NMJ with anaesthesia implications with scholine phase 1 ,2 block with other ndmr in details 50 mark question
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have all the material needed for a comprehensive 50-mark answer. Let me write it up.
Neuromuscular Junction (NMJ): Anatomy, Physiology, and Anaesthetic Implications - Including Succinylcholine Phase I & II Block and NDMRs
(50 Mark Model Answer)
PART 1: ANATOMY AND PHYSIOLOGY OF THE NMJ
Structure of the NMJ
The NMJ (motor end plate) is the synapse between the terminal branch of a somatic motor neuron and a skeletal muscle fiber. It has three key components:
1. Presynaptic (Nerve Terminal)
- The axon of the motor neuron carries electrical signals from the anterior horn of the spinal cord to the muscle
- The nerve terminal contains all apparatus for ACh synthesis, storage, and release
- Choline acetyltransferase synthesizes ACh from choline + acetyl-CoA (from mitochondria)
- ACh is stored in synaptic vesicles (quanta), of which there are two pools: a readily releasable pool (VP2, close to active zones) and a reserve pool (VP1, tethered to actin/cytoskeleton by synapsin, synaptotagmin, spectrin)
- SNARE proteins (synaptobrevin/VAMP) dock vesicles at active zones and mediate exocytosis
- The nerve terminal also contains P/Q-type voltage-gated calcium channels and potassium channels
2. Synaptic Cleft
- ~20 nm wide
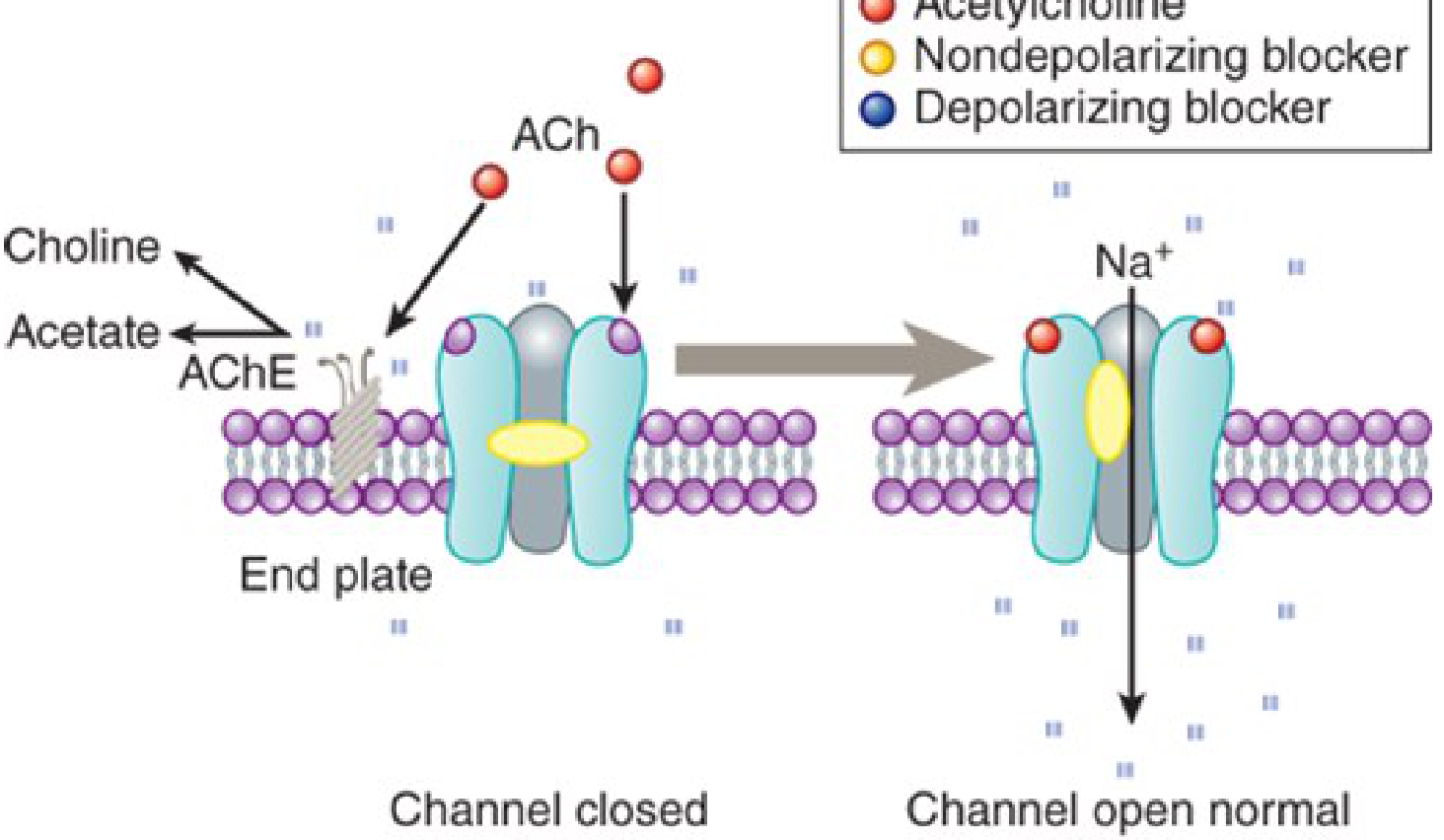
- Acetylcholinesterase (AChE) is densely anchored here - it hydrolyzes ACh into choline + acetate within milliseconds
- Choline is recycled back into the nerve terminal
3. Postsynaptic (Motor End Plate)
- The postjunctional membrane has deep junctional folds that greatly increase surface area
- Nicotinic ACh receptors (nAChR) are densely packed at 10,000/μm² at the crests of the folds
- AChE is located in the depths of the folds
The Adult nAChR - Molecular Structure
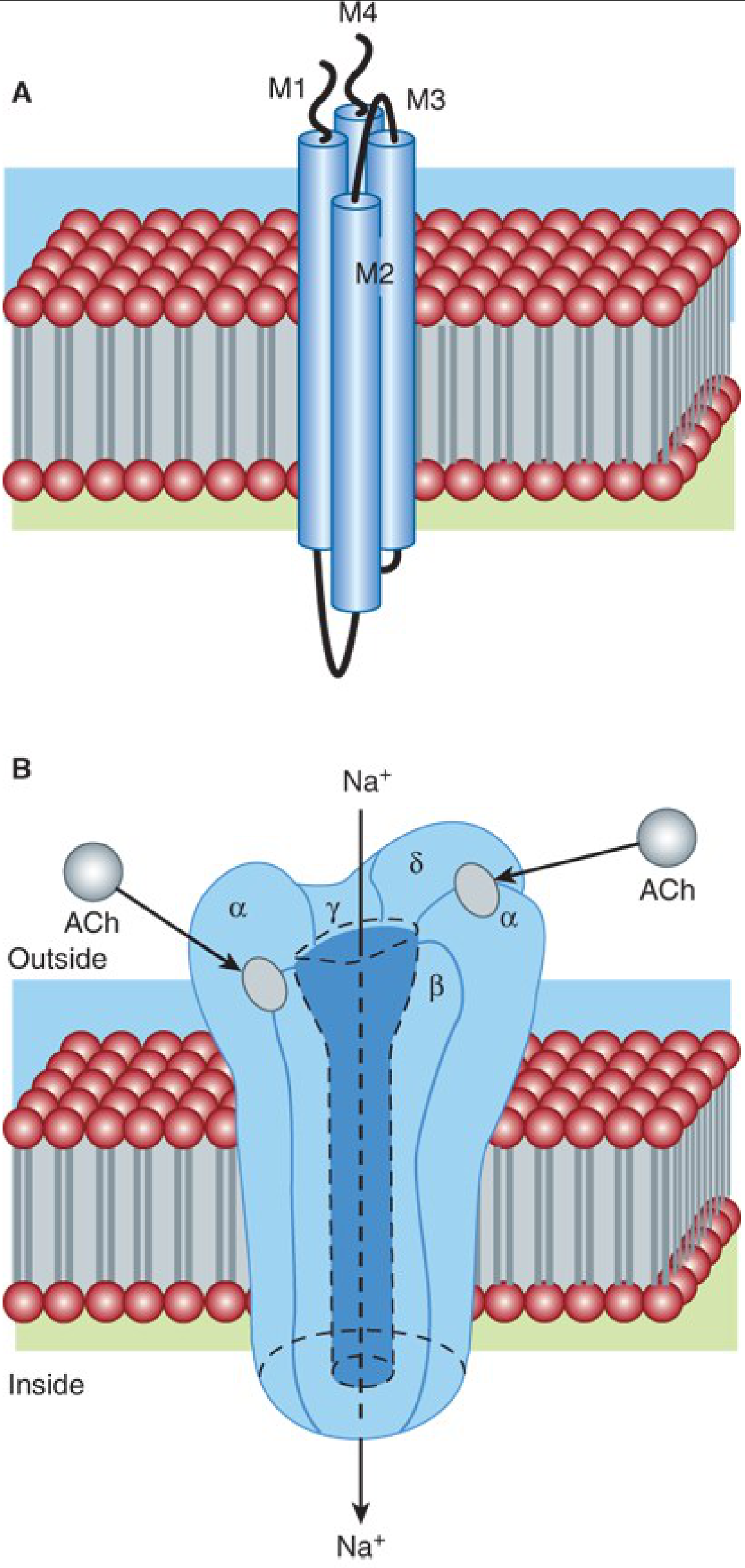
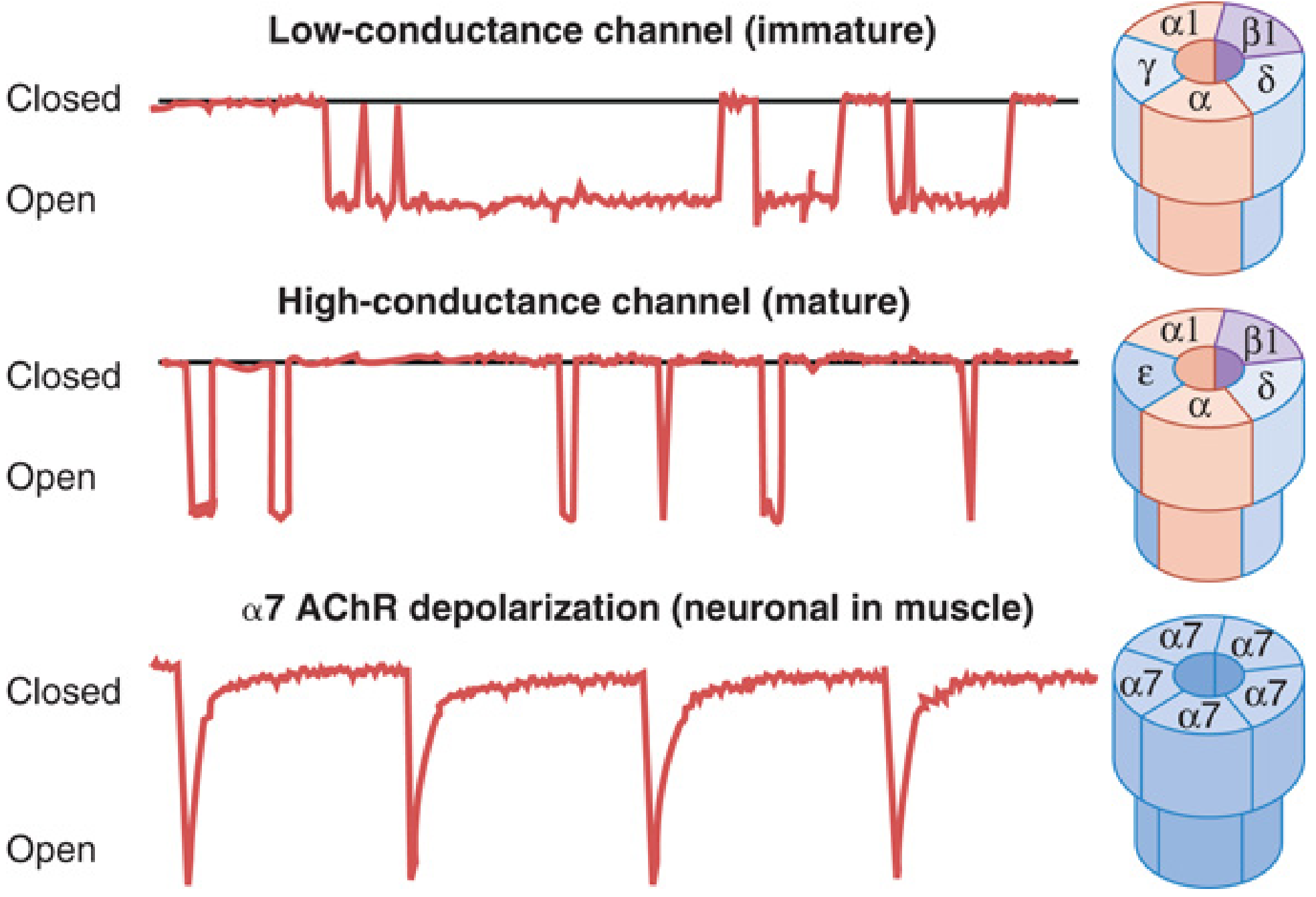
The adult/mature receptor is a pentamer of two α1-subunits, one β1, one δ, and one ε subunit (α₂β₁δε). Each subunit has four transmembrane helical domains (M1-M4); the M2 domains line the ion channel pore. The fetal/immature/extrajunctional receptor replaces the ε subunit with a γ subunit (α₂β₁δγ).
