Abdominal x-ray 101
abdominal x-ray normal bowel gas pattern interpretation
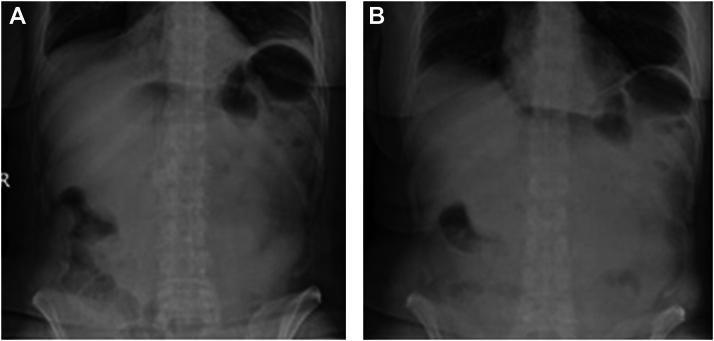
small bowel obstruction abdominal x-ray dilated loops air fluid levels
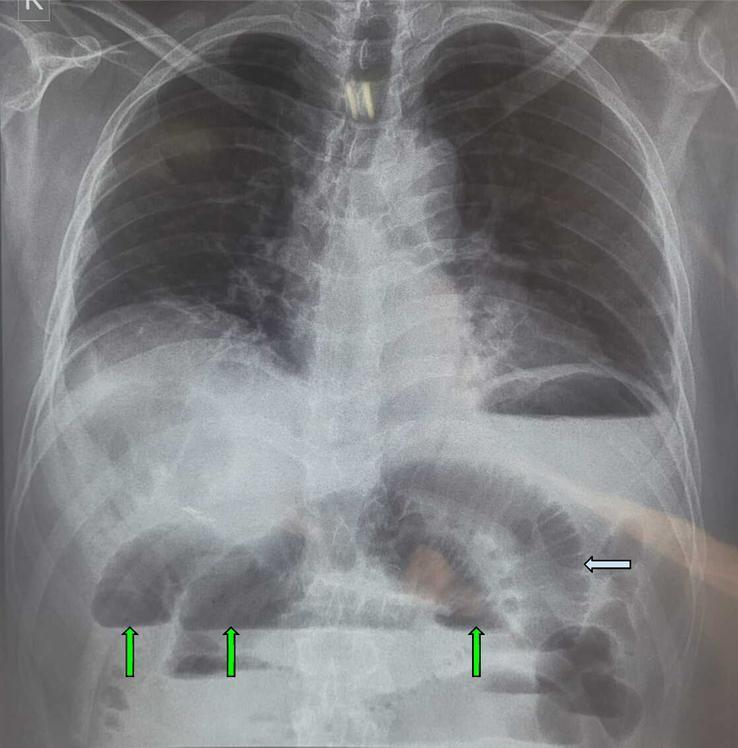
pneumoperitoneum free air under diaphragm erect chest x-ray perforated viscus
Abdominal X-Ray (AXR) 101
1. Overview & When to Order It
| Indication | Notes |
|---|---|
| Suspected viscus perforation | Pair with erect CXR |
| Bowel obstruction | Small or large bowel |
| Bowel wall pattern assessment | Ischaemia, colitis |
| Intra-abdominal foreign body | Ingested items, surgical hardware |
| Urinary tract calculi follow-up | Monitoring radiopaque stones |
| Bowel transit time in constipation | Marker studies |
2. Standard Views
- Supine AXR: The workhorse. Should cover diaphragm to hernial orifices (obturator foramina must be included).
- Erect CXR: The most sensitive plain-film test for pneumoperitoneum — patient should ideally stand for 10 minutes beforehand to allow free gas to rise.
- Left lateral decubitus AXR: Used when the patient cannot stand; free air collects between the liver and right lateral abdominal wall.
- Erect AXR: Historically used for air-fluid levels, but now discouraged — evidence shows it can be misleading.
