Yo
Hey! What's up? How can I help you today?
Accessible I get in this AI
Here's a quick rundown of what you can do with me:
What I Can Help With
Research & Knowledge
- Answer questions on virtually any topic - science, history, math, tech, etc.
- Medical/clinical questions (I have access to medical textbooks)
- Indian taxation (GST, income tax, CA exam prep)
Documents & Files
- Create Word docs (.docx), PowerPoint presentations (.pptx), Excel spreadsheets (.xlsx), PDFs
- Read and extract content from uploaded files
Search & Current Info
- Web search for up-to-date information
- Search PubMed for medical research papers
Images & Media
- Generate images from descriptions
- Analyze images or videos you upload
Code & Data
- Write and run code (Python, JavaScript, etc.)
- Data analysis and visualization
Just ask me anything or drop a file and I'll get to work. What do you need?
which book you use for medicine
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Here's the full library of medical textbooks I have access to, organized by specialty:
📚 Medical Textbook Library
Anatomy
- Gray's Anatomy for Students
- Netter's Atlas of Human Anatomy
- Color Atlas of Human Anatomy (Vol 1, 2, 3)
- General Anatomy and Musculoskeletal System (THIEME Atlas)
- Imaging Anatomy - Bones, Joints, Vessels and Nerves
- Color Atlas of Ultrasound Anatomy, 3e
Anesthesiology
- Miller's Anesthesia, 10e (2-Volume)
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
- Morgan and Mikhail's Clinical Anesthesiology, 7e
Biochemistry
- Harper's Illustrated Biochemistry, 32nd Ed
- Lippincott Illustrated Reviews: Biochemistry, 8e
- Basic Medical Biochemistry - A Clinical Approach, 6e
Cardiology
- Braunwald's Heart Disease (2-Volume)
- Fuster and Hurst's The Heart, 15th Ed
- Textbook of Clinical Echocardiography
Community Medicine
- Park's Textbook of Preventive and Social Medicine
Dermatology
- Fitzpatrick's Dermatology (Vol 1 & 2)
- Andrews' Diseases of the Skin, 2e
- Dermatology 2-Volume Set, 5e
Emergency Medicine
- Tintinalli's Emergency Medicine
- Rosen's Emergency Medicine
- Roberts and Hedges' Clinical Procedures in Emergency
ENT
- Cummings Otolaryngology Head and Neck Surgery
- Scott-Brown's Otorhinolaryngology (Vol 1 & 2)
- K.J. Lee's Essential Otolaryngology
- Shambaugh Surgery of the Ear
Family Medicine
- Textbook of Family Medicine, 9e
- Pfenninger and Fowler's Procedures for Primary Care
- Swanson's Family Medicine Review
Forensic Medicine
- Parikh's Textbook of Medical Jurisprudence
- DiMaio's Forensic Pathology, 3rd Ed
- P.C. Dikshit Textbook of Forensic Medicine
- The Essentials of Forensic Medicine and Toxicology, 36th Ed (2026)
- Forensic Anthropology - A Comprehensive Introduction
- Brogdon's Forensic Radiology
Gastroenterology
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Yamada's Textbook of Gastroenterology, 7e
- Clinical Gastrointestinal Endoscopy, 3e
- Maingot's Abdominal Operations
General Surgery
- Bailey and Love's Short Practice of Surgery, 28th Ed
- Schwartz's Principles of Surgery, 11th Ed
- Sabiston Textbook of Surgery
- Fischer's Mastery of Surgery, 8e
- S Das A Manual on Clinical Surgery, 13th Ed
- Current Surgical Therapy, 14e
- Mulholland and Greenfield's Surgery, 7e