Key features:
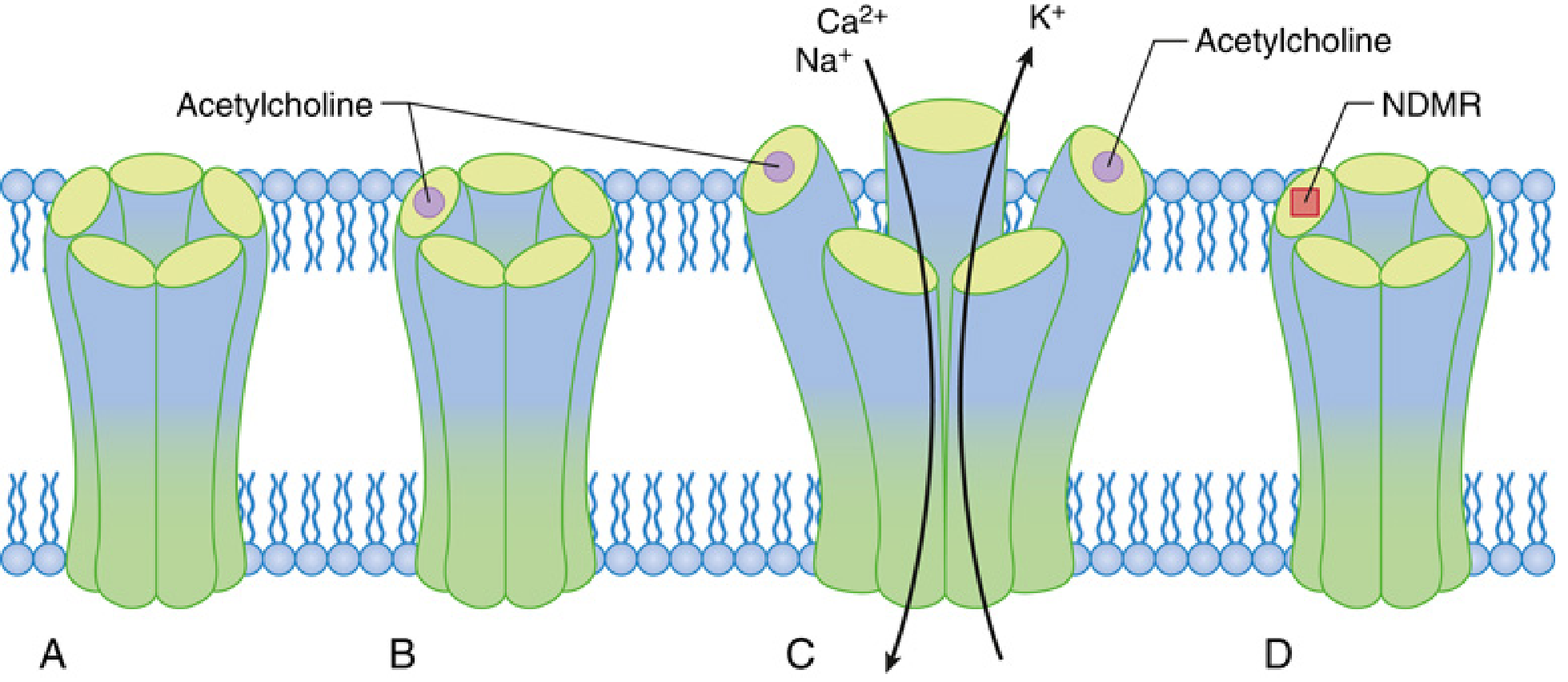
- Two ACh molecules must bind simultaneously to the α-β and δ-α subunit interfaces for channel opening
- Channel allows Na⁺ influx and K⁺ efflux → end-plate potential (EPP)
- If EPP exceeds threshold, an action potential propagates along the muscle membrane → excitation-contraction coupling → muscle contraction
- The margin of safety at the NMJ is large: ~75% of receptors can be blocked before muscle twitch is visibly depressed
Normal Neuromuscular Transmission - Step by Step
- Nerve action potential reaches terminal → Na⁺ influx → depolarization
- Voltage-gated P/Q-type Ca²⁺ channels open → Ca²⁺ enters nerve terminal
- Ca²⁺ triggers vesicle docking and exocytosis via SNARE proteins (synaptotagmin is Ca²⁺ sensor)
- ACh quanta released into cleft; diffuses to nAChRs
- Two ACh molecules bind to α subunits → channel opens → Na⁺/K⁺ flux → EPP
- EPP threshold exceeded → muscle action potential → contraction
- AChE rapidly hydrolyzes ACh → channel closes → repolarization → ready for next stimulus
Anaesthetic Relevance of Ca²⁺ at NMJ:
- Ca²⁺ concentration doubles → 16-fold increase in ACh quantal release
- Mg²⁺ (used in pre-eclampsia) competes with Ca²⁺ at P channels → decreases ACh release → potentiates NDMRs
- Calcium channel blockers (verapamil, diltiazem) have minimal effect on normal transmission but may potentiate NDMRs at high doses
Prejunctional Receptors
There are also α3-β2 nAChRs on the nerve terminal (prejunctional). During high-frequency stimulation (tetanus/TOF), these receptors are activated by ACh and facilitate mobilization and release of ACh from the reserve pool. This is why:
- NDMRs block these receptors → impair ACh mobilization during repetitive stimulation → fade on TOF/tetanus
- Depolarizing agents (high dose succinylcholine) also block these → cause fade in Phase II block
PART 2: NEUROMUSCULAR MONITORING
Before discussing block types, it is essential to understand monitoring, since block types are defined by their response to nerve stimulation.
