Define oedema and pathogenesis refer Robbins and harshmohan pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed from Robbins (both Basic Pathology and Pathologic Basis of Disease). Note that Harsh Mohan's pathology textbook is not available in the library, so I'll clearly note this. Let me now compile the comprehensive answer.
Oedema (Edema) - Definition and Pathogenesis
Source: Robbins & Kumar Basic Pathology (9th ed.) and Robbins, Cotran & Kumar Pathologic Basis of Disease
Note: Harsh Mohan's Textbook of Pathology is not available in the medical library, so the content below is drawn entirely from Robbins (both editions), which covers this topic in full detail.
Definition
Oedema is defined as an abnormal accumulation of interstitial fluid within tissues.
- Approximately 60% of lean body weight is water, of which two-thirds is intracellular. Most remaining water is interstitial fluid; only 5% of total body water is in blood plasma.
- When extravascular fluid collects in body cavities rather than tissue, it is called an effusion:
- Pleural cavity = Hydrothorax
- Pericardial cavity = Hydropericardium
- Peritoneal cavity = Hydroperitoneum (Ascites)
- Anasarca = severe, generalized edema with profound swelling of subcutaneous tissues and accumulation in multiple body cavities.
Oedema fluid falls into two types:
| Type | Protein content | Cause |
|---|---|---|
| Transudate | Protein-poor | Hydrostatic/osmotic imbalance (non-inflammatory) |
| Exudate | Protein-rich | Increased vascular permeability (inflammatory) |
Pathogenesis
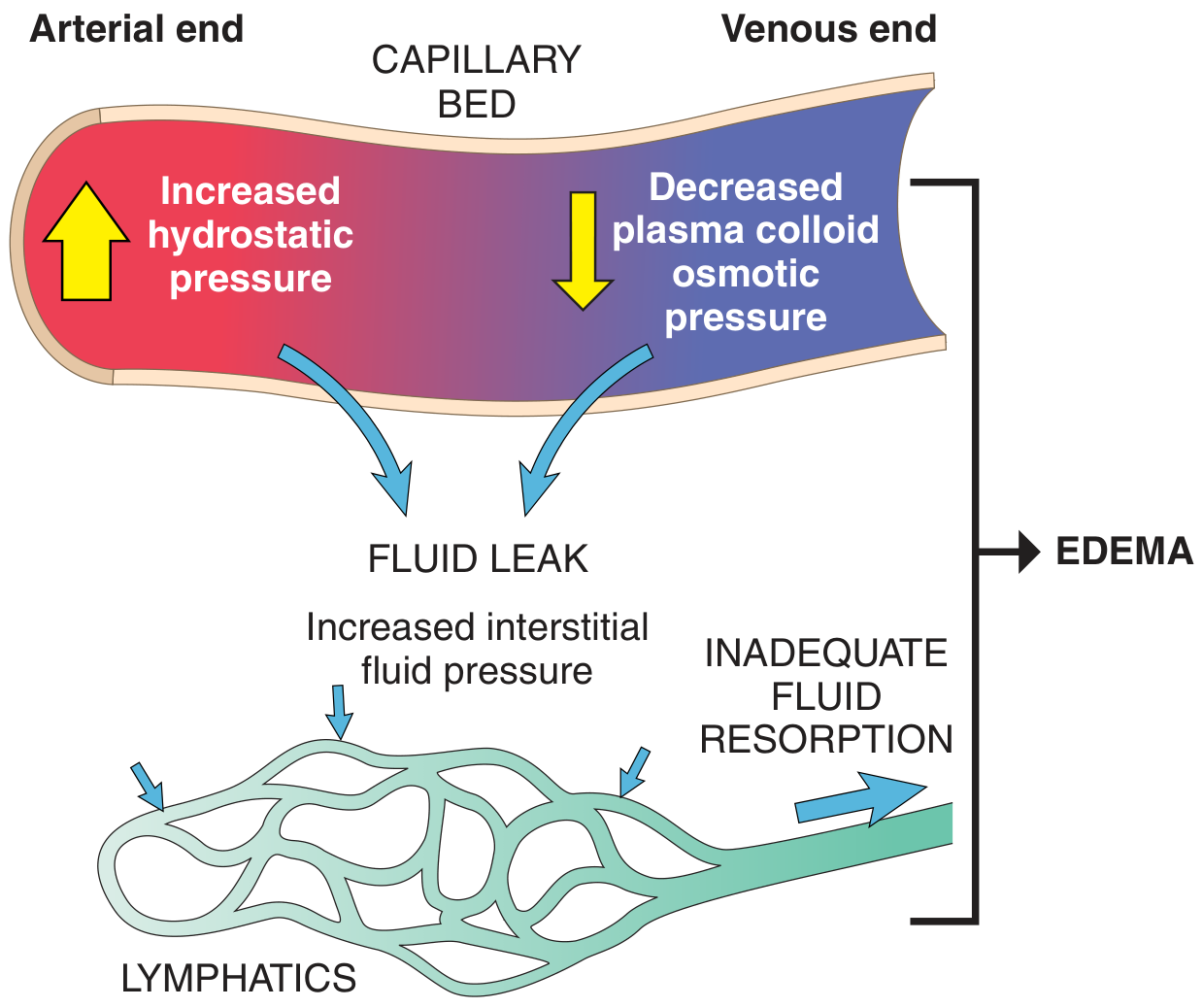
Normal Starling Forces (the Baseline)
Fluid movement between the vascular and interstitial spaces is governed by two opposing forces:
- Vascular hydrostatic pressure - pushes fluid OUT of capillaries into interstitium
- Colloid osmotic pressure (from plasma proteins, mainly albumin) - pulls fluid BACK into capillaries
Normally, outflow at the arteriolar end is nearly balanced by inflow at the venular end. The small net outflow is drained by lymphatic vessels back to the bloodstream via the thoracic duct - keeping tissues "dry."
