare) | Short cycles, spotting |
Summary
After abortion, the abrupt fall in hCG removes corpus luteum support, estrogen and progesterone drop, and the HPO axis is disinhibited. FSH rises within days, recruits a new follicular cohort, and ovulation typically occurs within 2-4 weeks (before the first period in the majority of women). The endometrium regenerates from the stratum basale under estrogen stimulation and undergoes a full proliferative-secretory-menstrual cycle. The first period typically returns within 4-8 weeks, and cycles normalize within 2-3 months. - Berek & Novak's Gynecology, Chapter 7; PMC3443686
This is a shared conversation. Sign in to Orris to start your own chat.