Peripheral nerve stimulator (PNS) - applied to ulnar nerve, monitoring adductor pollicis; or facial nerve, monitoring orbicularis oculi.
| Stimulation Pattern | Description | Clinical Use |
|---|---|---|
| Train of Four (TOF) | 4 stimuli at 2 Hz, 0.5-second intervals | Intraoperative monitoring; TOF ratio = T4/T1 |
| Tetanic stimulation | 50-100 Hz for 5 sec | Assess depth; detects fade |
| Double burst stimulation | Two bursts of 3 tetanic stimuli | Better for detecting residual block by feel |
| Post-tetanic count (PTC) | Tetanus + count single twitches | Assesses deep block when no TOF response |
| Single twitch | 0.1 Hz | Simple twitch height comparison |
Residual block = TOF ratio <0.9, associated with aspiration risk, hypoxia, upper airway obstruction.
PART 3: DEPOLARIZING NEUROMUSCULAR BLOCKADE - SUCCINYLCHOLINE (Suxamethonium)
Structure and Pharmacokinetics
Succinylcholine = two ACh molecules joined back-to-back (bisquaternary). Dose: 1-1.5 mg/kg IV.
Metabolism: Rapidly hydrolyzed by plasma/pseudocholinesterase (butyrylcholinesterase) in plasma and liver:
- Succinylcholine → succinylmonocholine + choline → succinic acid + choline
- Only a small fraction reaches the NMJ (enzyme has enormous capacity)
- NOT hydrolyzed by AChE at the end plate
- Duration 5-10 minutes; block terminated by diffusion away from end plate
Dibucaine Number:
- Dibucaine inhibits normal pseudocholinesterase by 80% (dibucaine number ~80)
- Atypical enzyme: dibucaine number ~20 → succinylcholine duration dramatically prolonged (hours)
- Heterozygous: dibucaine number ~40-60 → moderately prolonged
- Clinical implication: family history of prolonged apnoea after suxamethonium warrants pseudocholinesterase activity and dibucaine number testing
PHASE I BLOCK (Depolarizing Block)
Mechanism:
Succinylcholine acts as an ACh agonist at the nAChR - it is not a competitive antagonist. Because it is structurally similar to ACh (two linked ACh molecules), it binds to the α-subunit ACh recognition sites, opens the channel, and causes depolarization of the end plate.
Key difference from ACh: succinylcholine is resistant to hydrolysis by AChE, so it persists in the cleft, repeatedly binding and re-binding, causing sustained end-plate depolarization.
Sequence of Events in Phase I Block:
- Succinylcholine binds nAChR → channels open → EPP generated → muscle fasciculations (unsynchronized contraction of motor units)
- Voltage-dependent gates of adjacent perijunctional sodium channels open (initial muscle contraction visible as fasciculations)
- Because succinylcholine is not cleared, end plate remains continuously depolarized
- The time-dependent inactivation gate of perijunctional Na⁺ channels closes ("accommodation")
- Na⁺ cannot flow through inactivated channels → no propagation of action potential beyond junctional zone
- The perijunctional zone becomes a buffer, shielding distal muscle membrane
- Result: flaccid paralysis despite end plate being depolarized
The muscle membrane separates into three zones:
- End plate - depolarized by succinylcholine
- Perijunctional zone - Na⁺ channels in inactivated state
- Distal muscle - Na⁺ channels in resting state (can be stimulated directly by electricity)
Characteristics of Phase I Block:
| Feature | Phase I Block |
|---|---|
| End-plate membrane potential | Depolarized (resting state lost) |
| Fasciculations | Present at onset |
| Single twitch height | Reduced |
| TOF | No fade (T1=T2=T3=T4, all reduced proportionally) |
| TOF ratio | Normal (>0.7) |
| Tetanic stimulation | Sustained (no fade) |
| Post-tetanic potentiation | Absent |
| Anticholinesterases | Augment (worsen) the block |
| Effect on depolarizing block | Augmented by nondepolarizers (pretreatment converts to dual block) |
Direct electrical stimulation of muscle: Produces contraction (because distal Na⁺ channels are in resting state) - this differentiates depolarizing block from denervation.
PHASE II BLOCK (Desensitization / Dual Block)
When succinylcholine is given in high doses or by prolonged infusion, the character of blockade changes. The initial depolarizing (Phase I) block transitions to a Phase II block, which has characteristics mimicking a nondepolarizing block.
Definition: Phase II block is a complex phenomenon that develops during prolonged or repeated exposure to depolarizing agents, in which the end-plate membrane repolarizes but becomes unresponsive to further depolarization.
Mechanism - Multiple Contributing Factors:
-
Desensitization: The nAChR undergoes conformational change to a desensitized (closed-channel) state despite agonist occupation. In the desensitized state, the channel is closed and cannot be opened even when the agonist is bound. The receptor has high affinity for agonist but zero functionality. Desensitization may occur very rapidly (milliseconds after agonist exposure) or slowly.