- 22nd Edition Pye's Surgical Handicraft
Genetics
- Thompson & Thompson Genetics and Genomics in Medicine, 9e
- Emery's Elements of Medical Genetics and Genomics
Histology
- Junqueira's Basic Histology, 17e
- Histology: A Text and Atlas
Immunology
- Janeway's Immunobiology, 10e
- Cellular and Molecular Immunology
- Roitt's Essential Immunology
Internal Medicine
- Harrison's Principles of Internal Medicine, 22e (2025)
- Goldman-Cecil Medicine, 2-Volume Set
- Firestein & Kelley's Textbook of Rheumatology
- Rheumatology, 2-Volume Set (2022)
- The Washington Manual of Medical Therapeutics
- Frameworks for Internal Medicine
- Symptom to Diagnosis: An Evidence Based Guide, 4e
Laboratory Medicine
- Tietz Textbook of Laboratory Medicine, 7e
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Quick Compendium of Clinical Pathology, 5e
Microbiology
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28e
- Medical Microbiology, 9e
- Sherris & Ryan's Medical Microbiology, 8e
Nephrology
- Brenner and Rector's The Kidney (2-Volume)
- Comprehensive Clinical Nephrology, 7e
- National Kidney Foundation Primer on Kidney Diseases, 8e
Neurology
- Adams and Victor's Principles of Neurology, 12e
- Bradley and Daroff's Neurology in Clinical Practice
- Localization in Clinical Neurology, 8e
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Neuroscience
- Eric Kandel's Principles of Neural Science, 6e
- Neuroanatomy through Clinical Cases, 3e
- Neuroscience: Exploring the Brain, 5e
Obstetrics & Gynecology
- Berek & Novak's Gynecology
- Creasy & Resnik's Maternal-Fetal Medicine
Ophthalmology
- Kanski's Clinical Ophthalmology, 10e
- The Wills Eye Manual
Orthopedics
- Campbell's Operative Orthopaedics, 15th Ed (2026)
- Miller's Review of Orthopaedics, 9e
- Rockwood and Green's Fractures in Adults, 10th Ed (2025)
Pathology
- Robbins & Kumar Basic Pathology
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Pediatrics
- The Harriet Lane Handbook, 23e
- Red Book 2021 (Infectious Diseases)
Pharmacology
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Katzung's Basic and Clinical Pharmacology, 16e
- Lippincott Illustrated Reviews: Pharmacology
Physiology
- Guyton and Hall Textbook of Medical Physiology
- Ganong's Review of Medical Physiology, 26e
- Costanzo Physiology, 7e
- Medical Physiology
Psychiatry
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- Kaplan and Sadock's Synopsis of Psychiatry
- Stahl's Essential Psychopharmacology
- The Maudsley Prescribing Guidelines, 15e
- The Maudsley Deprescribing Guidelines
- The Clozapine Handbook
Pulmonology
- Murray & Nadel's Textbook of Respiratory Medicine (2-Volume)
- Fishman's Pulmonary Diseases and Disorders (2-Volume)
Radiology
- Grainger & Allison's Diagnostic Radiology
Urology
- Campbell Walsh Wein Urology (3-Volume)
- Hinman's Atlas of Urologic Surgery
- Smith and Tanagho's General Urology, 19e
That's 130+ textbooks across 30+ specialties! Ask me anything medical and I'll pull from these directly.
Rheumatic heart disease everything want for exam
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete exam-ready guide on Rheumatic Heart Disease, compiled from Robbins Pathology, Goldman-Cecil Medicine, Firestein & Kelley's Rheumatology, and Park's Preventive Medicine.
