Nephrotic vs nephratic syndrome
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have rich content from multiple authoritative sources. Let me compile the full answer.
Nephrotic vs. Nephritic Syndrome
Core Concept
Both are glomerular syndromes, but they differ fundamentally in the nature of the injury:
- Nephrotic: the filtration barrier becomes abnormally permeable to protein - so you lose protein into the urine, but red cells don't escape
- Nephritic: inflammatory injury disrupts the capillary wall, causing bleeding into the urine and impairing GFR
Side-by-Side Comparison
| Feature | Nephrotic | Nephritic |
|---|---|---|
| Core defect | Increased permeability to protein | Glomerular inflammation + capillary wall disruption |
| Proteinuria | Massive: ≥3.5 g/day (frank nephrotic range) | Mild-moderate (subnephrotic) |
| Hematuria | Absent or microscopic | Present - dysmorphic RBCs, RBC casts |
| Albumin | Low (<3 g/dL) | Normal or mildly reduced |
| Edema | Prominent, often periorbital, pitting | Mild to moderate |
| Hypertension | Variable | Prominent |
| Lipids | Hyperlipidemia + lipiduria | Normal |
| GFR / Azotemia | Usually preserved (except MCD) | Reduced - oliguria, azotemia |
| Complement | Normal (most causes) | Often low (e.g., post-strep, MPGN, lupus) |
| Urine sediment | "Bland" - fatty casts, oval fat bodies, lipiduria | Active - RBC casts, granular casts |
Nephrotic Syndrome in Depth
Pathophysiology
The glomerular capillary wall (endothelium + GBM + podocytes) serves as a size-and-charge barrier. When it is structurally or physicochemically disrupted, plasma proteins escape into the filtrate. Massive proteinuria depletes serum albumin faster than the liver can compensate, causing hypoalbuminemia. Low oncotic pressure drives fluid into the interstitium (underfill edema). Primary sodium retention by the distal nephron also contributes (overfill edema - common in non-MCD causes).
Hyperlipidemia arises because:
- Low oncotic pressure triggers hepatic lipoprotein synthesis
- Reduced lipoprotein lipase activity impairs clearance
Additional consequences include hypercoagulability (loss of antithrombin III, proteins C and S), and increased susceptibility to infection (loss of immunoglobulins + complement).
Clinical Features
- Proteinuria ≥3.5 g/day (>40 mg/m²/hour in children)
- Hypoalbuminemia <3 g/dL
- Generalized edema - periorbital (especially in the morning), dependent, can progress to ascites or pleural effusions
- Hyperlipidemia and lipiduria
- Hypercoagulable state (renal vein thrombosis risk)
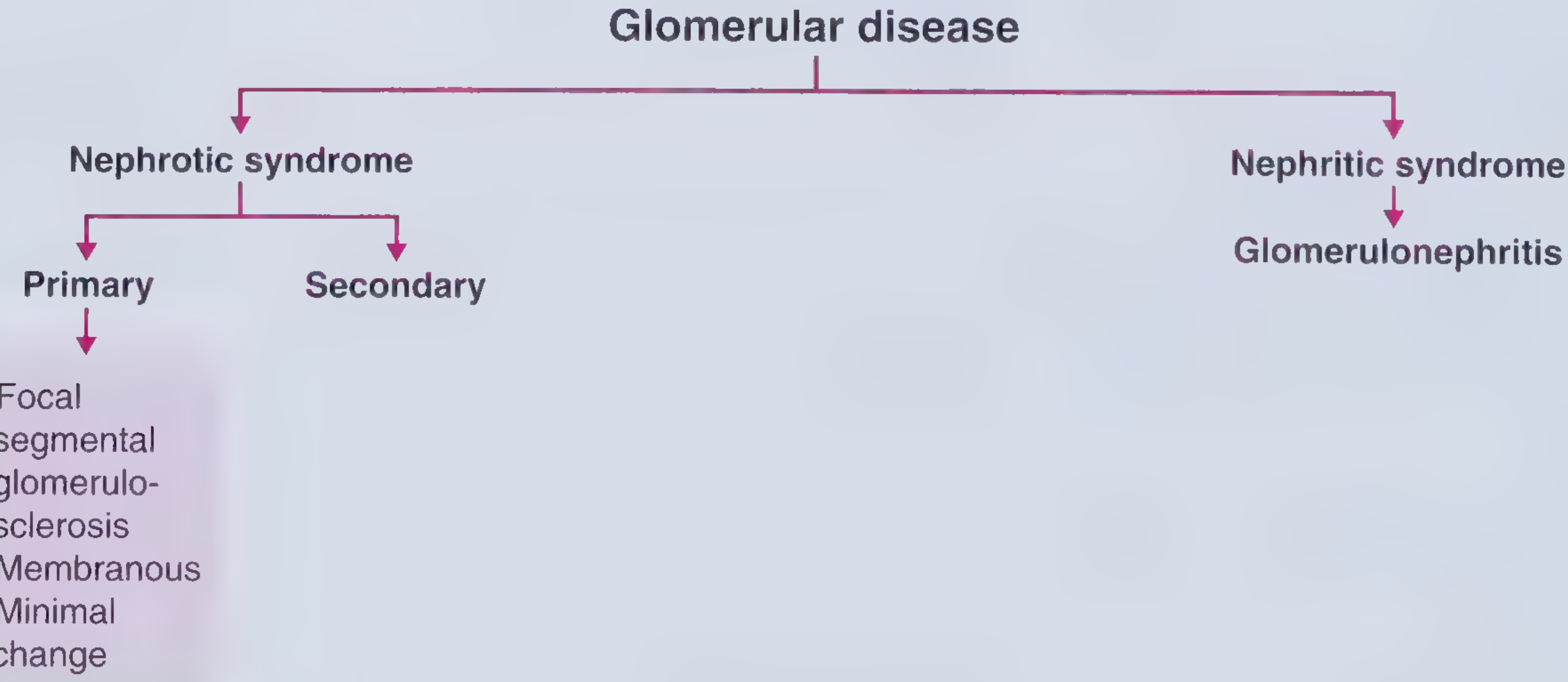
Primary Causes (in decreasing prevalence in adults)
- Focal Segmental Glomerulosclerosis (FSGS) - most common in adults, especially African Americans; podocyte injury; associated with HIV, obesity, sickle cell, reflux nephropathy