3. Systematic Approach — The ABCDE Framework
| Letter | What to Check |
|---|---|
| A — Air | Distribution of bowel gas; free air; pneumobilia |
| B — Bowel | Calibre (dilated?); pattern (SB vs. LB); mucosal folds |
| C — Calcification | Stones, vascular calcification, pancreatic calcification |
| D — Densities/Organs | Liver, spleen, kidneys, psoas shadows, bladder |
| E — Extras | Bones, soft tissues, foreign bodies, tubes/lines |
4. Normal Bowel Gas Pattern
- Small bowel: Located centrally, calibre ≤3 cm in adults, shows valvulae conniventes (thin, complete folds that span the full bowel width — most prominent in the jejunum)
- Large bowel: Located peripherally, calibre up to 5–6 cm (caecum up to 9 cm), shows haustra (thick, incomplete folds that only partially cross the lumen)
- Rectum: Usually contains some gas/stool
- Gas should be present in stomach, small bowel, colon, and rectum; a gasless abdomen may indicate fluid-filled obstruction or ascites
Key rule (Harriet Lane): Small bowel is central with valvulae; large bowel is peripheral with haustra.
5. Abnormal Gas Distribution
A. Pneumoperitoneum (Free Intraperitoneal Air)

| Sign | Description |
|---|---|
| Subdiaphragmatic crescent (erect CXR) | Radiolucent gas between diaphragm and liver — most sensitive plain film sign |
| Rigler's sign (double wall sign) | Gas visible on both sides of the bowel wall on a supine AXR |
| Falciform ligament sign | Free gas outlines the normally invisible falciform ligament |
| Football sign | Massive pneumoperitoneum gives an oval gas-filled appearance of the abdomen |
| Continuous diaphragm sign | Air outlines the inferior diaphragm, including under the heart silhouette |
⚠️ Causes of pneumoperitoneum without peritonitis: recent laparotomy/laparoscopy, pneumatosis intestinalis, vaginal douche — do not always indicate perforation.
B. Gas in Bowel Wall (Pneumatosis Intestinalis)
6. Bowel Obstruction
Small Bowel Obstruction (SBO)
- Multiple centrally-placed dilated loops (diameter >3.5 cm, usually <5 cm)
- Valvulae conniventes visible (thin, complete transverse bands — "stacked coins")
- "Stepladder" air-fluid levels on erect view
- "String of beads" sign: small gas pockets trapped between folds in fluid-filled loops
- Paucity of colonic gas (collapsed distal bowel confirms obstruction)
CT is the definitive investigation — identifies the transition point (abrupt calibre change from dilated to collapsed bowel) and defines the cause.
Large Bowel Obstruction (LBO)
- Peripheral dilatation (haustrated colon around the abdominal frame)
- Diameter typically >5 cm (caecum is most vulnerable — >9 cm risks perforation)
- Site: ~60% due to sigmoid carcinoma; also diverticulitis, volvulus
| Entity | Appearance |
|---|---|
| Sigmoid volvulus | Inverted U-shaped loop, massively dilated, devoid of haustra; "liver overlap sign," "left flank overlap sign," "pelvic overlap sign" |
| Caecal volvulus | Distended caecum displaced toward left upper quadrant; attached gas-filled appendix sometimes visible |
Paralytic Ileus vs. Obstruction
| Feature | Mechanical Obstruction | Paralytic Ileus |
|---|---|---|
| Gas distribution | Dilated proximal + collapsed distal | Dilated throughout (small AND large bowel) |
| Transition point on CT | Present | Absent |
| Cause | Adhesion, hernia, tumour | Post-op, peritonitis, metabolic, drugs (opioids) |
7. Bowel Diameter Limits (Rules of 3, 6, 9)
| Segment | Upper limit of normal |
|---|---|
| Small bowel | 3 cm |
| Large bowel (general) | 6 cm |
| Caecum | 9 cm (higher → impending perforation risk) |
8. Calcifications on AXR
| Location | Likely Structure |
|---|---|
| Right upper quadrant | Gallstones (~10% are radio-opaque), calcified liver lesions |
| Renal areas / ureters | Renal/ureteric calculi (80–90% radio-opaque) |
| Epigastrium | Pancreatic calcification (chronic pancreatitis) |
| Pelvis | Phleboliths (common/benign), uterine fibroids, bladder stones |
| Vascular (curvilinear) | Aortic / iliac artery calcification, aortic aneurysm |
9. Soft Tissue Landmarks
- Psoas shadows: bilateral fusiform density along lumbar spine — loss suggests retroperitoneal pathology (bleeding, infection, AAA)