RHEUMATIC HEART DISEASE - Complete Exam Notes
1. DEFINITION
- Rheumatic Fever (RF): Acute, immunologically mediated, multisystem inflammatory disease occurring 2-3 weeks after Group A beta-hemolytic Streptococcal (GAS) pharyngitis
- Rheumatic Heart Disease (RHD): Chronic, progressive, deforming fibrotic valvular disease that results from repeated attacks of RF
- RF is not a communicable disease, but results FROM one (streptococcal pharyngitis)
- Robbins Pathologic Basis of Disease
2. EPIDEMIOLOGY
| Feature | Details |
|---|---|
| Age of RF | 5-15 years (children & adolescents) |
| Peak RHD prevalence | 3rd and 4th decades of life |
| Sex | RF: equal in both sexes; RHD: more common and more severe in females |
| India prevalence | 5-7 per 1,000 in 5-15 year age group; ~1 million RHD cases |
| India hospital burden | RHD = 20-30% of all CVD hospital admissions |
| Worldwide | >15 million cases; 282,000 new cases/year |
| Risk of RF after GAS pharyngitis | 0.3% to 3% |
- Risk factors: Poverty, overcrowding, poor housing, malnutrition, inadequate healthcare
- High-risk groups: School-age children (5-15 yrs), slum dwellers, people in closed communities (barracks)
- Park's Preventive & Social Medicine; Goldman-Cecil Medicine
3. PATHOGENESIS (MOLECULAR MIMICRY)
The key mechanism is molecular mimicry - immune cross-reactivity between streptococcal antigens and host cardiac tissue:
- GAS pharyngitis occurs
- 2-3 week delay (time to generate immune response)
- Antibodies and CD4+ T cells directed against streptococcal M proteins cross-react with cardiac antigens
- Anti-streptococcal antibodies also recognize N-acetyl-glucosamine (streptococcal carbohydrate) AND cardiac myosin, tropomyosin, laminin
- Antibodies bind valvular endothelium → upregulate VCAM-1 → facilitate CD4+ T cell infiltration
- Macrophage activation within Aschoff bodies (cytokine-mediated)
- Streptococci are completely absent from lesions (purely immune mediated)
- Genetic susceptibility is required (not all GAS-infected people develop RF)
- Robbins Pathology; Firestein & Kelley's Rheumatology
4. PATHOLOGY / MORPHOLOGY
Acute RF - Aschoff Bodies (PATHOGNOMONIC)
- Focal inflammatory lesions found throughout the heart
- Composition: T lymphocytes + plasma cells + Anitschkow cells (macrophages)
- Anitschkow cells = plump activated macrophages with:
- Abundant cytoplasm
- Central round-to-ovoid nucleus
- Chromatin condenses into slender wavy ribbon = "caterpillar cells"
- When binucleate = Aschoff giant cells
Pancarditis (all 3 layers involved):
- Pericarditis: Friction rub
- Myocarditis: Aschoff bodies in myocardium; can cause cardiac dilation
- Endocarditis/Valvulitis: Most important clinically
