Hepatic encephalopathy management
Reading File
Finding Sources
Searching PubMed
"hepatic encephalopathy"[MeSH Terms] AND management
Searching the Web
hepatic encephalopathy management guidelines 2024 2025
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me synthesize a complete, well-structured answer.
Hepatic Encephalopathy (HE) - Management
Pathophysiology (Brief)
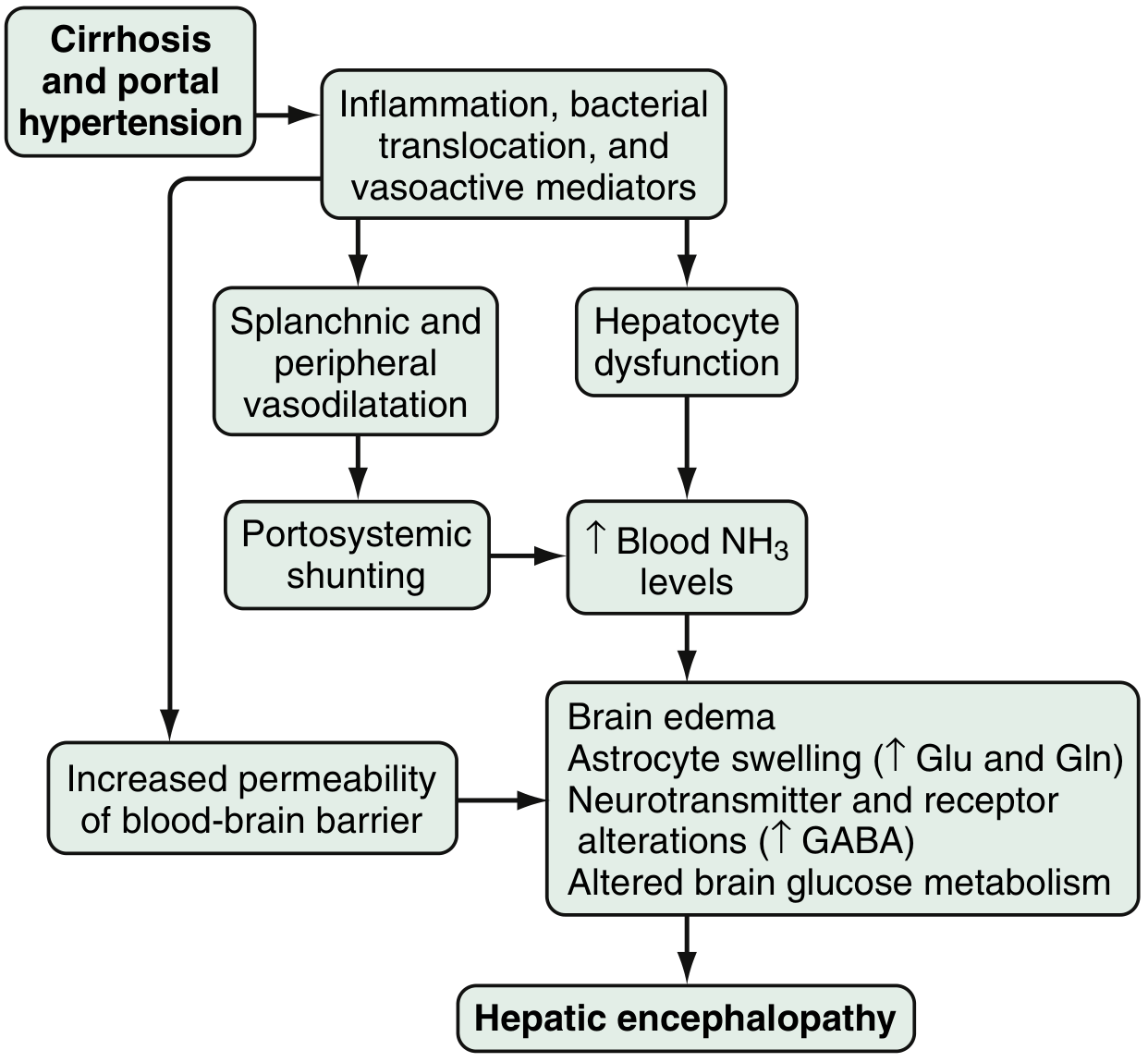
Fig. 94.1 - Proposed pathophysiology of HE (Sleisenger and Fordtran's)
HE results from the interplay of:
- Ammonia accumulation - produced in the colon by bacterial metabolism of protein/nitrogen compounds; normally cleared by hepatocytes but diverted via portosystemic shunting in cirrhosis
- Blood-brain barrier disruption - increases ammonia extraction by cerebellum and basal ganglia, causing astrocyte swelling, brain edema, and cytotoxic injury
- Neurotransmitter dysregulation - enhanced GABA/benzodiazepine receptor sensitivity (mediated by astrocyte neurosteroids), altered serotonin, NO, and opioid peptide signaling
- Inflammatory cascade - bacterial translocation and systemic inflammation amplify neurological dysfunction
Arterial hyperammonemia is present in ~90% of HE patients, yet serum ammonia levels are neither sensitive nor specific for diagnosis or staging. - Sleisenger and Fordtran's, p.1815
Classification - West Haven Criteria
| Grade | Consciousness | Clinical Features | Neurologic Signs | EEG |
|---|---|---|---|---|
| 0 | Normal | None | None | Normal |
| Minimal HE | Normal | Normal | Abnormal neuropsychological testing | Normal |
| 1 | Sleep-wake reversal, restlessness | Forgetfulness, irritability, mild confusion | Tremor, apraxia, incoordination | Abnormal |
| 2 | Lethargy, slow responses | Disorientation, amnesia, inappropriate behavior | Asterixis, dysarthria, ataxia, hypoactive reflexes | Abnormal |
| 3 | Somnolence, confusion | Disorientation, aggressive behavior | Asterixis, hyperactive reflexes, Babinski sign, muscle rigidity | Abnormal |
| 4 | Coma | Unresponsive | Decerebration | Abnormal |
Symptom to Diagnosis, Table 17-5
Types of HE
| Type | Cause | Prognosis | Key Treatment |
|---|---|---|---|
| Type A | Acute liver failure | Poor | Treat underlying cause, supportive, transplant |
| Type B | Non-cirrhotic portosystemic shunting (e.g., Budd-Chiari, congenital shunts) | Good | Shunt reduction/occlusion if amenable |
| Type C | Cirrhotic portal hypertension | Variable | Symptom control, prevent recurrence, transplant when indicated |
Precipitating Factors (ALWAYS identify and treat)
A mnemonic to remember these: "A BAD GI CHAP"
| Category | Examples |
|---|---|
| Infection | SBP, urinary, pulmonary - most common and must be sought actively |
| GI bleeding | Variceal or non-variceal; blood is a protein load in the gut |
| Electrolyte disturbances | Hypokalemia, alkalosis (from diuretics or vomiting) |
| Drugs | Benzodiazepines, barbiturates, opioids, narcotics |
| Dehydration/overdiuresis | Worsens azotemia and hepatic perfusion |
| Constipation | Increases intestinal ammonia absorption |
| Excess protein intake | High oral protein load |
| Progressive hepatic dysfunction | Natural disease progression |