- Liver/spleen: enlarged if extending below the costal margin
- Kidneys: normally visible in the loin (right lower than left); renal outlines lost in retroperitoneal disease
- Bladder: pelvic soft tissue density; should be empty for a good AXR
10. AXR in Special Conditions
Acute Pancreatitis (Sleisenger & Fordtran's)
- Sentinel loop: focal ileus of a small bowel loop adjacent to inflamed pancreas
- Colon cut-off sign: spasm of the transverse/descending colon with air cut-off at the splenic flexure
- Pancreatic calcification → chronic pancreatitis
Toxic Megacolon
- Transverse colon dilated >6 cm with loss of haustral pattern + "mucosal islands" (pseudopolyps)
- Complication of UC, Crohn's, infectious colitis — surgical emergency
11. AXR Limitations — When to go to CT
| Situation | Preferred modality |
|---|---|
| Appendicitis | CT (or US in children/pregnancy) |
| Diverticulitis | CT |
| Cholecystitis | Ultrasound |
| Pancreatitis staging | CT (contrast-enhanced) |
| Confirm perforation when CXR equivocal | CT (lung windows) |
| Confirm SBO + define cause | CT |
- Grainger & Allison's Diagnostic Radiology, Ch. 18
- Harriet Lane Handbook (23rd ed.), Ch. 26
- Sleisenger & Fordtran's GI and Liver Disease, Ch. on Pancreatitis
Ct 101
CT scan abdomen axial slice anatomy liver spleen kidneys labelled
CT Hounsfield units window level bone lung soft tissue window settings
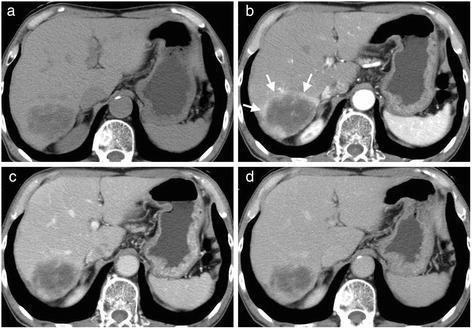
CT contrast phases arterial portal venous delayed enhancement liver timing
CT (Computed Tomography) 101
1. How CT Works
2. Hounsfield Units (HU) — The Language of CT
| Tissue / Material | HU Range |
|---|---|
| Air | −1000 |
| Fat | −100 to −50 |
| Water | 0 |
| Soft tissue / muscle | +20 to +80 |
| Blood (acute haemorrhage) | +50 to +90 |
| Calcification / bone | +130 to +1000 |
| Dense cortical bone | ~+1000 |
| Iodinated contrast (vessels) | +150 to +400 |
Practical rules: Fat is black (negative HU), water is mid-grey (0 HU), bone is bright white (+1000 HU). Anything brighter than expected soft tissue = calcification, contrast, or haemorrhage. Anything darker = fat or gas.
3. CT Windows — Seeing What You Want
- Window Level (WL) = the centre of the range you want to display (the "brightness")
- Window Width (WW) = the spread of the range (the "contrast")

| Window Preset | Level (WL) | Width (WW) | Used For |
|---|---|---|---|
| Soft tissue / abdomen | +40 | 350–400 | Organs, tumours, fluid |
| Lung | −600 | 1500 | Lung parenchyma, airways, pneumothorax |
| Bone | +700 | 2000–3000 | Fractures, cortical detail, spine |
| Brain | +35 | 80 | Intracranial haemorrhage, oedema |
| Subdural | +75 | 200 | Thin subdural collections |
| Liver | +60 | 160 | Hepatic lesions |
| Free gas | −600 | 1500 | Pneumoperitoneum (lung window on abdominal CT!) |
Key clinical point: Always view a suspected pneumoperitoneum on lung window settings — free gas invisible on soft-tissue windows becomes obvious on lung windows (Grainger & Allison's).
4. Contrast Media — Types, Phases, and Safety
Types of Contrast
| Type | Agent | Use |
|---|---|---|
| Iodinated IV contrast | Iohexol, iopromide, ioversol | CT vascular/organ enhancement |
| Oral contrast | Dilute iodine or barium | Bowel opacification |
| Rectal contrast | Dilute iodine | Pelvic/colorectal CT |
| Gadolinium | Gadopentetate | MRI (not CT — see NSF risk below) |
IV Contrast Phases
| Phase | Timing After Injection | What It Shows |
|---|---|---|
| Non-contrast (NCCT) | Before injection | Calcification, haemorrhage, fat, baseline attenuation |
| Arterial phase | ~25–35 s | Aorta, hepatic artery, hypervascular tumours (HCC, carcinoid), renal cortex |
| Portal venous phase | ~60–70 s | Portal vein, liver parenchyma (max enhancement), bowel wall, spleen |
| Delayed / nephrographic phase | ~90–120 s | Urothelial tumours, renal collecting system (CTU), abscess characterisation |
| Equilibrium / delayed | 3–15 min | Fibrotic lesions, cholangiocarcinoma, adrenal washout |
Wash-in / wash-out: HCC shows arterial hyperenhancement then portal phase washout — hallmark of HCC without biopsy. Haemangiomas show peripheral nodular enhancement with progressive fill-in.