- Fibrinoid necrosis within cusps/tendinous cords
- Small 1-2 mm vegetations (verrucae) along lines of closure
- MacCallum plaques: Subendocardial thickenings in left atrium (from regurgitant jets)
Chronic RHD - Cardinal Changes of Mitral Valve:
- Leaflet thickening
- Commissural fusion and shortening
- Thickening and fusion of tendinous cords (chordae tendineae)
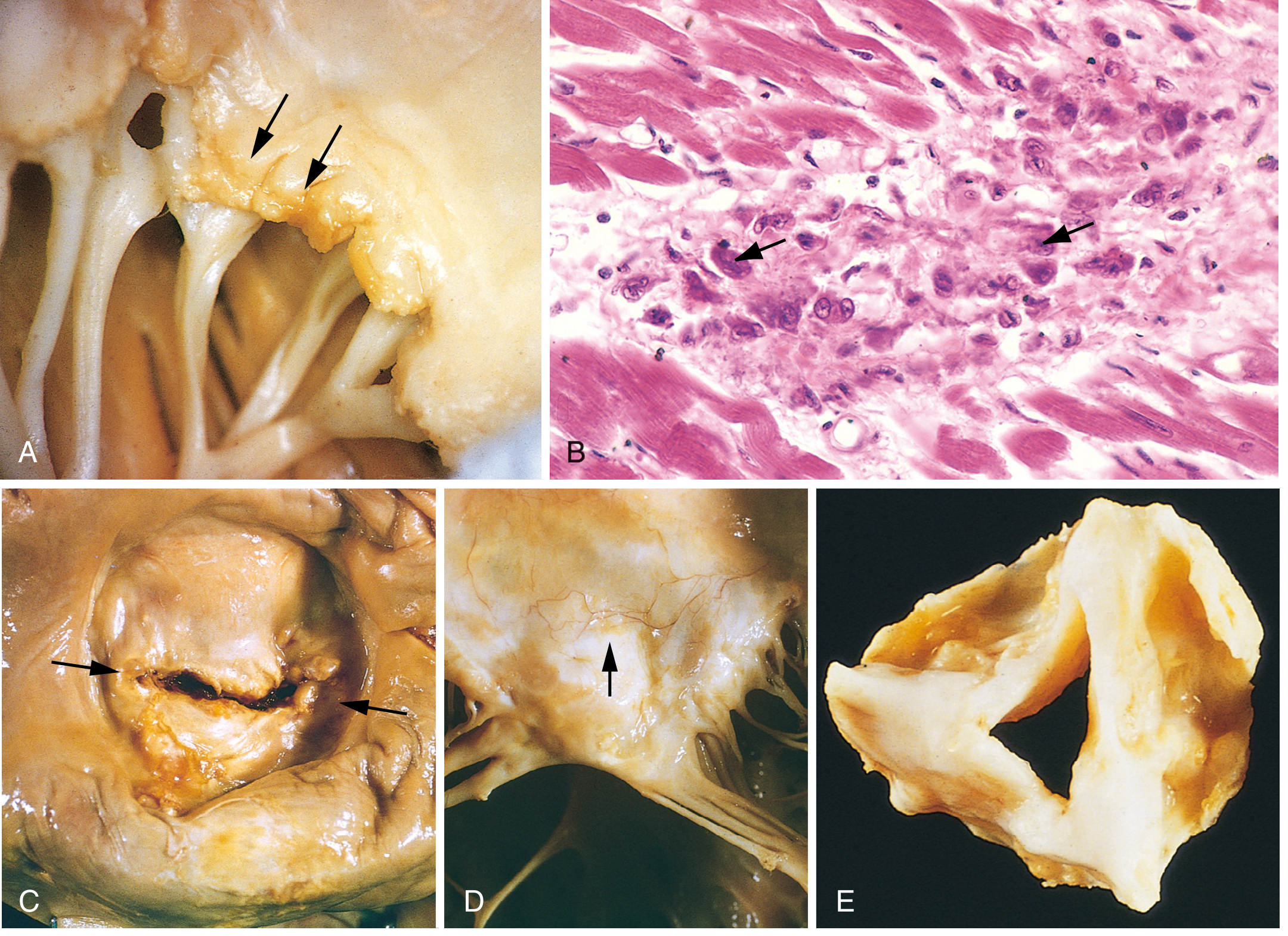
Fig. 12.22 from Robbins Pathologic Basis of Disease - Acute and chronic rheumatic heart disease
Valve Involvement (Frequency Order):
| Valve | Involvement |
|---|---|
| Mitral | Nearly 100%; isolated in ~2/3 of cases |
| Aortic | 20-30%; combined with mitral in ~25% |
| Tricuspid | Histologic disease in 15-40%; rarely clinically relevant |
| Pulmonary | Rarely affected |
- RHD is virtually the ONLY cause of mitral stenosis
- Most common valvular pathology in RHD = Mitral regurgitation (then progresses to stenosis)
- Aortic involvement: regurgitation more common than stenosis
- Robbins; Goldman-Cecil
5. CLINICAL FEATURES OF ACUTE RF
| Manifestation | Frequency | Notes |
|---|---|---|
| Fever | >90% | Lasts ~12 weeks, tendency to recur |
| Polyarthritis | 75-90% | MOST common; large joints (knees, ankles, elbows, wrists); migratory; NO residual damage; sterile synovial fluid |
| Carditis | 60-70% | Pancarditis; first-degree AV block (most common ECG finding) |
| Sydenham Chorea | 30% | "St. Vitus dance"; involuntary, non-rhythmic purposeless movements; worse on one side; stops during sleep; no residual damage |
| Subcutaneous nodules | <10% | Small (0.5-2 cm), painless, over bony prominences/extensor tendons; appear ~4 weeks after onset |
| Erythema marginatum | <10% | Pink, non-pruritic, blanching macules/papules; serpiginous pattern; trunk and proximal limbs |
- Symptoms begin ~2 weeks after streptococcal pharyngitis
- Disease usually persists 2-4 weeks
- Only carditis causes permanent damage - all other manifestations resolve without residual injury
6. REVISED JONES CRITERIA (2015 AHA) - DIAGNOSIS
Diagnostic Rule:
- Initial ARF: 2 major OR 1 major + 2 minor criteria
- Recurrent ARF: 2 major, OR 1 major + 2 minor, OR 3 minor criteria
- PLUS evidence of preceding GAS infection (positive culture/rapid test, OR elevated ASO/anti-DNase B)
Major Criteria:
| Low-Risk Populations | Moderate/High-Risk Populations |
|---|---|
| Carditis (clinical and/or subclinical echocardiographic valvulitis) | Same |
| Arthritis - polyarticular only | Arthritis - mono OR polyarticular |
| Chorea | Chorea |
| Erythema marginatum | Erythema marginatum |
| Subcutaneous nodules | Subcutaneous nodules |
Minor Criteria:
