Iv drip in newborn
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
IV drip newborn neonatal intravenous fluid therapy guidelines sites rates
Reading File
Here is a thorough, textbook-referenced overview of IV therapy in newborns:
IV Drip (Intravenous Fluid Therapy) in Newborns
1. Why Newborns Often Need IV Fluids
- Inability to feed orally (prematurity, respiratory distress, surgical conditions, hypoglycemia)
- Maintenance of hydration while enteral feeding is being established
- Medication delivery (antibiotics, inotropes, etc.)
- Correction of electrolyte imbalances or hypoglycemia
- Perioperative fluid replacement
2. Access Sites
Peripheral IV (PIV):
- Dorsum of hand, feet, antecubital fossa, or scalp veins (scalp veins common in neonates)
- Use 24-gauge cannulae in term newborns; 26-gauge in very premature infants
Umbilical Venous Catheter (UVC):
- Available in the first 7-10 days of life through the umbilical vein
- Preferred for central access in neonatal resuscitation and NICU admission
- Can be used to give glucose, medications, and TPN
Umbilical Arterial Catheter (UAC):
- Umbilical artery - used for continuous blood pressure monitoring and blood gas sampling
Intraosseous (IO):
- Emergency access if IV/UVC not obtainable (e.g., during resuscitation)
3. Fluid Requirements by Day of Life
Neonatal fluid requirements increase progressively during the first week of life. Established estimates for term newborns are:
| Day of Life | Fluid Requirement |
|---|---|
| Day 1 | 60 mL/kg/24 hr |
| Day 2 | 75 mL/kg/24 hr |
| Day 3 | 90 mL/kg/24 hr |
| Day 4 | 105 mL/kg/24 hr |
| Day 5 | 120 mL/kg/24 hr |
| Day 6 | 135 mL/kg/24 hr |
| Day 7 | 150 mL/kg/24 hr |
| After day 7 | 150 mL/kg/24 hr (maintenance) |
Preterm and VLBW infants have higher insensible water losses (thin, highly permeable skin; larger surface area:weight ratio) and may need up to 200 mL/kg/day. Humidified incubators reduce insensible losses by up to 30%.
- Barash Clinical Anesthesia 9e, p. 3584-3585
- Miller's Anesthesia 10e, p. 10617
4. Fluid Type
Maintenance Fluid
- Standard: 10% Dextrose + 0.2% NaCl + 20 mmol/L KCl for the first 48 hours
- Reason for sodium: The neonatal distal tubule cannot fully respond to aldosterone, causing obligate sodium losses - IV fluids must contain sodium to avoid hyponatremia
- After 48-72 hours: term infants may tolerate 5% Dextrose instead of 10%; preterm infants often need the higher glucose load longer
- Hypotonic solutions alone are contraindicated for replacing blood/ECF losses - they cause hyponatremia and hypovolemia
Replacement Fluid (blood loss, ECF losses, surgery)
- Use near-isotonic solutions: Lactated Ringer's (LR) or PlasmaLyte
- These match the electrolyte composition of ECF
Colloids
-
Albumin 5% is traditionally used as the plasma expander of choice in neonates
-
Synthetic colloids (HES, gelatin) have been used but safety data in neonates remain limited
-
Barash Clinical Anesthesia 9e, p. 3585
5. Glucose Management
- Neonates are prone to hypoglycemia (especially: premature infants, infants of diabetic mothers, SGA, those receiving continuous glucose infusions that are abruptly stopped)
- Glucose infusion rate (GIR) is typically maintained at 4-6 mg/kg/min in stable term neonates; preterm infants may need 6-8 mg/kg/min
- D10W at 60 mL/kg/day ≈ 4.2 mg/kg/min GIR; at 80 mL/kg/day ≈ 5.6 mg/kg/min
- Monitor blood glucose regularly, especially perioperatively