| Portosystemic shunts | Surgical shunts or TIPS - may require reduction/occlusion |
| Azotemia/renal failure | Reduces ammonia clearance |
Goldman-Cecil Medicine; Washington Manual; Mulholland and Greenfield's Surgery
Management Framework
Step 1: Supportive Care
- Resuscitate and correct hemodynamic instability
- IV fluid resuscitation and rehydration
- Correct electrolyte abnormalities (especially hypokalemia, alkalosis)
- Ensure adequate caloric intake
- Airway protection in Grade 3-4 (intubation if needed)
- Avoid hepatotoxic and CNS-depressant drugs
Step 2: Reduce Gut Ammonia - Pharmacotherapy
First-Line: Lactulose
- Mechanism: Non-absorbable disaccharide; acts as cathartic to purge nitrogenous waste; acidifies colon (traps NH₃ as NH₄⁺, non-absorbable); reduces urease-producing bacteria
- Dose: 15-45 mL PO bid-qid (or 30 mL every 1-2 hours in acute phase, then taper once bowel movements begin)
- Target: 2-3 soft stools per day (titrate dose to achieve this)
- Enema: 300 mL lactulose + 700 mL distilled water for patients unable to take oral intake
- Cautions: Avoid in ileus or bowel obstruction; monitor for hypovolemia and hypernatremia
- Washington Manual, p.748; Goldman-Cecil Medicine; Symptom to Diagnosis
Second-Line / Add-on: Rifaximin
- Mechanism: Oral non-absorbable broad-spectrum antibiotic; reduces intestinal bacterial load and urease activity
- Dose: 550 mg PO bid (some sources cite 400 mg every 8 hours for acute phase)
- Evidence: RCT showed rifaximin + lactulose reduces recurrence of HE and time to first hospitalization over 6 months (49.1% reduction vs. lactulose alone + placebo)
- Role: Add rifaximin in patients not improving on lactulose alone; preferred over neomycin due to better safety profile
- Secondary prophylaxis: Rifaximin + lactulose for patients with recurrent encephalopathy
- Washington Manual; Mulholland and Greenfield's Surgery, p.2893
Alternative Antibiotics (less preferred)
- Neomycin: 500 mg to 1 g PO tid - limited by ototoxicity and nephrotoxicity
- Metronidazole: 250 mg PO bid-qid - limited by neurotoxicity with prolonged use
Step 3: Bowel Decontamination
- Bowel purge with oral cathartics or enemas to remove blood and nitrogenous compounds (especially after GI bleeding)
- Polyethylene glycol (PEG) 3350-electrolyte solution (4 L PO/NG over 4 hours) may produce more rapid clinical response than lactulose alone - Goldman-Cecil Medicine
Step 4: Nutrition
- Do NOT restrict dietary protein chronically - this worsens sarcopenia and malnutrition in cirrhosis, which independently worsens prognosis
- Target 1.2-1.5 g/kg/day protein intake
- Switch from animal protein to vegetable/dairy protein in recurrent/persistent HE (reduces ammoniagenic amino acids)
- Branched-chain amino acids (BCAAs): Supplement in patients intolerant of protein; corrects the BCAA:aromatic amino acid imbalance and improves recovery from episodic HE
- L-carnitine: Has been shown to improve cognitive deficits and reduce ammonia levels
- Late evening snack: Recommended by ACG 2025 guidelines to improve lean muscle tissue and reduce HE risk
- Mulholland and Greenfield's Surgery; Rosen's Emergency Medicine
Secondary Prophylaxis (Prevention of Recurrence)
