Crush syndrome etiology pathology signs and symptoms investigation and treatment explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
crush syndrome rhabdomyolysis pathophysiology signs symptoms treatment diagrams
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Searching PubMed
crush syndrome rhabdomyolysis acute kidney injury treatment
Reading File
Reading File
Loading Image
I now have comprehensive information to write a complete, detailed, well-illustrated answer. Let me compose it.
Crush Syndrome: A Comprehensive Overview
Definition
Crush syndrome is the systemic manifestation of prolonged, severe crushing of skeletal muscle, leading to rhabdomyolysis, release of toxic intracellular contents into the circulation, and potentially life-threatening complications including acute kidney injury (AKI), hyperkalemia, metabolic acidosis, and multi-organ failure. It is distinguished from a simple crush injury (local tissue damage only) by its systemic sequelae.
"Crush syndrome is the body's systemic manifestations caused by crushed muscle tissue, and often occurs when blood flow is restored to the crushed tissue and toxins are released in the body's circulation." - Rosen's Emergency Medicine, 10th Ed.
Etiology
Crush syndrome develops when a large mass of skeletal muscle is subjected to prolonged compressive force. The threshold is approximately 4-6 hours of compression, though it can develop in as little as 1 hour depending on the force and affected muscle mass.
Traumatic Causes
| Category | Examples |
|---|---|
| Disasters | Earthquakes, building collapses, tsunamis, explosions |
| Industrial/occupational | Mining accidents, heavy machinery entrapment |
| Road traffic accidents | Vehicle entrapment |
| Military/war | Blast injuries, entrapment under rubble |
| Prolonged immobilization | Coma, fall victims unable to move, drug overdose |
| Electrical injury | High-voltage electrocution causing massive muscle necrosis |
| Burns | Severe burns destroying large muscle mass |
Non-traumatic Causes of Rhabdomyolysis (that can produce a similar syndrome)
- Seizures (sustained muscle contraction)
- Strenuous exercise (exertional rhabdomyolysis)
- Heatstroke / hyperthermia
- Malignant hyperthermia
- Neuroleptic malignant syndrome
- Drugs/toxins: statins, cocaine, heroin, alcohol, amphetamines, MDMA, CO poisoning
- Infections: influenza A/B, Coxsackievirus, S. pyogenes, S. aureus pyomyositis
- Metabolic disorders: hypokalemia, hypophosphatemia, hypocalcemia, DKA
- Inherited myopathies (recurrent episodes - suspect glycolytic/lipid metabolism disorders)
Epidemiology