- Iatrogenic hyperglycemia from excess dextrose can augment ischemic brain injury - balance is key; however, in cardiac surgery neonates, avoiding hypoglycemia takes precedence
6. Electrolytes
- Serum potassium may be 1-2 mmol/L higher than adult normal in the first 2 days (physiological)
- Sodium supplementation is added from Day 2-3 onward; avoid in first 24 hours due to post-birth natriuresis
- Calcium supplementation is needed in preterm infants and those at risk of hypocalcemia
- Monitor: Na, K, glucose, urine output (target ≥ 1-2 mL/kg/hr after Day 1)
7. Physiological Considerations Specific to Newborns
| Feature | Clinical Impact |
|---|---|
| Low GFR (matures over weeks) | Cannot excrete excess water or sodium efficiently |
| Large ECF (40% body weight) | Post-birth diuresis expected - 5-10% weight loss is normal |
| High TBW (80% body weight in term; 90% in VLBW) | ECF contracts after birth - do not over-restrict fluids |
| Immature tubular function | Obligate sodium loss in first days; avoid sodium-free fluids |
| High insensible losses (preterm) | Higher fluid needs; use humidified environments |
- Blood volume: ~90 mL/kg in term newborns, ~100 mL/kg in preterm/VLBW
- Barash Clinical Anesthesia 9e, p. 3583-3585
8. Monitoring
| Parameter | Target |
|---|---|
| Urine output | 1-2 mL/kg/hr (after Day 1) |
| Body weight | Max 5-10% weight loss in first week is normal |
| Serum electrolytes | Check daily in NICU |
| Blood glucose | Maintain > 2.6-2.8 mmol/L (47-50 mg/dL) |
| Hematocrit | Transfuse if Hct <30% in first week; <25% after 2 weeks (restrictive threshold: Hgb ~9 g/dL first week, ~7 g/dL after 2 weeks) |
9. Special Scenarios
- Neonatal surgery: Replace ongoing losses with isotonic fluids (LR/PlasmaLyte); abdominal surgery losses can exceed 50 mL/kg/hr
- Resuscitation: UVC is the fastest reliable central access; intraosseous is the emergency backup
- TPN: For neonates who cannot receive enteral feeds; provides amino acids, lipids, glucose, electrolytes, vitamins
Key principles summarized:
- Start low (60 mL/kg/day Day 1), increase daily to 150 mL/kg/day by Day 7
- Use glucose-containing solutions with sodium (not plain dextrose, not hypotonic saline alone)
- Monitor glucose closely, especially in at-risk groups
- Prefer isotonic solutions (LR, PlasmaLyte) for any volume replacement
- Preterm infants need more fluid and more careful monitoring than term newborns
Sources: Barash Clinical Anesthesia 9e; Miller's Anesthesia 10e
Iso p 80 ml can be given in four hours in three day, old newborn
Finding Sources
Finding Sources
Reading File
Finding Sources
Direct Answer: Is 80 mL Isotonic Fluid Over 4 Hours Safe in a 3-Day-Old?
It depends entirely on the baby's weight and the clinical indication. Here is the breakdown:
Step 1 - Calculate the Projected Daily Rate
80 mL over 4 hours = 20 mL/hr
Over 24 hours = 20 × 24 = 480 mL/day
Step 2 - Compare to Allowed Daily Maintenance
Day 3 of life maintenance allowance = 90 mL/kg/24 hr
(Barash Clinical Anesthesia 9e)
| Baby's weight | Allowed per day (90 mL/kg) | 80 mL/4 hr is... |
|---|---|---|
| 1 kg | 90 mL | 5.3× the daily limit - dangerous overdose |
| 2 kg | 180 mL | 2.7× the daily limit - dangerous |
| 3 kg | 270 mL | 1.8× the daily limit - unsafe as maintenance |
| 3.5 kg | 315 mL | 1.5× the daily limit - unsafe |
Conclusion: 80 mL over 4 hours as a continuous maintenance drip is NOT appropriate for a 3-day-old at any typical birth weight. The neonatal kidney at this age cannot excrete excess water, making fluid overload a real and dangerous risk.