- Membranous Nephropathy - immune complex deposition on subepithelial surface; associated with anti-PLA2R antibodies; secondary causes include HBV, SLE, malignancy
- Minimal Change Disease (MCD) - most common in children (>90% of childhood nephrotic); effacement of podocyte foot processes on EM; normal on LM; responds to steroids
- Membranoproliferative GN (MPGN) - can be nephrotic or nephritic
Secondary Causes
- Diabetic nephropathy (most common secondary cause worldwide)
- Amyloidosis
- Membranous lupus nephritis (class V)
- Preeclampsia
Nephritic Syndrome in Depth
Pathophysiology
Inflammatory injury to the glomerular capillaries (proliferative GN) causes:
- Hematuria - capillary wall damage lets RBCs escape into the Bowman space; dysmorphic RBCs and RBC casts form in the tubules
- Reduced GFR - inflammation reduces filtration surface area, causing oliguria, fluid retention, and azotemia
- Hypertension - from fluid retention and renin release from ischemic kidneys
- Mild proteinuria - some protein leaks through damaged walls, but not as severely as nephrotic
Clinical Features
- Hematuria - "cola-colored" or "smoky" urine; dysmorphic RBCs + RBC casts on urine microscopy
- Oliguria and azotemia
- Hypertension
- Mild proteinuria (usually <3.5 g/day)
- Edema (milder)
Major Causes
| Disease | Key Clue |
|---|---|
| Postinfectious GN (post-strep) | 1-4 weeks after strep pharyngitis or impetigo; low C3; subepithelial "humps" on EM; children 6-10 yr |
| IgA Nephropathy (Berger) | Gross hematuria during/after URI (synpharyngitic - within 1-2 days); most common GN worldwide |
| Rapidly Progressive GN (RPGN/Crescentic GN) | Rapid renal function decline over days-weeks; crescents on biopsy; classified as anti-GBM (type I), immune complex (type II), or pauci-immune/ANCA (type III) |
| Anti-GBM (Goodpasture) | Linear IgG on IF; pulmonary hemorrhage + nephritis; anti-GBM antibodies |
| Lupus nephritis (class III/IV) | Low C3/C4, ANA, anti-dsDNA positive |
| ANCA-associated vasculitis | GPA, MPA, EGPA; pauci-immune (no immune deposits); p-ANCA or c-ANCA positive |
| MPGN | Hypocomplementemia; "tram-track" on LM |
Key Mnemonic
NephrOtic = Oil (lipids), Oedema, Only protein in urine
NephrItic = Inflammation, Injury, Iron (blood/hematuria)
NephrItic = Inflammation, Injury, Iron (blood/hematuria)
Or remember the "PHAROH" features of nephrotic:
Proteinuria, Hypoalbuminemia, Anasarca/edema, Hyperlipidemia, Oval fat bodies/lipiduria, Hypercoagulability
When They Overlap
Some diseases can present with features of both ("nephrotic-nephritic overlap"):
- Membranoproliferative GN
- Diffuse proliferative lupus nephritis (class IV)
- FSGS (occasionally with hematuria)
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine; Brenner and Rector's The Kidney; Comprehensive Clinical Nephrology 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.