Edema results when:
- Hydrostatic pressure increases, OR
- Colloid osmotic pressure decreases, OR
- Lymphatic drainage is overwhelmed or obstructed
Mechanisms of Edema Formation
1. Increased Hydrostatic Pressure
Mainly caused by disorders that impair venous return:
- Localized: Deep vein thrombosis (DVT) in lower extremity -> edema confined to distal leg
- Generalized: Congestive heart failure -> systemic venous pressure rise -> widespread edema
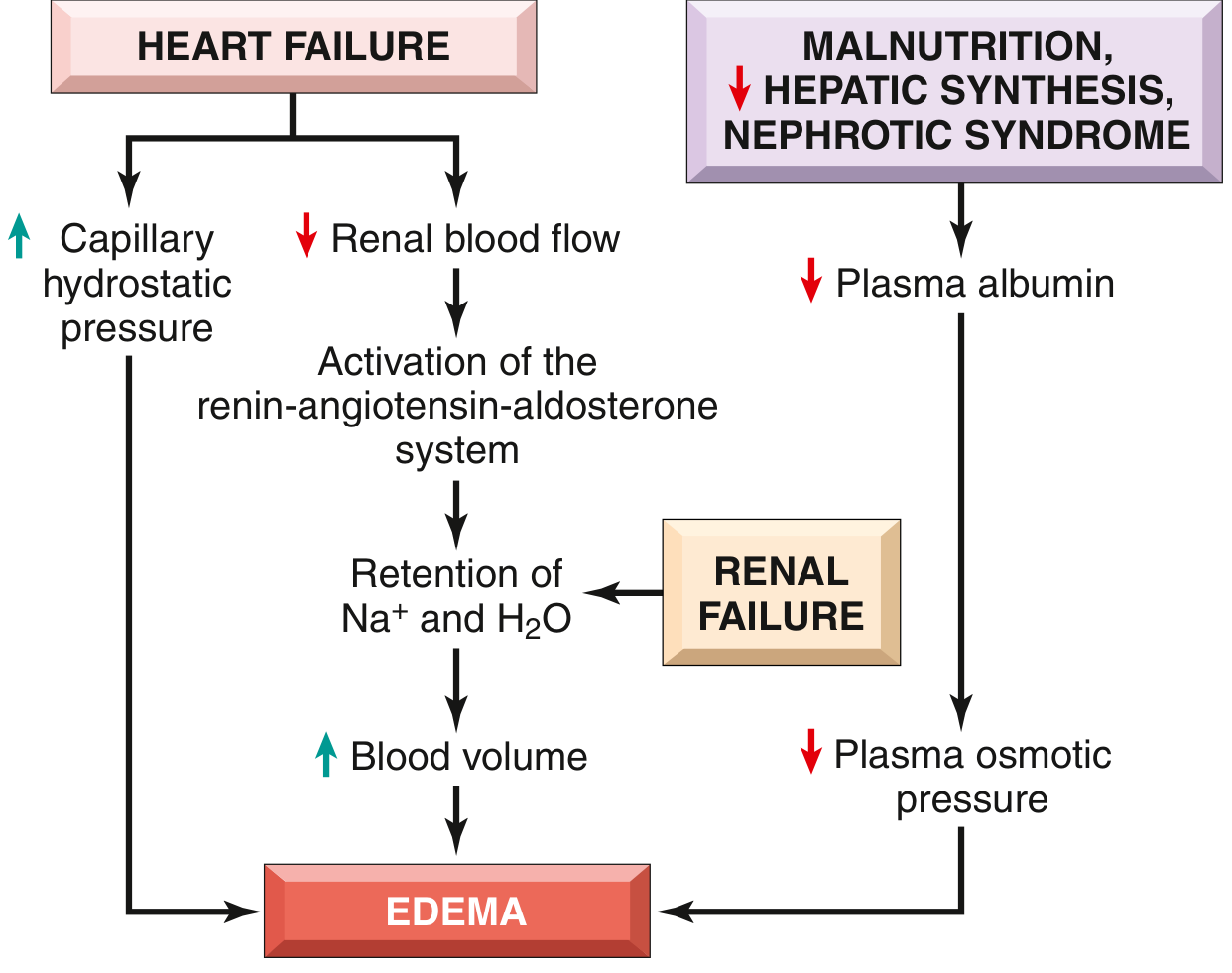
Mechanism in heart failure:
- Reduced cardiac output -> pooling of blood in venous circulation -> increased capillary hydrostatic pressure
- Simultaneously, reduced cardiac output -> renal hypoperfusion -> activation of renin-angiotensin-aldosterone (RAA) axis -> Na+ and water retention (secondary hyperaldosteronism)
- In a normal heart, this would boost cardiac filling and output. In the failing heart, the increased cardiac filling cannot be translated into increased output -> fluid retention worsens -> vicious cycle of increasing hydrostatic pressure and worsening edema.