What 80 mL in 4 Hours Could Be Acceptable As
Only if it is a resuscitation/volume expansion bolus (not maintenance):
- Neonatal shock/resuscitation bolus is typically 10-20 mL/kg of isotonic fluid given over 30-60 minutes
- For a 3 kg baby: 10 mL/kg = 30 mL, 20 mL/kg = 60 mL - given once, rapidly, not over 4 hours
- Even as a bolus, 80 mL (= ~27 mL/kg for a 3 kg baby) at that rate would need to be justified by a clear clinical picture of severe hypovolemia/shock
What the Correct Maintenance Rate Looks Like for a 3-Day-Old
For a 3 kg baby on Day 3:
- Total daily fluid = 90 mL/kg × 3 kg = 270 mL/day
- Hourly rate = 270 ÷ 24 = ~11.25 mL/hr
- Over 4 hours = 11.25 × 4 = ~45 mL (not 80 mL)
Why Fluid Overload is Especially Dangerous in Neonates
- Immature kidneys - GFR is low at Day 3; excess water cannot be excreted efficiently
- Large ECF volume - The newborn is already in the process of normal post-birth diuresis; adding excess fluid disrupts this
- Pulmonary consequences - Overload causes pulmonary edema, worsens respiratory distress
- Risk of patent ductus arteriosus (PDA) - Fluid overload is a well-known trigger for symptomatic PDA in preterm neonates
- Hyponatremia - Excess isotonic volume can dilute sodium in the face of impaired excretion
- IVH risk in preterm infants - Rapid volume shifts increase risk of intraventricular hemorrhage
Bottom Line
| Scenario | Is 80 mL/4 hr appropriate? |
|---|---|
| As maintenance drip | No - far exceeds Day 3 limits at any weight |
| As a single resuscitation bolus for shock in a 3-4 kg baby | Possibly, but 10-20 mL/kg over 30-60 min is the standard |
| For a preterm <1.5 kg baby | Absolutely not |
If you are managing a specific clinical case, the appropriate rate should be calculated as: (90 mL × weight in kg) ÷ 24 hours, with the fluid type being D10W + 0.2% NaCl (± KCl from Day 2-3 onward).
Acute kidney failure in newborn baby.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching the Web
neonatal acute kidney injury AKI causes diagnosis management guidelines 2023 2024
Searching PubMed
"neonatal acute kidney injury" AND management
Reading Web Page
https://cps.ca/en/documents/position/acute-kidney-injury
Loading Image
Acute Kidney Injury (AKI) in the Newborn
1. Overview
Neonatal AKI is a common and serious condition - occurring in up to 38% of NICU admissions, and in up to 40% of neonates with associated comorbidities (e.g., perinatal asphyxia, sepsis, CHD). It is associated with increased mortality, prolonged hospital stay, and long-term risk of chronic kidney disease (CKD).
The newborn kidney is inherently vulnerable because:
- GFR is very low at birth and matures slowly over weeks
- Tubular function is immature (poor ability to concentrate/dilute urine, obligate sodium losses)
- The kidney cannot efficiently handle excess fluid, electrolytes, or nephrotoxins
2. Definition (Modified KDIGO for Neonates)
AKI is defined by rise in serum creatinine (SCr) OR fall in urine output:
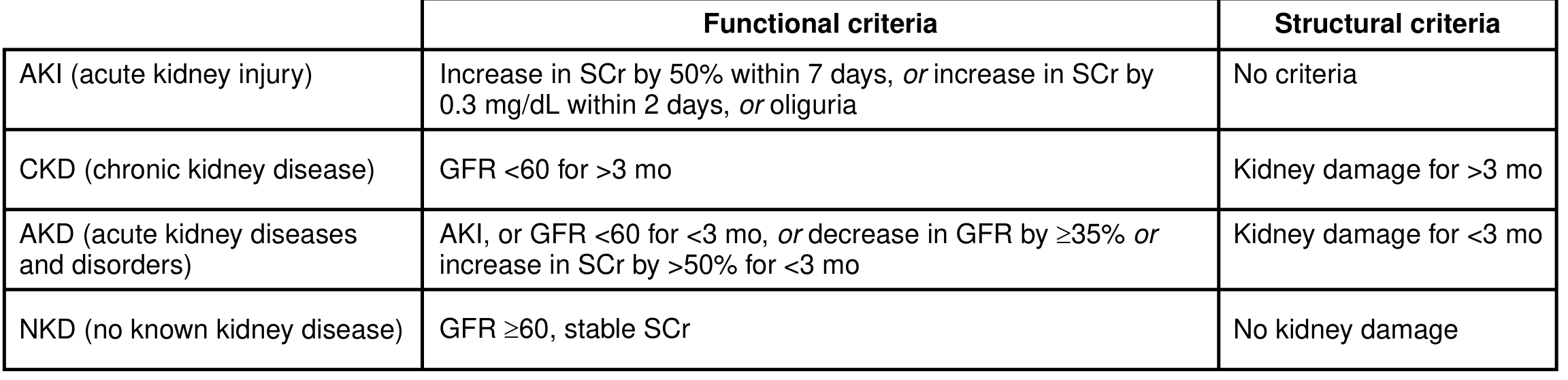
Important neonatal caveat: At birth, neonatal SCr reflects maternal creatinine (normally ~0.8-1.0 mg/dL). It physiologically falls over the first 7-14 days to a nadir of ~0.3-0.4 mg/dL in term infants (lower in preterm). Therefore, a rising SCr in the first days of life - even if the absolute value is "normal" - is abnormal and suggests AKI.