- Crush syndrome occurs in 2-15% of all trauma patients
- Up to 30-40% of earthquake victims and survivors of multi-story building collapses
- First recognized clinically during the London Blitz (World War II) by Bywaters and Beall, 1941
Pathology and Pathophysiology
The central event is traumatic rhabdomyolysis - destruction of skeletal muscle with release of intracellular myocyte contents. Two overlapping mechanisms drive this:
1. Direct Compression Injury (During Entrapment)
- External force mechanically disrupts the sarcolemma (muscle cell membrane)
- Ischemia develops as microvascular compression cuts off O2 supply
- Anaerobic metabolism generates lactic acid → metabolic acidosis
- ATP depletion disables the Na+/K+-ATPase and Ca2+-ATPase pumps
2. Ischemia-Reperfusion Injury (Upon Extrication)
- The paradoxical exacerbation of injury when blood flow is restored
- Reactive oxygen species (ROS) and free radical generation
- Complement activation and neutrophil/platelet-endothelial interaction
- Cytokine release → local and systemic inflammatory response
Cellular cascade:
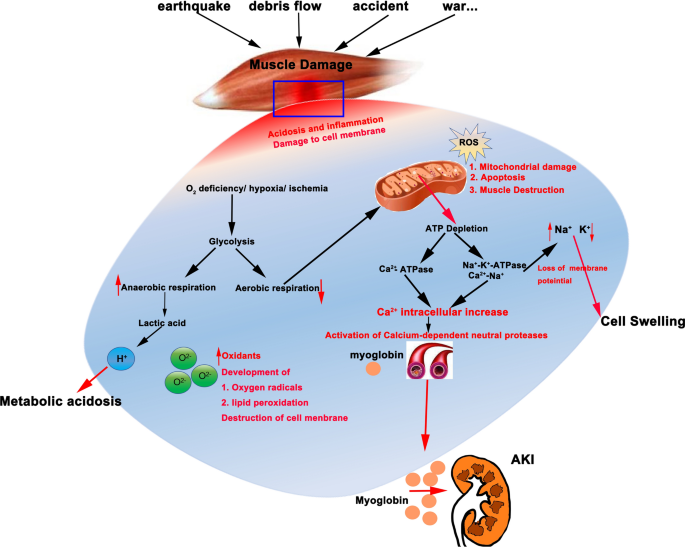
Cellular mechanisms: ATP depletion leads to Ca²⁺ influx, ROS generation, myoglobin release, and ultimately AKI. (From Springer Nature, 2025)
Key Toxic Substances Released
| Substance | Mechanism of harm |
|---|---|
| Myoglobin | Causes pigment nephropathy, tubular obstruction, ferrihemate formation → free hydroxyl radicals → lipid peroxidation; direct tubular cell toxicity |
| Potassium (K+) | Massive hyperkalemia → cardiac arrhythmias, ventricular fibrillation, cardiac arrest |
| Phosphate | Hyperphosphatemia → precipitates in distal tubules → worsens AKI; also causes secondary hypocalcemia |
| Creatine kinase (CK) | Marker of muscle damage; correlates with AKI risk |
| Uric acid | Precipitates in distal tubules in acid urine → tubular obstruction and nephrotoxicity |
| Lactic acid | Metabolic acidosis → aggravates arrhythmogenicity and coagulopathy |
| Thromboplastin | Triggers DIC (disseminated intravascular coagulation) |
| Calcium (Ca²⁺) | Intracellular Ca²⁺ activates proteases and phospholipases → further myocyte destruction |
Pathogenesis of Renal Failure (Most serious complication)
The mechanism is multifactorial:
- Pre-renal AKI: Hypovolemia from fluid sequestration into crushed muscle (third-spacing) → reduced renal perfusion pressure
- Intrinsic AKI - Tubular obstruction: Myoglobin and uric acid precipitate in distal tubules, especially in acidic urine (pH < 5.6)