-
Prejunctional receptor block: High concentrations of succinylcholine block the prejunctional α3-β2 nAChRs → impaired ACh mobilization → fade on tetanic/TOF stimulation (similar to NDMRs)
-
Channel block: Succinylcholine, as a slender molecule, can enter the open channel and physically block ion flow (open-channel block) - use-dependent, not reversed by anticholinesterases
-
Receptor internalisation: With very prolonged exposure, receptor downregulation may occur
Conditions that promote Phase II block:
- Total succinylcholine dose >3-4 mg/kg
- Prolonged infusion
- Volatile anaesthetics (halothane, isoflurane)
- Certain antibiotics (aminoglycosides)
- Local anaesthetics
- Phenothiazines
- Calcium channel blockers
- Pre-existing neuromuscular disease
Characteristics of Phase II Block:
| Feature | Phase II Block |
|---|---|
| End-plate membrane potential | Repolarized (but unresponsive) |
| Fasciculations | Absent |
| Single twitch height | Reduced |
| TOF | Fade present (T1>T2>T3>T4) - like NDMR |
| Tetanic stimulation | Fade present (unsustained) |
| Post-tetanic potentiation | Present |
| Anticholinesterases | May partially reverse (variable - cautious use) |
Comparison Table: Phase I vs Phase II Block
| Feature | Phase I (Depolarizing) | Phase II (Desensitization) |
|---|---|---|
| Onset | Immediately with succinylcholine | After prolonged/high-dose succinylcholine |
| Fasciculations | Yes | No |
| TOF fade | No | Yes (like NDMR) |
| Tetanic fade | No | Yes |
| Post-tetanic potentiation | Absent | Present |
| Cholinesterase inhibitors | Worsen block | May partially reverse |
| Membrane potential | Depolarized | Repolarized (desensitized) |
Management of Phase II Block:
- Discontinue succinylcholine infusion
- Confirm by nerve stimulator (TOF with fade)
- Controlled ventilation and wait for spontaneous recovery
- Neostigmine may be tried cautiously if TOF fade is well established and TOF ratio is improving but still <0.9 - effect is unpredictable; may transiently worsen before improving
- Most important: identify at-risk patients before using succinylcholine infusions
Clinical Implication - NDMR following Succinylcholine:
After a single intubating dose of succinylcholine (Phase I block), subsequent NDMRs show increased sensitivity (reduced dose requirements). This is because:
- Residual desensitized receptors from succinylcholine reduce the margin of safety
- Fewer functional receptors are available for NDMR to overcome
PART 4: NON-DEPOLARIZING MUSCLE RELAXANTS (NDMRs)
Mechanism of Action
NDMRs act as competitive antagonists at the nAChR. They bind to the α-subunit recognition sites (same sites as ACh) but do not open the channel. Since both α-subunit sites must be occupied by ACh for channel opening, occupation of even one site by an NDMR is sufficient to prevent channel activation.
At higher concentrations, many NDMRs (e.g., tubocurarine, gallamine) also enter the channel and cause channel block - this is not reversed by anticholinesterases.
The relationship between NDMR and ACh is competitive - increasing ACh concentration (via anticholinesterases) can displace and reverse NDMR block. However, if NDMR concentration is doubled, ACh must quadruple to compete; this is why deep blocks are harder to reverse.
Classification of NDMRs
By Chemical Structure:
| Class | Drugs | Onset | Duration |
|---|---|---|---|
| Steroidal | Pancuronium, Vecuronium, Rocuronium, Pipecuronium | Varies | Long/Intermediate |
| Benzylisoquinoline | d-Tubocurarine, Atracurium, Cisatracurium, Mivacurium, Metocurine | Varies | Long/Intermediate/Short |
By Duration:
| Duration | Drugs | Elimination t½ |
|---|---|---|
| Long-acting | Pancuronium, d-Tubocurarine | 90-120 min (clinical) |
| Intermediate | Vecuronium, Rocuronium, Atracurium, Cisatracurium | 30-60 min |
| Short-acting | Mivacurium | 15-20 min |
Individual NDMRs - Pharmacology and Anaesthetic Implications
1. PANCURONIUM
- Dose: ED95 ~0.07 mg/kg; intubation 0.1 mg/kg
- Onset: 3-5 min | Duration: 60-90 min (long-acting)
- Metabolism/Elimination: 80% renal; 10-20% hepatic
- Side effects:
- Tachycardia and hypertension - due to vagolytic effect (muscarinic M2 blockade at SA node) and sympathomimetic (norepinephrine reuptake inhibition)
- Minimal histamine release
- Implications: Avoid in patients with ischaemic heart disease, hypertension; prolonged in renal/hepatic failure; cost-effective long-acting agent
2. VECURONIUM
- Dose: ED95 ~0.05 mg/kg; intubation 0.1 mg/kg
- Onset: 2-3 min | Duration: 25-40 min (intermediate)
- Metabolism: Hepatic (primarily) - 3-desacetyl vecuronium is active metabolite (~80% potency)
- Elimination: Biliary (60%) > renal (40%)
- Side effects:
- No vagolytic effect - cardiovascular stability (ideal in cardiac surgery, elderly)
- No histamine release
- Implications: Prolonged in hepatic failure; 3-desacetyl metabolite accumulates in ICU patients → prolonged weakness; reversed by neostigmine or sugammadex
3. ROCURONIUM
- Dose: ED95 ~0.3 mg/kg; intubation 0.6 mg/kg (RSI: 1.2 mg/kg)
- Onset: 60-90 seconds at 0.6 mg/kg; 60 seconds at 1.2 mg/kg - fastest NDMR onset
- Duration: 30-60 min (intermediate)
- Elimination: Primarily biliary/hepatic; 10-25% renal
- Side effects:
- Slight vagolytic tendency at high doses
- Minimal histamine release
- Pain on injection
- Anaesthetic Implications:
- The only NDMR that can substitute for succinylcholine in RSI (at 1.2 mg/kg, onset comparable)
- Uniquely reversible by sugammadex at any depth of block
- Prolonged in hepatic failure
- Widely used for maintenance relaxation
4. ATRACURIUM
- Dose: ED95 ~0.23 mg/kg; intubation 0.4-0.5 mg/kg
- Onset: 2-3 min | Duration: 25-35 min
- Unique Metabolism: Hofmann Elimination + Ester Hydrolysis
- Hofmann elimination - spontaneous non-enzymatic degradation at physiological pH and temperature (temperature and pH dependent)
- Produces laudanosine (a CNS stimulant - theoretical seizure risk at very high doses; not clinically significant in standard doses)
- No dependence on renal or hepatic function
- Side effects:
- Histamine release (dose-dependent) - can cause bronchospasm, hypotension, flushing; give slowly