Adrenal Washout Protocol (specific use case)
- Measure HU pre-contrast, at 60 s, and at 15 min
- Absolute contrast washout ≥60% → benign adenoma (sensitivity 86–88%, specificity 92–96%)
- Relative washout (post-contrast only) ≥40% → adenoma (sensitivity 96%, specificity 100%) (Grainger & Allison's)
5. Contrast Safety
Contrast-Induced Nephropathy (CIN) / Post-Contrast AKI (PC-AKI)
- Absolute creatinine rise >0.3 mg/dL (26.4 µmol/L), OR
-
50% rise in serum creatinine, OR
- Urine output <0.5 mL/kg/h for ≥6 hours
- CKD 3 (moderate impairment): IV hydration with 0.9% saline 100 mL/h starting 6–2 h before CT, continuing 4–12 h after
- CKD 4–5 (severe): avoid iodinated contrast where possible; use alternative modalities
- CIN is real but rare with modern low-osmolar agents in normal renal function
Allergic / Hypersensitivity Reactions
- Mild: nausea, flushing, urticaria — treat with antihistamine
- Moderate: bronchospasm, facial oedema — add corticosteroids
- Severe (anaphylaxis): hypotension, loss of consciousness — epinephrine, resuscitation
- Pre-medication with steroids + antihistamines for patients with prior moderate/severe reactions
Gadolinium Caution
- Nephrogenic Systemic Fibrosis (NSF): fibrocyte proliferation causing skin thickening, contractures, paraesthesia in patients with renal impairment
- Brain deposition: gadolinium accumulates in dentate nuclei, globus pallidus, thalamus with repeated doses — clinical significance still under study
- Linear GBCAs have marketing suspension in Europe; use macrocyclic agents preferentially
6. Anatomy of an Axial CT Slice — Orientation Rules
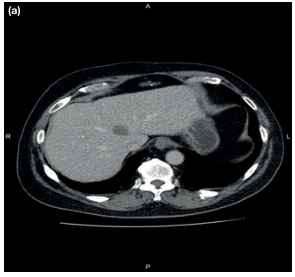
- Patient's right = viewer's left (and vice versa)
- Anterior structures are at the top
- Posterior structures (spine) are at the bottom
| Level | Landmarks |
|---|---|
| T10–T12 | Oesophagogastric junction, adrenals, upper kidneys |
| L1 | Coeliac axis, upper pole kidneys, pancreatic body/tail |
| L2 | SMA origin, renal hila, pancreatic head/uncinate |
| L3–L4 | Aortic bifurcation, iliac vessels |
| S1 | Sigmoid colon, distal ureters |
7. CT Reconstruction Planes and Techniques
| Format | Description | Use |
|---|---|---|
| Axial | Standard transverse slices | Default reading view |
| Coronal | Front-to-back reformats | Bowel, kidneys, abdominal overview |
| Sagittal | Side-to-side reformats | Spine, aorta, pelvic organs |
| MPR (Multiplanar Reconstruction) | Any oblique plane | Vessels, ducts, operative planning |
| MIP (Max Intensity Projection) | Highlights brightest voxels | CT angiography, urinary calculi |
| MinIP (Min Intensity Projection) | Highlights darkest voxels | Airways, emphysema |
| VR (Volume Rendering) | 3D surface model | Surgical planning, patient communication |
8. Systematic Approach to Reading an Abdominal/Pelvic CT
- Check the basics: patient name/DOB, date, scan phase (contrast vs. non-contrast), view plane
- Lung bases (if included): effusions, consolidation, free air under diaphragm
- Liver: size, attenuation, focal lesions, biliary dilatation
- Gallbladder & bile ducts: calculi, wall thickening, pericholecystic fluid
- Spleen: size (normal <12 cm), focal lesions
- Pancreas: size, ductal dilatation, peripancreatic fat stranding, calcification
- Adrenal glands: size (<10 mm limb width), nodules
- Kidneys & ureters: calculi, hydronephrosis, masses, enhancement pattern
- Bladder & pelvis: wall thickening, masses, lymphadenopathy
- Bowel: wall thickening, fat stranding, dilatation, transition points
- Vasculature: aortic diameter (<3 cm normal), iliac vessels, contrast fill
- Retroperitoneum: lymph nodes (>1 cm short axis = suspicious), fat stranding
- Bones: fractures, lytic/sclerotic lesions, vertebral alignment