- Intrinsic AKI - Direct nephrotoxicity: Myoglobin forms ferrihemate, which generates hydroxyl radicals via Fenton reaction → oxidative tubular injury; acidic urine promotes dissociation of myoglobin into nephrotoxic ferriheme
- Renal vasoconstriction: Activated renin-angiotensin system, hypovolemia, and inflammatory mediators reduce GFR
- Macrophage extracellular traps: Recent research shows platelet-activated macrophages form METs that are pathogenic in rhabdomyolysis-induced AKI
Compartment Syndrome (local complication)
Normal compartment pressure = <10 mmHg
After crush injury:
- Microvascular trauma → edema + interstitial bleeding within a closed fascial space
- Myocytes lose ability to retain intracellular water → further edema
- Rising pressure > 30 mmHg compresses microvasculature → muscle ischemia
- Irreversible nerve and muscle damage after 4-6 hours of ischemia
Full Pathophysiology Flowchart
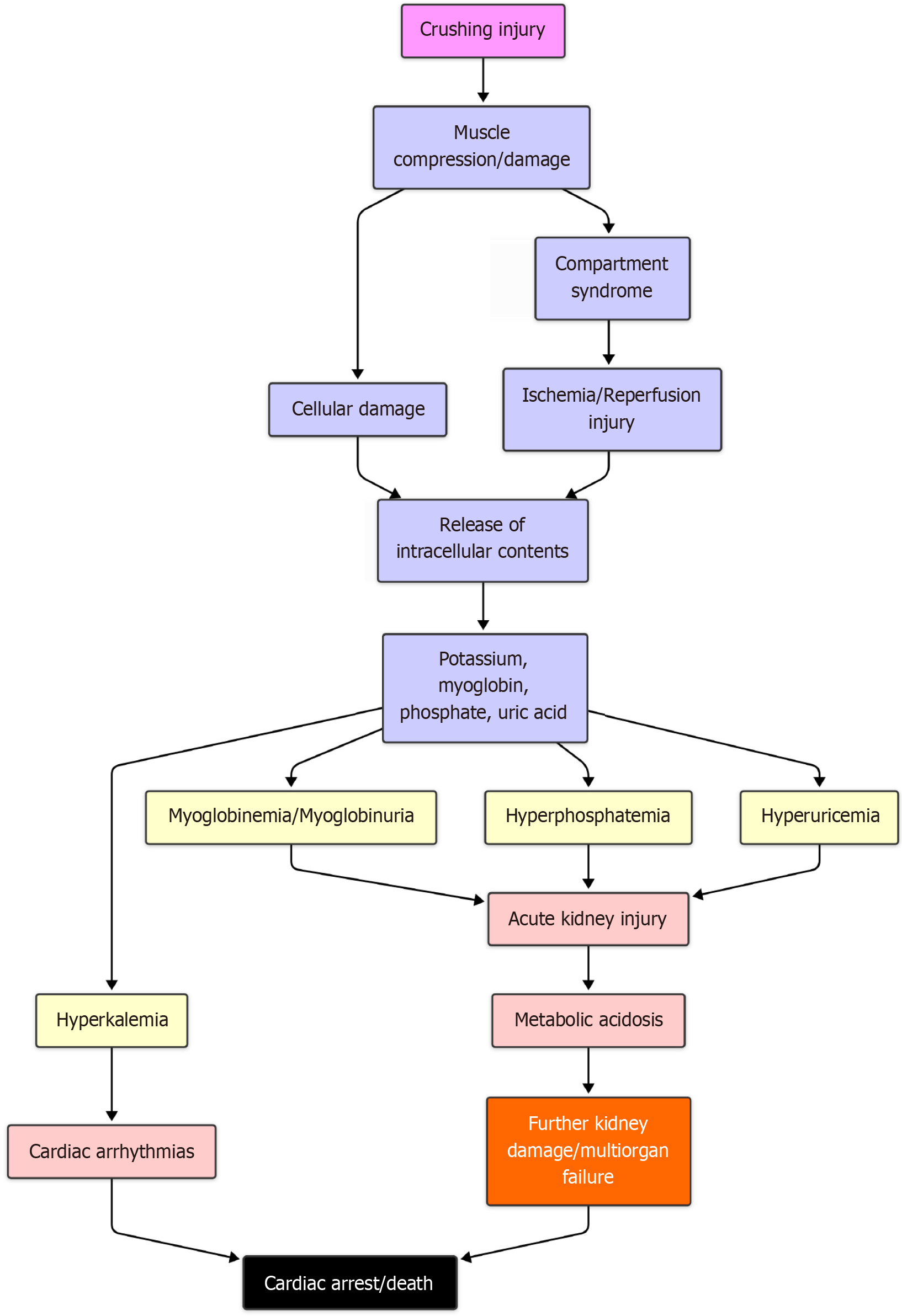
From crushing injury through rhabdomyolysis to cardiac arrest/death via hyperkalemia, AKI, and metabolic acidosis.
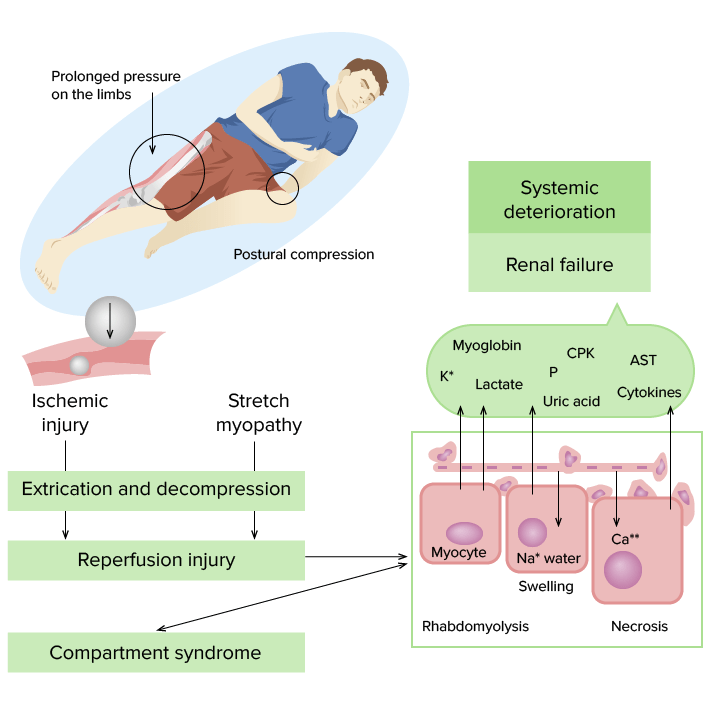
Ischemic injury + stretch myopathy → reperfusion injury → rhabdomyolysis and compartment syndrome → systemic deterioration and renal failure. (Lecturio Medical)
Signs and Symptoms
Local (Limb) Findings
- Swollen, tense, firm limb - due to edema and third-spacing of fluid
- Skin changes: ecchymosis, blistering, pressure necrosis, degloving injuries, lacerations
- Pain out of proportion to apparent injury (hallmark of developing compartment syndrome)
- Paresthesias: numbness, tingling, burning in the affected limb (nerve compression/ischemia)
- Weakness or paralysis of the compressed segment
- Pulselessness (late sign - major vessels often unaffected early; it is a microvasculature disorder)
The "5 Ps" of Compartment Syndrome
- Pain (most consistent - out of proportion, worsened by passive stretch)
- Paresthesias (earliest neurological sign)
- Passive stretch pain (pain on passive movement of muscles in the compartment)
- Pressure (palpably tense compartment)
- Pulselessness (late and unreliable)
Systemic Findings
| System | Manifestations |
|---|---|
| Cardiovascular | Hypovolemic shock (tachycardia, hypotension); cardiac arrhythmias (PVCs, VT, VF) from hyperkalemia/acidosis; cardiac arrest |
| Renal | Oliguria/anuria (early warning sign); dark reddish-brown urine (myoglobinuria - "tea-colored" or "Coca-Cola" urine); acute tubular necrosis; renal failure |
| Metabolic | Metabolic acidosis; hypocalcemia (early - Ca²⁺ sequestered in damaged muscle); hypercalcemia (late - release from necrotic muscle); hyperkalemia; hyperphosphatemia; hyperuricemia |