- Implications: Drug of choice in patients with significant renal AND hepatic failure; hypothermia prolongs block (Hofmann slowed); avoid rapid IV bolus
5. CISATRACURIUM
- Dose: ED95 ~0.05 mg/kg; intubation 0.15-0.2 mg/kg
- Onset: 3-5 min | Duration: 40-75 min
- Metabolism: Hofmann elimination (primarily; ~80%); minimal ester hydrolysis
- One of 10 isomers of atracurium; 3-4x more potent than atracurium
- Side effects:
- Negligible histamine release - preferred over atracurium in asthmatics/atopic patients
- Less laudanosine production (lower doses used)
- Implications: Preferred for organ failure patients, ICU (least histamine release, organ-independent elimination), prolonged mechanical ventilation
6. MIVACURIUM
- Dose: ED95 ~0.08 mg/kg; intubation 0.15-0.2 mg/kg
- Onset: 2-3 min | Duration: 15-20 min (shortest-acting NDMR)
- Metabolism: Plasma cholinesterase (pseudocholinesterase) - like succinylcholine
- Side effects:
- Histamine release (dose-dependent) if given rapidly
- Prolonged in pseudocholinesterase deficiency (same risk as succinylcholine)
- Implications: Useful for short procedures where tracheal intubation is needed but succinylcholine is contraindicated; no need for reversal in most cases; avoid in pseudocholinesterase deficiency
Factors Modifying NDMR Response
Factors that POTENTIATE (prolong/deepen) NDMR block:
- Volatile anaesthetics (isoflurane > enflurane > halothane > N₂O) - potentiate dose-dependently
- Aminoglycoside antibiotics (competitive at NMJ + reduce presynaptic Ca²⁺ entry)
- Hypokalemia, hypermagnesaemia, hypocalcaemia, acidosis, hypothermia
- Renal failure (pancuronium, vecuronium, rocuronium)
- Hepatic failure (vecuronium, rocuronium, pancuronium)
- Prior succinylcholine (desensitization → enhanced sensitivity)
- Myasthenia gravis (reduced functional receptors → exquisite sensitivity)
Factors that REDUCE (antagonize) NDMR block:
- Prior burns/immobilisation/denervation (upregulation of extrajunctional receptors including γ-subunit and α7 receptors)
- Upper motor neuron lesions
- Carbamazepine (chronic use induces receptor changes)
- Alkalosis, hypercalcaemia, hyperkalaemia
Reversal of NDMRs
Anticholinesterases
- Neostigmine (0.04-0.07 mg/kg) + glycopyrrolate; or pyridostigmine
- Inhibit AChE → accumulation of ACh → competitive displacement of NDMR
- Only effective at moderate block - deep block (TOF count <2, PTC <10) cannot be reliably reversed
- Ceiling effect: cannot produce more ACh than the system can provide
- Always co-administer anticholinergic (glycopyrrolate 0.2 mg per 1 mg neostigmine) to prevent muscarinic effects (bradycardia, bronchospasm, hypersalivation)
Sugammadex - Cyclodextrin Encapsulation
- Modified γ-cyclodextrin that encapsulates rocuronium and vecuronium (steroidal NDMRs) in a 1:1 ratio with high affinity
- Reduces free plasma NDMR → concentration gradient causes NDMR to diffuse away from NMJ into plasma → immediate reversal
- Key advantage: Works at ANY depth of block (unlike neostigmine)
- 2 mg/kg for shallow block (spontaneous recovery to T2)
- 4 mg/kg for deep block (1-2 PTC, no TOF response)
- 16 mg/kg for immediate reversal after 1.2 mg/kg rocuronium (RSI reversal)
- No muscarinic effects; no ceiling
- Adverse effects: hypersensitivity/anaphylaxis (rare), bradycardia
- Renal failure: sugammadex-rocuronium complex excreted renally; complex is stable and inactive, but elimination delayed - use with caution in severe renal impairment
PART 5: SPECIFIC ANAESTHETIC IMPLICATIONS OF SUCCINYLCHOLINE (BEYOND PHASE I/II)
Contraindications and Hazards
1. Hyperkalaemia
Normal succinylcholine → K⁺ rises ~0.5 mEq/L (safe in normokalemia).
In pathological upregulation of extrajunctional receptors, massive K⁺ efflux → potentially lethal cardiac arrest.
Absolute contraindications for succinylcholine (hyperkalaemia risk):
- Burns (>24-48 hours old, until fully healed - peak risk 7-10 days)
- Massive trauma/crush injury (>24-48 hours)
- Spinal cord injury (>24-48 hours - extrajunctional upregulation)
- Prolonged immobilisation
- Denervating conditions: Guillain-Barré, severe Parkinson's, stroke, encephalitis, tetanus
- Myopathies: Duchenne muscular dystrophy (high risk of rhabdomyolysis too)
- Severe intraabdominal infection/sepsis (>3-5 days)
Note: Risk is minimal in the first 24-48 hours after injury.
2. Malignant Hyperthermia (MH)
- Succinylcholine is a trigger for MH along with all volatile agents
- MH: autosomal dominant disorder (RYR1 mutations); uncontrolled Ca²⁺ release from sarcoplasmic reticulum → hypermetabolic state
- Management: stop trigger, dantrolene 2.5 mg/kg IV (blocks RyR1)
- Succinylcholine should never be used routinely in paediatric patients (unknown myopathy risk)
3. Raised Intraocular Pressure (IOP)
- Extraocular muscles are tonic/multiply innervated; lack accommodation
- Succinylcholine → sustained contracture of extraocular muscles → IOP rises 6-12 mmHg
- Relative contraindication in penetrating eye injury (though risk of aspiration in full stomach may outweigh IOP risk)
- Alpha-conotoxin-sensitive conventional AChRs + desensitization-resistant receptors on extraocular muscles explain this
4. Raised Intragastric Pressure
- Abdominal fasciculations → raised intragastric pressure
- However, concurrent rise in lower oesophageal sphincter tone prevents increased regurgitation risk - no net increase in aspiration risk
5. Raised Intracranial Pressure
- Muscle fasciculations → transient rise in ICP via raised intrathoracic and venous pressure
- Precurarisation (small dose NDMR 3-5 min before) reduces fasciculations
6. Postoperative Myalgia
- Unsynchronised fasciculations cause myoglobinemia and muscle pain (especially in young ambulatory patients)
- Reduced by: precurarisation with rocuronium 0.06 mg/kg, pretreatment with NSAIDs or benzodiazepines
7. Bradycardia
- Succinylcholine can cause sinus bradycardia (especially in children, or with repeated doses) via muscarinic stimulation
- Prevented by atropine (0.02 mg/kg IV pre-treatment in children)
8. Prolonged Apnoea
- Pseudocholinesterase deficiency (genetic or acquired: liver disease, renal disease, malnutrition, pregnancy, echothiophate eye drops, organophosphate poisoning)