KDIGO Staging for Neonates
| Stage | Serum Creatinine Criteria | Urine Output Criteria |
|---|---|---|
| 1 | Rise ≥0.3 mg/dL in 48 hrs OR ≥1.5x baseline in 7 days | <1.0 mL/kg/hr for 6-12 hrs |
| 2 | ≥2.0x baseline | <0.5 mL/kg/hr for ≥12 hrs |
| 3 | ≥3.0x baseline OR SCr ≥2.5 mg/dL | <0.3 mL/kg/hr for ≥24 hrs OR anuria ≥12 hrs |
3. Causes - The Three Categories
A. Prerenal (Most Common, ~70%)
Reduced kidney perfusion - kidney structure is intact
- Hypovolemia (fluid losses, hemorrhage, dehydration)
- Perinatal asphyxia / hypoxia-ischemia (HI)
- Sepsis / septic shock
- Cardiac failure / congenital heart disease (CHD)
- Patent ductus arteriosus (PDA) - reduces renal perfusion
- Necrotizing enterocolitis (NEC)
- High mean airway pressure (impairs venous return)
- Twin-to-twin transfusion syndrome (donor twin)
- ECMO
B. Intrinsic Renal (Intrinsic damage to kidney parenchyma)
- Acute tubular necrosis (ATN) - most common intrinsic cause; follows prolonged prerenal or nephrotoxin exposure
- Nephrotoxic medications: aminoglycosides (gentamicin), vancomycin, NSAIDs (indomethacin, ibuprofen - close PDA but impair renal blood flow), amphotericin B, acyclovir, contrast agents
- Renal vein thrombosis (presents with hematuria, thrombocytopenia, flank mass)
- Congenital renal anomalies (polycystic kidney disease, renal dysplasia)
- Perinatal asphyxia - direct tubular ischemic injury
C. Postrenal (Obstructive)
- Posterior urethral valves (PUV) - most common obstructive cause, males only
- Ureteropelvic junction (UPJ) obstruction
- Bilateral hydronephrosis
- Urethral atresia, prune belly syndrome
4. Risk Factors for Neonatal AKI
| Category | Examples |
|---|---|
| Prematurity / low birth weight | VLBW (<1500 g), ELBW (<1000 g) |
| Perinatal events | Asphyxia, Apgar <6 at 5 min |
| Infections | Sepsis, congenital infections |
| Structural | Congenital heart disease, renal anomalies |
| Drugs | Aminoglycosides, NSAIDs, vancomycin, ACE inhibitors (maternal) |
| Procedures | Cardiac surgery, ECMO |
| Metabolic | Hyperuricemia (tumor lysis), hemolysis |
5. Clinical Features
- Oliguria - urine output <1 mL/kg/hr (most sensitive early sign); anuria may be present
- Edema - periorbital, peripheral, or generalized; fluid overload
- Hypertension - due to fluid/sodium retention
- Electrolyte abnormalities:
- Hyperkalemia (dangerous - can cause arrhythmias)
- Hyponatremia (dilutional)
- Hyperphosphatemia
- Hypocalcemia
- Metabolic acidosis
- Elevated SCr and BUN (azotemia)
- Signs of underlying cause - pallor (sepsis), respiratory distress, abdominal distension (NEC/obstruction)
6. Investigations
| Test | Purpose |
|---|---|
| Serum creatinine (daily) | Define and stage AKI |
| BMP (Na, K, Cl, HCO3, BUN, Cr) | Electrolytes + acid-base |
| Calcium, phosphate | Metabolic effects |
| Urine output (strict I/O, daily weights) | Monitor function |
| Urine analysis (dipstick + microscopy) | Hematuria → thrombosis/glomerular; casts → ATN |
| Urine Na, FENa | Distinguish prerenal vs intrinsic |
| Renal ultrasound | Structural anomalies, obstruction, vascular Doppler |
| Blood gas | Metabolic acidosis severity |
| CBC, cultures | Sepsis workup |
FENa (Fractional Excretion of Sodium) in Neonates
- FENa = (urine Na × plasma Cr) ÷ (plasma Na × urine Cr) × 100
- Prerenal: FENa <2-3% in term; <5% in preterm
- Intrinsic ATN: FENa >3% in term; >5% in preterm
- (Note: FENa is normally higher in preterm neonates due to immature tubular reabsorption - interpret carefully)
7. Management
Step 1 - Treat the Underlying Cause
- Restore perfusion (fluid resuscitation for prerenal) - isotonic bolus 10-20 mL/kg over 30-60 min