| Hematologic | DIC (thromboplastin release); elevated D-dimers, prolonged PT/aPTT; thrombocytopenia |
| Respiratory | ARDS (acute respiratory distress syndrome) - late complication |
| Neurological | Confusion, altered consciousness (due to metabolic derangements or hypoxia) |
| General | Fever, nausea, vomiting, malaise |
Classic Triad of Rhabdomyolysis
- Myalgia (muscle pain and tenderness)
- Generalized weakness
- Dark (reddish-brown) urine
Note: In practice, only a minority of patients present with all three. Many present with only one or two components, requiring a high index of suspicion.
Timeline of complications
| Phase | Time | Clinical events |
|---|---|---|
| Immediate | 0-6 h after extrication | Hypovolemic shock, hyperkalemia, cardiac arrhythmias, metabolic acidosis |
| Early delayed | 6-24 h | Oliguria, myoglobinuria, rising creatinine, compartment syndrome |
| Late | 1-7 days | Acute renal failure, ARDS, DIC, sepsis, ischemic organ injury |
| Delayed death | Days-weeks | Renal failure (primary), ARDS, sepsis, multi-organ failure |
Investigations
Bedside / Point-of-Care
- ECG: monitor for hyperkalemia changes (peaked T waves → widened QRS → sine wave → VF)
- Urinalysis (dipstick): positive for blood (myoglobin) but no RBCs on microscopy - this discrepancy is diagnostic
- Urine color: dark brown/tea-colored
- Compartment pressure measurement: Stryker device or saline manometer; >30 mmHg is diagnostic
Blood Tests
| Investigation | Expected Finding | Significance |
|---|---|---|
| Serum CK | >1000-5000 U/L (often >100,000 U/L) | Gold standard marker; 5x upper limit of normal indicates rhabdomyolysis; peaks at 2-3 days |
| Serum creatinine/BUN | Elevated | Renal impairment |
| Serum K+ | Elevated (hyperkalemia) | Life-threatening; may cause VF |
| Serum Ca²⁺ | Low (early), high (late) | Tetany, arrhythmias |
| Serum phosphate | Elevated | Contributes to AKI |
| Serum uric acid | Elevated | Tubular precipitation |
| ABG | Metabolic acidosis (low pH, low HCO3-) | Aggravates hyperkalemia toxicity |
| Blood glucose | Varies | Needed for hyperkalemia treatment |
| CBC | Anemia, thrombocytopenia (if DIC) | |
| Coagulation (PT/aPTT, D-dimer, fibrinogen) | Abnormal in DIC | |
| LDH, ALT, AST | Elevated (from muscle) | Note: AST/LDH are non-specific |
| Serum myoglobin | Elevated | Cleared rapidly; CK more reliable |
| Serum albumin | Low (hypoalbuminemia) | Volume loss, third-spacing |
Serum CK <20,000 U/L carries lower AKI risk. CK as low as 5000 U/L can cause AKI if sepsis, acidosis, or volume depletion co-exist. - Comprehensive Clinical Nephrology, 7th Ed.