- Management: controlled ventilation until spontaneous recovery; fresh frozen plasma (contains pseudocholinesterase)
PART 6: CLINICAL PHARMACOLOGY COMPARISON TABLE
| Property | Succinylcholine | Rocuronium | Vecuronium | Atracurium | Cisatracurium | Pancuronium | Mivacurium |
|---|---|---|---|---|---|---|---|
| Type | Depolarizing | NDMR | NDMR | NDMR | NDMR | NDMR | NDMR |
| Onset | 60 sec | 60-90 sec | 2-3 min | 2-3 min | 3-5 min | 3-5 min | 2-3 min |
| Intubation dose | 1-1.5 mg/kg | 0.6 mg/kg | 0.1 mg/kg | 0.4-0.5 mg/kg | 0.15-0.2 mg/kg | 0.1 mg/kg | 0.15-0.2 mg/kg |
| Duration | 5-10 min | 30-60 min | 25-40 min | 25-35 min | 40-75 min | 60-90 min | 15-20 min |
| Metabolism | Plasma ChE | Hepatic/biliary | Hepatic/biliary | Hofmann + ester | Hofmann | Renal (80%) | Plasma ChE |
| Histamine | None | None | None | Yes (moderate) | Minimal | None | Yes (mild) |
| Vagal effect | Stimulation (bradycardia) | Mild block (tachycardia) | None | None | None | Block (tachycardia) | None |
| Reversibility | Spontaneous | Neostigmine / Sugammadex | Neostigmine / Sugammadex | Neostigmine | Neostigmine | Neostigmine | Spontaneous/Neostigmine |
| Organ failure | Caution (pseudoChE) | Hepatic caution | Hepatic caution | Safe | Safe | Avoid renal/hepatic | Avoid pseudoChE def |
PART 7: SPECIAL SITUATIONS AND RECEPTOR UPREGULATION
Extrajunctional Receptor Upregulation
In burns, spinal cord injury, immobilisation, denervation, and sepsis, the immature (γ-subunit) AChR and α7 homomeric receptors are expressed throughout the muscle membrane (not just at the end plate). This has critical implications:
- Succinylcholine → catastrophic K⁺ release from these widespread receptors (absolute contraindication)
- Resistance to NDMRs - α7 receptors:
- Do not desensitize with choline
- Have lower affinity for NDMRs (require 3/5 subunits blocked to inhibit; conventional receptor needs only 1/2)
- Result: higher doses of NDMR needed; unpredictable responses
Myasthenia Gravis
- Autoimmune destruction of postjunctional nAChRs (antibodies to α subunit)
- Reduced receptor number → reduced safety margin
- Exquisitely sensitive to NDMRs (use 10-20% of normal dose, carefully titrated)
- Resistant to succinylcholine (fewer receptors to depolarize, but prolonged due to cholinesterase deficiency from pyridostigmine therapy)
Eaton-Lambert Myasthenic Syndrome
- Antibodies against presynaptic voltage-gated Ca²⁺ channels (P/Q type)
- Decreased ACh release
- Sensitive to BOTH depolarizing and nondepolarizing agents - use extreme caution, very small doses
ICU-Acquired Neuromuscular Weakness
- Prolonged NDMR infusion in ICU + corticosteroids → critical illness myopathy and neuropathy
- 3-desacetyl vecuronium (active metabolite of vecuronium) accumulates in renal failure
- Use peripheral nerve stimulator monitoring to prevent overdosing; cisatracurium preferred in ICU
SUMMARY POINTS FOR EXAM
-
NMJ transmits via ACh → nAChR (pentameric, 2 ACh required) → EPP → muscle contraction; margin of safety is large (75% blockade needed before twitch visible)
-
Succinylcholine Phase I = depolarizing block; fasciculations; no TOF fade; worsen with anticholinesterases; direct muscle stimulation works
-
Succinylcholine Phase II = desensitization/dual block after prolonged exposure; TOF fade present; resembles NDMR; may partially reverse with neostigmine; best managed with controlled ventilation
-
NDMRs = competitive antagonists; reversed by anticholinesterases (moderate block) or sugammadex (any depth, steroidal agents only)
-
Rocuronium 1.2 mg/kg + sugammadex 16 mg/kg = viable alternative to succinylcholine-based RSI
-
Succinylcholine contraindications: burns >48h, cord injury >48h, denervation, hyperkalaemia, MH susceptibility, myopathies
-
Atracurium/Cisatracurium = organ-independent elimination (Hofmann) → drug of choice in multi-organ failure
-
Mg²⁺ potentiates all neuromuscular blockers by reducing presynaptic Ca²⁺ entry; monitor closely in pre-eclamptic patients
-
Residual block (TOF ratio <0.9) is a real clinical hazard → aspiration, hypoxia; use nerve stimulator routinely and ensure TOF ratio >0.9 before extubation
Sources: Miller's Anesthesia 10e (Chapters 11, 24); Morgan & Mikhail's Clinical Anesthesiology 7e (Chapters 11-12); Katzung's Basic and Clinical Pharmacology 16e (Chapter 27)
Describe scholine and ndmr how they act on neuromuscular junction
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have all the textbook material and diagrams needed. Here is a clear, complete answer.
How Succinylcholine (Suxamethonium) and NDMRs Act on the NMJ
Quick Recap: The Normal NMJ
Before understanding how drugs interfere, recall the normal sequence:
- Nerve action potential → Ca²⁺ enters nerve terminal → ACh vesicles released
- ACh diffuses across cleft → binds to both α-subunits of the nAChR (pentameric: α₂βδε)
- Channel opens → Na⁺/Ca²⁺ influx, K⁺ efflux → end-plate potential (EPP)
- EPP exceeds threshold → muscle action potential → contraction
- Acetylcholinesterase (AChE) rapidly destroys ACh → channel closes → end plate repolarizes → ready for next impulse
The key rule: BOTH α-subunit sites must be simultaneously occupied by ACh for the channel to open. This single rule explains how both drug classes work.
SUCCINYLCHOLINE (Suxamethonium) - Depolarizing Agent
What it is structurally
Succinylcholine = two ACh molecules joined back to back (bisquaternary). Because of this resemblance, it can do exactly what ACh does - bind the α-subunits and open the channel.
Step-by-step action at the NMJ
Step 1 - Mimics ACh (Agonist action)
Succinylcholine binds to both α-subunits of the nAChR → channel opens → ions flow → end-plate depolarizes. This generates a wave of action potentials across the whole muscle, producing visible fasciculations (unsynchronised twitching of muscle groups).
Step 2 - Sustained depolarization (the key difference from ACh)
ACh is destroyed by AChE within milliseconds, so the end plate repolarizes quickly. Succinylcholine, however, is NOT hydrolysed by AChE. It is only cleared slowly by plasma pseudocholinesterase after diffusing away from the cleft. Because it persists in the cleft, it repeatedly re-binds and re-fires the receptor, keeping the end plate continuously depolarized.