After an episode of overt HE resolves:
- Lactulose - continue long-term; may discontinue if precipitating factor is well-controlled and liver/nutritional function has improved
- Rifaximin + lactulose - for patients with recurrent HE; significantly reduces further recurrence
- Identify and eliminate ongoing precipitants
- Counsel on dietary modification (vegetable-based protein, regular meals, avoid protein fasting)
- Review and eliminate offending medications (sedatives, opioids, proton pump inhibitors - a 2025 meta-analysis [PMID 40812534] shows PPIs significantly increase HE risk in cirrhotic patients and should be used cautiously)
Emerging and Adjunct Therapies
| Agent | Mechanism | Status |
|---|---|---|
| L-ornithine-L-aspartate (LOLA) | Increases ammonia fixation in liver (urea/glutamine synthesis) | Studied; some benefit |
| Sodium benzoate | Provides alternative ammonia excretion pathway | Being studied |
| Glycerol phenylbutyrate | Ammonia scavenger; reduces urease substrate | Being studied |
| Gut microbiome modulation | Reduce urease activity of colonic flora | Experimental (mouse data) |
| Extracorporeal liver support (MARS, SPAD) | Used in acute-on-chronic liver failure | 2025 meta-analysis (PMID 39578719) shows benefit; considered in ACLF |
TIPS-Related HE
- TIPS is a common precipitant of HE (worsens portosystemic shunting)
- If medically refractory, shunt reduction or occlusion may be required
- Must weigh against risk of recurrent variceal bleeding
Liver Transplantation
- Liver transplantation (LT) generally reverses HE and is the only definitive therapy
- Indicated in patients with refractory or recurrent HE with appropriate MELD score
- 1- and 3-year survival without LT: 42% and 23%, respectively
- Evaluate for transplant in all patients with overt HE episodes
- Sleisenger and Fordtran's, p.1815; Symptom to Diagnosis
Prognosis
- HE is a poor prognostic indicator: cumulative survival 20-40% at 1 year, 15% at 3 years without transplantation
- Associated with early readmissions and increased 1-year mortality
- Type A (ALF): highest mortality, urgent transplant consideration
Key Points / Clinical Pearls
- Blood ammonia level alone does not diagnose, stage, or predict prognosis of HE - diagnosis is clinical
- Always look for the underlying precipitating cause - treating it is as important as pharmacotherapy
- Avoid benzodiazepines and opioids; if sedation is needed, use low-dose alternatives carefully
- Asterixis (flapping tremor) is present in Grades 1-3 but is not specific to HE
- PPIs increase HE risk in cirrhotic patients and should be reviewed/discontinued if not necessary
- Protein restriction is harmful - maintain adequate protein with source modification
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease (p.1815-1816) | Goldman-Cecil Medicine | Washington Manual of Medical Therapeutics (p.747-748) | Mulholland and Greenfield's Surgery (p.2891-2893) | Symptom to Diagnosis, 4th Ed. | Rosen's Emergency Medicine | Recent meta-analyses: PMID 40812534 (PPIs and HE risk, 2025), PMID 39578719 (extracorporeal liver support in ACLF, 2025)
This is a shared conversation. Sign in to Orris to start your own chat.