Urine Tests
- Urine myoglobin: confirms rhabdomyolysis (though clears faster than CK)
- Urine microscopy: pigmented granular casts (characteristic), absence of RBCs
- Urine pH: aim >6.5 with alkalization therapy
- Urine electrolytes and creatinine: for clearance calculations
- 24-hour urine output: monitoring for oliguria/polyuria during recovery
Imaging
- X-ray: fractures, pneumothorax (associated injuries)
- Ultrasound: compartment assessment, deep vein thrombosis (DVT)
- CT/MRI: defines extent of muscle necrosis; MRI is most sensitive for muscle damage
- ECG: continuous monitoring mandatory
Laboratory Follow-up Protocol
Serial bloods every 2-4 hours monitoring: K+, Ca²+, PO4, pH, creatinine, CK, Hb, coagulation.
Treatment
The cornerstone of management is early, aggressive fluid resuscitation - ideally begun before extrication.
Pre-hospital / Field Management
- Begin IV fluid resuscitation before extrication if possible - this is the most effective intervention to prevent crush syndrome
- Use normal saline (0.9% NaCl) - avoid lactated Ringer's and other K+-containing fluids (risk of fatal hyperkalemia)
- Initial bolus: 1-2 L followed by 1000 mL/h, then reduce to 500 mL/h after 2 hours
- Continuous cardiac monitoring (ECG) - can be performed in confined spaces
- Immediate treatment of hyperkalemia: insulin + dextrose, calcium gluconate, beta-agonists, sodium bicarbonate, ion exchange resins
Fluid Resuscitation
- Target urine output: 200-300 mL/h (5-7 L/24 hours) for adults
- An average adult may require up to 12 L/day of fluids to sustain forced diuresis of 8 L/day
- Avoid fluid overload - monitor closely for pulmonary edema
- Urinary catheter placement is essential for monitoring
Alkaline Diuresis
- Once urine output is established: mannitol + sodium bicarbonate (alkaline diuresis)
- Maintain urine pH > 6.5 to prevent precipitation of myoglobin and uric acid in tubules
- Both myoglobin and uric acid are less nephrotoxic in alkaline urine
- Mannitol: osmotic diuretic, also reduces reperfusion injury component
- Target diuresis: up to 8 L/day
Management of Specific Complications
| Complication | Treatment |
|---|---|
| Hyperkalemia | Calcium gluconate (cardiac membrane stabilization); insulin + dextrose; sodium bicarbonate; beta-agonists; kayexalate; dialysis for refractory cases |
| Hypocalcemia | Calcium gluconate IV only if symptomatic (tetany, arrhythmias) - do not treat asymptomatic hypocalcemia as Ca²⁺ may precipitate in necrotic muscle |
| Metabolic acidosis | Sodium bicarbonate IV; also treats hyperkalemia |
| Renal failure | Renal replacement therapy (hemodialysis or CRRT - continuous renal replacement therapy) |
| DIC | FFP, cryoprecipitate, platelets as indicated |
| ARDS | Mechanical ventilation with lung-protective strategy |
Fasciotomy (for Compartment Syndrome)
Indications:
- Compartment pressure >30 mmHg (measured within 6 hours of injury)
- Delta pressure (diastolic BP - compartment pressure) <30 mmHg
- Absence of distal pulses
- Requirement for debridement of necrotic muscle
CRITICAL CAVEAT: Late fasciotomy (>12 hours post-entrapment, especially >12-24 hours) may cause massive myoglobin release from necrotic muscle, worsening renal failure. It also introduces infection risk into dead tissue. Most guidelines recommend against routine fasciotomy for late presentations of crush wounds, unless specific indications above are met. - Bailey & Love's Surgery, 28th Ed.