Step 3 - Perijunctional sodium channel inactivation
The voltage-gated Na⁺ channels adjacent to the end plate (perijunctional zone) have two gates:
- A voltage-dependent activation gate (opens when depolarization occurs)
- A time-dependent inactivation gate (closes shortly after the activation gate opens)
With the end plate continuously depolarized, the inactivation gates of the perijunctional Na⁺ channels stay permanently closed - a state called accommodation. No further Na⁺ can flow, no action potential propagates beyond the junction → flaccid paralysis.
The muscle membrane is divided into 3 zones:
| Zone | State | Consequence |
|---|---|---|
| End plate | Continuously depolarized by succinylcholine | Not conducting |
| Perijunctional Na⁺ channels | Inactivated (frozen closed) | Acts as buffer |
| Distal muscle | Resting (excitable) | Responds to direct electrical stimulation |
Clinically important: Because distal muscle Na⁺ channels are in the resting state, direct electrical stimulation of muscle produces contraction even during succinylcholine paralysis. This distinguishes succinylcholine block from muscle disease.
Summary of succinylcholine action at NMJ
Succinylcholine → binds nAChR α-subunits (agonist)
↓
Channel opens → EPP → fasciculations
↓
Not destroyed by AChE → remains in cleft
↓
Sustained end-plate depolarization
↓
Perijunctional Na⁺ channel inactivation (accommodation)
↓
No action potential propagation → FLACCID PARALYSIS
Why anticholinesterases worsen Phase I succinylcholine block
Neostigmine inhibits AChE → more ACh accumulates in cleft → ACh competes with succinylcholine at the receptor → but ACh itself also keeps depolarizing the end plate → deepens, not reverses, the block. This is opposite to NDMR behaviour.
NDMRs (Non-Depolarising Muscle Relaxants)
What they are structurally
NDMRs are either steroidal (rocuronium, vecuronium, pancuronium) or benzylisoquinoline (atracurium, cisatracurium, mivacurium) compounds. They are bulky molecules that fit into the ACh binding pockets on the α-subunits but do not activate the receptor.
Step-by-step action at the NMJ
Step 1 - Competitive binding at α-subunits
NDMRs bind to one or both α-subunit recognition sites on the nAChR - the same sites where ACh binds. But unlike ACh or succinylcholine, NDMRs do not trigger the conformational change that opens the channel.
Step 2 - Prevention of channel opening
Remember: both α-subunit sites must be occupied by ACh simultaneously for the channel to open. If even one site is occupied by an NDMR, ACh cannot activate that receptor - the channel stays closed, no current flows, no EPP is generated.
Step 3 - Competitive, concentration-dependent block
The outcome (block or transmission) is a competition between:
- ACh (agonist - wants to open the channel)
- NDMR (antagonist - blocks the opening)
At moderate NDMR concentrations, many receptors are blocked → reduced total EPP → if EPP falls below threshold → no muscle contraction → paralysis, but with no fasciculations and no initial depolarization.
The large margin of safety at the NMJ means ~75% of receptors must be blocked before any visible twitch depression occurs.
Step 4 - Additional channel block at higher doses
Some NDMRs (e.g., tubocurarine, gallamine) can also physically enter the open ion channel and obstruct ion flow (channel block - open or closed). This effect is not at the ACh recognition site, so it is not reversed by anticholinesterases.
Why anticholinesterases reverse NDMR block
Neostigmine/pyridostigmine inhibit AChE → ACh accumulates in the cleft → more ACh molecules compete for the α-subunit binding sites → at high enough ACh concentration, ACh displaces the NDMR and re-occupies both α-subunits → channel reopens → transmission restored.
Mathematical relationship: If NDMR concentration doubles, ACh must increase fourfold to maintain competition. This is why deep NDMR blocks are harder to reverse with neostigmine - you need much more ACh to overcome high NDMR concentrations.
Summary of NDMR action at NMJ
NDMR → binds α-subunit(s) of nAChR (pure antagonist - no channel activation)
↓
ACh cannot occupy both α-subunits simultaneously
↓
Channel stays CLOSED
↓
No end-plate potential
↓
No muscle action potential → FLACCID PARALYSIS (no fasciculations)
↓
Reversed by: ACh accumulation (neostigmine) OR
cyclodextrin encapsulation (sugammadex for rocuronium/vecuronium)
Side-by-Side Comparison
| Feature | Succinylcholine (Depolarizing) | NDMRs (Non-Depolarizing) |
|---|---|---|
| Receptor action | Agonist (opens channel) | Antagonist (blocks channel opening) |
| Binding site | α-subunits of nAChR (same as ACh) | α-subunits of nAChR (same as ACh) |
| Initial effect | Depolarization → fasciculations | No depolarization, no fasciculations |
| End-plate state | Continuously depolarized | Resting (no depolarization) |
| Na⁺ channel state | Perijunctional channels inactivated | Normal (resting) |
| AChE hydrolysis | No (cleared by plasma pseudoChE) | No (cleared by redistribution/metabolism) |
| Anticholinesterases | Worsen block (more depolarization) | Reverse block (more ACh competes) |
| TOF response | No fade (T1=T2=T3=T4) | Fade present (T4 < T3 < T2 < T1) |
| Tetanic stimulation | Sustained (no fade) | Fade (unsustained) |
| Post-tetanic potentiation | Absent | Present |
| Reversed by sugammadex | No | Yes (rocuronium and vecuronium only) |
Why NDMRs Show TOF Fade but Succinylcholine Does Not
This is a key exam distinction:
-
NDMRs block prejunctional α3-nAChRs on the nerve terminal → impair ACh mobilization from the reserve pool during repetitive stimulation → progressively less ACh released with each stimulus → T4 < T3 < T2 < T1 = fade
-
Succinylcholine (Phase I) does not produce fade at clinical doses. The end plate is uniformly depolarized; each stimulus sees the same degree of block. The ACh release mechanism is not significantly impaired → no fade. Only in Phase II block (prolonged succinylcholine) does fade appear, because then prejunctional receptors also get blocked.
Sources: Miller's Anesthesia 10e, Chapter 11; Katzung's Basic and Clinical Pharmacology 16e, Chapter 27; Morgan & Mikhail's Clinical Anesthesiology 7e, Chapter 11
This is a shared conversation. Sign in to Orris to start your own chat.