| Low-Risk | Moderate/High-Risk |
|---|---|
| Polyarthralgia | Monoarthralgia |
| Fever ≥38.5°C | Fever ≥38.5°C |
| ESR ≥60 mm/hr AND/OR CRP ≥3.0 mg/dL | ESR ≥30 mm/hr AND/OR CRP ≥3.0 mg/dL |
| Prolonged PR interval | Prolonged PR interval |
- Low-risk = ARF incidence <2 per 100,000 school-aged children/year OR all-age RHD prevalence ≤1 per 1,000/year
- India = moderate/high risk population
- Prolonged PR interval counts as minor criterion ONLY if carditis is NOT already a major criterion
- Goldman-Cecil; Firestein & Kelley
Special Diagnostic Situations (WHO 2002-03):
- Chorea alone = can diagnose RF (no other criteria needed)
- Insidious onset rheumatic carditis = can diagnose without other criteria
- Recurrent RF in established RHD = 3 minor criteria sufficient
7. LABORATORY FINDINGS
- Elevated inflammatory markers: ESR, CRP, leukocytosis
- Normochromic, normocytic anemia
- Throat culture: Usually negative by the time RF presents
- ASO (Anti-Streptolysin O) titer: Elevated (evidence of preceding GAS)
- Anti-DNase B: More sensitive, especially for skin infections
- ECG: Prolonged PR interval (1st degree AV block most common)
- Echocardiogram: Detects subclinical valvulitis; should be done in all suspected cases
8. CLINICAL FEATURES OF CHRONIC RHD
Appear years to decades after initial RF:
- Cardiac murmurs
- Cardiac hypertrophy and dilation
- Heart failure
- Atrial fibrillation (especially with mitral stenosis)
- Thromboembolic complications (stroke)
- Infective endocarditis (RHD is a major predisposing factor)
- Premature death - usually by age 35 or earlier
9. TREATMENT
Acute RF:
| Treatment | Details |
|---|---|
| Hospitalization | All patients with acute RF |
| Eradication of GAS | IM Benzathine Penicillin G 1.2 million units (single dose) |
| Arthritis | Aspirin 80-100 mg/kg/day (max 4-8 g/day) OR Naproxen 10-20 mg/kg/day |
| NSAID duration | 1-2 weeks until all symptoms resolve |
| Carditis/Heart failure | Diuretics, ARBs, fluid restriction, bed rest; glucocorticoids in severe cases |
| Chorea | Usually self-limiting; resolves in weeks to months |
| Valve surgery | Rarely for acute RF; helpful if acute valve leaflet rupture |
10. SECONDARY PROPHYLAXIS (KEY EXAM TOPIC)
Drug of Choice: Benzathine Penicillin G (BPG) - IM
| Weight | Dose |
|---|---|
| >27 kg (>60 lbs) | 1.2 million units IM |
| <27 kg (<60 lbs) | 600,000 units IM |
- Frequency: Every 4 weeks (monthly); every 3 weeks for high-risk patients
- IM BPG is MORE EFFECTIVE than oral penicillin
Alternative Regimens:
- Oral Penicillin V: 250 mg twice daily
- Penicillin allergy: Oral erythromycin 40 mg/kg/day (children) or 400 mg BD (adults)
- Azithromycin: 250 mg daily