Hyperbaric Oxygen Therapy (HBO)
- Useful adjunct, particularly early post-injury
- At 2 atm: increases blood O2 content by 125%, increases tissue O2 tension 10-fold
- Reduces tissue edema via oxygen-induced vasoconstriction
- Long-term benefits: improved wound repair post-fasciotomy, reduced infection rates, better skin graft outcomes
- Does not replace fluid therapy
Dialysis
- Indications: refractory hyperkalemia, severe metabolic acidosis, fluid overload, oligoanuria with rising creatinine
- CRRT preferred in hemodynamically unstable patients
- Hemodialysis in stable patients
- Early dialysis (before overt uremia) may improve outcomes in disaster settings
Summary Treatment Algorithm
CRUSH INJURY IDENTIFIED
↓
Pre-extrication: IV NS 1-2L bolus → 1000 mL/h
ECG monitoring + treat hyperkalemia
↓
EXTRICATION
↓
Assess: Vitals, urine output, ECG, labs (CK, K+, Ca, pH, Cr)
Insert urinary catheter → target UO 200-300 mL/h
↓
UO established?
YES → Add Mannitol + NaHCO3 (alkaline diuresis)
Maintain urine pH > 6.5
NO → Increase fluid rate, reassess
↓
Compartment pressure >30 mmHg within 6 hrs? → Fasciotomy
↓
Renal failure? → Dialysis (HD or CRRT)
ARDS? → Mechanical ventilation
DIC? → FFP, platelets, cryoprecipitate
↓
ICU monitoring: serial labs q2-4h
K+, Ca, pH, Cr, CK, coagulation
Complications
| Complication | Mechanism | Comment |
|---|---|---|
| Acute kidney injury | Most serious; multifactorial | Primary cause of delayed death |
| Hyperkalemia | K+ release from myocytes | Can cause VF before any renal failure |
| Metabolic acidosis | Lactate + renal failure | Worsens K+ toxicity and arrhythmias |
| Cardiac arrhythmias | Hyperkalemia, acidosis | Including VF and cardiac arrest |
| Hypovolemic shock | Third-spacing + fluid sequestration in muscles | Can sequester many liters |
| DIC | Thromboplastin release | Dangerous in context of wounds/surgery |
| ARDS | Inflammatory mediator release | Late, severe complication |
| Sepsis | Open wounds, fasciotomy, ICU stay | Leading cause of late mortality |
| Compartment syndrome | Edema in closed fascial space | Local, but can worsen systemic disease |
| Fat embolism | Bone fractures or fat necrosis | Can cause respiratory failure |
| DVT/PE | Immobility, endothelial injury | Requires prophylaxis |
| Hypocalcemia (early) | Ca²⁺ sequestration in necrotic muscle | Tetany, arrhythmias |
| Hypercalcemia (late) | Ca²⁺ released from resolving necrosis | During recovery phase |
Prognosis
- With early, aggressive fluid resuscitation before extrication, many patients survive without dialysis
- Without treatment, mortality from AKI is high
- Recovery of renal function is possible in many survivors if supported through the acute phase
- Long-term sequelae include chronic neuropathic pain (from scar tissue stretching sensitized nerve endings) - managed by desensitization therapy
- In mass casualty settings, limited dialysis availability is a major determinant of mortality
Key Sources
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 10th Ed. - "Crush Injury and Crush Syndrome"
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - "Crush Injury and the Crush Syndrome"
- Bailey and Love's Short Practice of Surgery, 28th Ed. - "Crush Injury and Syndrome"
- Comprehensive Clinical Nephrology, 7th Ed. - "Rhabdomyolysis"
- Recent meta-analysis (2026): Rostami P et al. BMC Emergency Medicine - "Crush injury syndrome in earthquakes: a systematic review and meta-analysis on its frequency and complications." [PMID: 41928063]
This is a shared conversation. Sign in to Orris to start your own chat.