- Treat sepsis (antibiotics - choose least nephrotoxic regimen)
- Relieve obstruction (urinary catheter, urology consult for PUV)
- Stop nephrotoxic drugs
Step 2 - Fluid Management
- If hypovolemic (prerenal): fluid challenge 10-20 mL/kg isotonic saline or LR
- If euvolemic/hypervolemic (intrinsic/established AKI): fluid restrict to insensible losses (~30-50 mL/kg/day) + urine output replacement only
- Strict input/output records and daily weights are mandatory
- Avoid fluid overload - it is independently associated with mortality
Step 3 - Electrolyte Management
| Problem | Treatment |
|---|---|
| Hyperkalemia (K+ >6.5 mEq/L or ECG changes) | Stop K+ intake; calcium gluconate (cardiac stabilization); sodium bicarbonate; glucose + insulin; kayexalate (sodium polystyrene) - use cautiously in neonates due to NEC risk; dialysis if refractory |
| Hyponatremia | Fluid restrict (dilutional); replace only if symptomatic |
| Metabolic acidosis | Sodium bicarbonate if pH <7.2 or HCO3 <12 |
| Hypocalcemia | IV calcium gluconate |
| Hyperphosphatemia | Phosphate binders (calcium carbonate with feeds) |
Step 4 - Nutritional Support
- Ensure adequate caloric intake despite fluid restriction
- Adjust formula concentration or TPN
- Dietitian consultation for fluid-restricted neonates
Step 5 - Drug Dose Adjustment
- All renally-cleared drugs must have doses/intervals adjusted
- Aminoglycosides: extend dosing interval, monitor drug levels
- Avoid NSAIDs, contrast agents, nephrotoxic combinations
Step 6 - Dialysis / Renal Replacement Therapy (RRT)
Indications:
- Severe refractory hyperkalemia
- Fluid overload unresponsive to diuretics
- Severe metabolic acidosis
- Uremic symptoms (encephalopathy, pericarditis)
- SCr ≥2.5 mg/dL persistent
Modalities in neonates:
- Peritoneal dialysis (PD) - first choice in most neonatal centers; catheter inserted surgically; well-tolerated even in small/preterm infants
- Continuous renal replacement therapy (CRRT) - for hemodynamically unstable neonates; requires specialized equipment and vascular access; used in larger/more stable NICUs
- Hemodialysis is rarely used in neonates due to technical difficulty
8. Diuretics in Neonatal AKI
- Furosemide: often used to convert oliguric to non-oliguric AKI and to manage fluid overload
- Does NOT improve outcomes or reduce need for dialysis - used for fluid management, not to treat AKI itself
- Dose: 1-2 mg/kg IV; can be given as continuous infusion in severe fluid overload
- Use only after adequate volume status is confirmed (not in prerenal AKI)
9. When to Consult Nephrology
- AKI stage 2-3 (KDIGO)
- SCr ≥2.5 mg/dL persisting beyond 3 days
- Need for dialysis
- Suspected structural renal anomaly
- Refractory electrolyte disturbances
10. Prognosis and Follow-up
- Most prerenal AKI resolves with treatment of the underlying cause
- ATN may take days to weeks to recover
- Long-term risk: neonatal AKI - even if resolved - is associated with:
- CKD in childhood and adulthood
- Hypertension
- Reduced nephron mass (especially in preterm)
- Recommended follow-up:
- 3-6 months post-discharge for AKI requiring dialysis
- 6-12 months for preterm/SGA infants with severe AKI (SCr ≥2.5 mg/dL)
- Annual BP and creatinine checks thereafter
Sources: National Kidney Foundation Primer on Kidney Diseases 8e; Barash Clinical Anesthesia 9e; Canadian Paediatric Society AKI Guidelines (2024); Newborn Critical Care Center AKI Clinical Guidelines (reviewed March 2024); KDIGO AKI Framework
This is a shared conversation. Sign in to Orris to start your own chat.