- Free fluid / free gas: location, quantity
9. Common CT Findings and What They Mean
| Finding | Significance |
|---|---|
| Free gas | Perforated viscus (surgical emergency) |
| Free fluid (ascites) | Liver disease, malignancy, haemoperitoneum, infection |
| Fat stranding | Inflammation in adjacent tissue (appendicitis, diverticulitis, pancreatitis) |
| Bowel wall thickening | Inflammation, ischaemia, tumour, oedema |
| Target / halo sign | Benign mural oedema (IBD, radiation) |
| Transition point (dilated → collapsed) | Mechanical bowel obstruction |
| Pneumatosis intestinalis | Intramural gas — ischaemia (emergency) or benign |
| Portal venous gas | Ischaemic gut, very ominous |
| Hyperdense aorta | Acute intraluminal thrombus |
| Striated nephrogram | Pyelonephritis |
| Ring-enhancing lesion | Abscess, metastasis, primary brain tumour |
| Double duct sign | Pancreatic head mass (CBD + PD dilatation) |
10. Radiation Dose — Key Concepts
| Parameter | What It Is |
|---|---|
| mSv | Effective dose to patient |
| Typical CXR | ~0.02 mSv |
| Typical CT abdomen/pelvis | ~8–10 mSv |
| Typical CT chest | ~5–7 mSv |
| CTPA | ~5 mSv |
| ALARA principle | As Low As Reasonably Achievable — dose must be justified and optimised |
11. When to Use CT vs. Other Modalities
| Clinical Scenario | First Choice |
|---|---|
| Acute abdomen, haemodynamically stable | CT abdomen/pelvis with contrast |
| Suspected perforation | CT (or erect CXR) |
| Bowel obstruction characterisation | CT |
| Right iliac fossa pain (appendicitis) | US first, CT if equivocal |
| Renal colic | CT KUB (non-contrast) |
| Haematuria workup | CT Urogram (3 phases) |
| Pancreatitis severity staging | CECT at 48–72 h |
| Aortic aneurysm | CT angiography |
| Liver lesion characterisation | Multiphase CT ± MRI |
| Pregnancy / paediatrics | US or MRI preferred (no radiation) |
- Campbell-Walsh-Wein Urology, Ch. 3 — Hounsfield Units, CT technique
- Grainger & Allison's Diagnostic Radiology, Ch. 1 & 37 — Contrast phases, adrenal washout, CIN
- Brenner & Rector's The Kidney — CIN criteria and management
Ct Abdomen 101
Abdomen 101- preclinicals, clinically, diseases, investigations, management from cpg, nice
NICE guidelines acute abdomen appendicitis diverticulitis bowel obstruction management 2024 2025
NICE CG134 appendicitis NICE NG146 pancreatitis NICE NG147 diverticulitis management summary 2024
NICE guidance acute pancreatitis NG104 cholecystitis management 2024 BSG guidelines
NICE guidance cholecystitis gallstones management laparoscopic cholecystectomy 2024 2025
https://www.nice.org.uk/guidance/ng147/chapter/recommendatio…
Abdomen 101- preclinicals, clinically, diseases, investigations, management from cpg, nice
NICE guidelines appendicitis diverticulitis pancreatitis gallstones bowel obstruction management 2024 2025 summary
Generate a Word document with the full Abdomen 101 guide including anatomy, examination, diseases, investigations, and NICE/CPG management protocols
Intestinal Obstruction and perforation presentation
intestinal obstruction perforation clinical presentation signs symptoms NICE management 2024
small bowel obstruction management WSES guidelines 2024 strangulation surgical conservative criteria
Presentation: Clinical Features of Intestinal Obstruction + Neonatal Causes - Hema Cardinal features: History: Pain, vomiting, distension, constipation Examination: Distension, bowel sounds, dehydration Acute intestinal obstruction in newborn: Intestinal atresia Meconium ileus Meckel’s diverticulum Foreign body
Presentation: Presentation: Definition of intestinal obstruction ● Classification: ○ Dynamic (mechanical) ○ Adynamic (non-mechanical) ● Overview of importance and complications