Duration of Prophylaxis (WHO Recommendations):
| Category | Duration |
|---|---|
| RF without carditis | At least 5 years OR until age 18, whichever is longer |
| RF with mild carditis (mild MR or healed carditis) | 10 years after last attack OR until age 25, whichever is longer |
| Severe valvular disease / post-valve surgery | Life-long |
- Goldman-Cecil; Firestein & Kelley; Park's PSM
11. PRIMARY PREVENTION
- Prompt diagnosis and treatment of streptococcal pharyngitis with penicillin
- Reduces risk of RF by preventing initial attack
- Improving socioeconomic conditions (housing, crowding, nutrition)
12. RHD CONTROL PROGRAMME (Community Medicine - Park's)
Three levels of prevention:
- Primary: Treat GAS pharyngitis promptly; improve living conditions
- Secondary: Long-term BPG prophylaxis in known RF/RHD patients
- Non-medical: Improve housing, break poverty-disease cycle
Evaluation of Programme:
- Prevalence of RHD in school children (6-14 yr age group) from periodic surveys
- Survey every 5 years
- Recommended sample size: 20,000 to 30,000 children
13. COMPLICATIONS OF RHD
- Progressive valvular disease (mitral stenosis, MR, AR)
- Heart failure
- Atrial fibrillation
- Infective endocarditis
- Systemic embolism / stroke
- Pulmonary hypertension
- Pregnancy complications (high-risk cardiac condition)
14. QUICK MNEMONICS
Major Criteria - "JONES":
- J - Joints (polyarthritis)
- O - Oh heart (carditis)
- N - Nodules (subcutaneous)
- E - Erythema marginatum
- S - Sydenham chorea
Minor Criteria - "FESP":
- F - Fever ≥38.5°C
- E - Elevated ESR/CRP
- S - (Poly/mono)arthralgia
- P - Prolonged PR interval
15. HIGH-YIELD EXAM FACTS
| Fact | Answer |
|---|---|
| Most common cause of mitral stenosis worldwide | RHD |
| Most common valve affected in RHD | Mitral (nearly 100%) |
| Most common valvular pathology in RHD | Mitral regurgitation |
| Pathognomonic lesion of RF | Aschoff body |
| Cell in Aschoff body | Anitschkow cell (caterpillar cell) |
| Mechanism of RF | Molecular mimicry |
| Most common clinical feature | Polyarthritis (75-90%) |
| Only permanent damage in RF | Carditis |
| Most common ECG finding | Prolonged PR interval (1st degree AV block) |
| Drug of choice prophylaxis | Benzathine Penicillin G |
| Most effective route | IM (better than oral) |
| Chorea stops during | Sleep |
| Verrucae size | 1-2 mm |
| MacCallum plaques location | Left atrium |
| Juvenile mitral stenosis | Seen in India - early, severe, with PAH |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine; Firestein & Kelley's Textbook of Rheumatology; Park's Textbook of Preventive and Social Medicine
This is a shared conversation. Sign in to Orris to start your own chat.