Other causes: constrictive pericarditis, liver cirrhosis, venous obstruction/compression, arteriolar dilation (heat, neurohumoral dysregulation), lower extremity inactivity.
2. Reduced Plasma Osmotic Pressure (Hypoproteinemia)
Albumin accounts for ~50% of total plasma protein and is the primary contributor to colloid osmotic pressure.
Albumin levels fall due to:
- Increased urinary loss: Nephrotic syndrome - damaged glomeruli allow albumin to pass into urine
- Decreased synthesis: Severe liver disease (cirrhosis), protein malnutrition, protein-losing gastroenteropathy
Consequence: Low albumin -> increased fluid out of vessels -> reduced intravascular volume -> renal hypoperfusion -> secondary hyperaldosteronism -> Na+ and water retention. Critically, this retention does NOT fix the problem (the primary defect - low plasma protein - persists), and actually exacerbates the edema.
3. Lymphatic Obstruction (Lymphedema)
When lymphatic vessels are obstructed, interstitial fluid that normally drains back into circulation accumulates.
Causes:
- Inflammatory: Recurrent infections
- Neoplastic: Tumor compression/infiltration
- Parasitic: Filariasis (Wuchereria bancrofti) - massive lymphedema of the lower extremities and scrotum = elephantiasis
- Post-surgical / post-irradiation: e.g., arm edema after axillary lymph node dissection in breast cancer
4. Sodium Retention
Excess Na+ retention causes isotonic water retention, expanding interstitial fluid volume.
Causes:
- Excessive salt intake with renal insufficiency
- Decreased renal excretion of Na+ (renal hypoperfusion, increased RAA activity)
- Primary renal disease (e.g., acute renal failure, post-streptococcal glomerulonephritis)
5. Increased Vascular Permeability (Inflammatory Edema)
In acute or chronic inflammation and angiogenesis, inflammatory mediators (histamine, bradykinin, leukotrienes, etc.) increase vascular permeability -> protein-rich exudate leaks into tissues -> edema. This is discussed separately under inflammation.
Summary Diagram of Systemic Edema Pathways
Causes of Edema (Table 3.1 / Table 4.1, Robbins)
| Category | Specific Causes |
|---|---|
| Increased Hydrostatic Pressure | CCF, constrictive pericarditis, liver cirrhosis, DVT, venous compression by mass, prolonged dependency, arteriolar dilation |
| Reduced Plasma Osmotic Pressure | Nephrotic syndrome, severe liver disease, malnutrition, protein-losing gastroenteropathy |
| Lymphatic Obstruction | Inflammatory, neoplastic, post-surgical, post-irradiation (filariasis) |
| Sodium Retention | Renal insufficiency with excess salt, decreased Na+ excretion, renal hypoperfusion, increased RAA secretion |
| Inflammation | Acute, chronic inflammation, angiogenesis |
Morphology
- Gross: Edematous tissues feel wet; sectioned lung exudes frothy, blood-tinged fluid
- Microscopy: Clearing and separation of extracellular matrix elements
- Subcutaneous edema: Dependent distribution (legs when standing, sacrum when supine) = dependent edema; finger pressure leaves a depression = pitting edema
- Renal/nephrotic edema first appears in loose connective tissue - periorbital edema
- Pulmonary edema: Lungs 2-3x normal weight with frothy fluid
- Cerebral edema: Narrowed sulci, swollen and flattened gyri
Clinical Significance
| Site | Significance |
|---|---|
| Subcutaneous | Signals cardiac or renal disease; impairs wound healing and infection clearance |
| Pulmonary | Interferes with ventilation; predisposes to superimposed infection; can be fatal |
| Cerebral | Life-threatening; may cause herniation through foramen magnum; compromises brain stem - respiratory arrest |
Robbins & Kumar Basic Pathology, Chapter 3 (Hemodynamic Disorders), pp. 78-81
Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 4, pp. 117-118
This is a shared conversation. Sign in to Orris to start your own chat.