Cell adhesion molecules
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have excellent content from multiple textbooks and the key diagram. Let me compile a comprehensive answer.
Cell Adhesion Molecules (CAMs)
Cell adhesion molecules are transmembrane glycoproteins that mediate attachment between cells (cell-cell) and between cells and the extracellular matrix (cell-ECM). They are indispensable for embryogenesis, immune surveillance, wound healing, hemostasis, and tissue integrity - and their dysregulation drives cancer metastasis, autoimmunity, and vascular thrombosis.
Classification: Five Major Families
CAMs are grouped into five families based on structural homology:
| Family | Ca²⁺ dependency | Primary function | Key ligands |
|---|---|---|---|
| Cadherins | Ca²⁺-dependent | Cell-cell adhesion (homophilic) | Other cadherins |
| Integrins | Divalent cations | Cell-ECM and cell-cell | Fibronectin, collagen, laminin, ICAMs |
| Selectins | Ca²⁺-dependent | Leukocyte rolling (lectin-type) | Sialyl-Lewis X carbohydrates |
| Immunoglobulin superfamily (IgSF) | Ca²⁺-independent | Firm adhesion, diapedesis | Integrins, other IgSF members |
| Mucins | - | Selectin ligand scaffolds | Selectins |
(Henry's Clinical Diagnosis and Management by Laboratory Methods)
1. Cadherins
Cadherins are Ca²⁺-dependent glycoproteins that mediate homophilic (like-to-like) cell-cell bonding. They contain:
- A large extracellular domain with three repeated domains that bind Ca²⁺
- A single transmembrane segment
- A cytoplasmic tail that binds a complex of catenins (α, β, γ), which anchor to the actin cytoskeleton at the zona adherens
Three main subtypes:
- E-cadherin - epithelial cells; loss is a hallmark of epithelial-to-mesenchymal transition in cancer
- N-cadherin - neural tissues and muscle
- P-cadherin - placenta and epithelium
Cadherins serve as important components of desmosomes and adherens junctions. Loss of E-cadherin correlates strongly with invasive and metastatic tumor behavior.
(Campbell-Walsh-Wein Urology; Medical Physiology)
2. Integrins
Integrins are heterodimers of non-covalently linked α and β subunits, bridging the ECM with the intracellular cytoskeleton.
- ~18 α and 8 β subunits combine to form >24 distinct heterodimers
- External domain contacts fibronectin, fibrinogen, collagen, and laminin via the RGD tripeptide motif (Arg-Gly-Asp)
- Intracellular tail connects to focal adhesion complexes (talin, kindlin, vinculin)
Key subfamilies:
- β1 integrins (VLAs, CD29) - expressed on leukocytes, platelets, tumor cells; bind ECM components
- β2 integrins (CD18) - leukocytes and myeloid cells; αLβ2 = LFA-1 (CD11a/CD18) - the critical molecule for leukocyte adhesion to endothelium; binds ICAM-1
- β3 integrins - include αIIbβ3 (GPIIb/IIIa) on platelets - essential for platelet aggregation
Bidirectional signaling:
- Inside-out signaling: chemokine receptor activation → talin/kindlin bind β-tail → integrin shifts from bent (low-affinity) to extended (high-affinity) conformation
- Outside-in signaling: ligand binding → cytoskeletal reorganization and gene expression changes
(Henry's Clinical Diagnosis and Management by Laboratory Methods)
3. Selectins
The selectin family comprises three homologous lectin-type molecules (Ca²⁺-dependent, carbohydrate-binding) with shared extracellular architecture: lectin domain + EGF domain + consensus repeat (CR) domains.
| Selectin | CD | Expressed on | Ligands | Key role |
|---|---|---|---|---|
| L-selectin | CD62L | Most leukocytes (microvilli) | GlyCAM-1, MAdCAM-1, CD34 | Lymphocyte homing to HEVs, neutrophil rolling |
| E-selectin | CD62E | Activated endothelium | Sialyl-Lewis X (CLA) | Skin-homing T cells; effector/memory T cell recruitment |
| P-selectin | CD62P | Platelets (α-granules), endothelium (Weibel-Palade bodies) | PSGL-1, sialyl-Lewis X/A | First responder in inflammation; promotes coagulation |
Notably, "catch bonds" between selectins and their carbohydrate ligands are strengthened (not weakened) by blood flow shear forces.
(Henry's Clinical Diagnosis and Management by Laboratory Methods)
4. Immunoglobulin Superfamily (IgSF) CAMs
IgSF members share immunoglobulin-like domains and mediate Ca²⁺-independent adhesion. Key members include:
- ICAM-1 (CD54) - ligand for LFA-1 (β2 integrin) on endothelium; upregulated by TNF-α, IL-1 in inflammation
- ICAM-2 (CD102) - constitutively expressed on endothelium
- VCAM-1 (CD106) - ligand for α4β1 integrin (VLA-4) on lymphocytes and monocytes; upregulated in atherosclerosis
- MAdCAM-1 - gut-homing addressin, ligand for α4β7 integrin
- N-CAMs (neural cell adhesion molecules) - GPI-linked or transmembrane; mediate neural-neural adhesion during axon guidance and fasciculation
(Henry's Clinical Diagnosis and Management by Laboratory Methods; Medical Physiology)
5. The Leukocyte Adhesion Cascade
The classic multistep model describes how leukocytes exit the bloodstream at sites of inflammation:
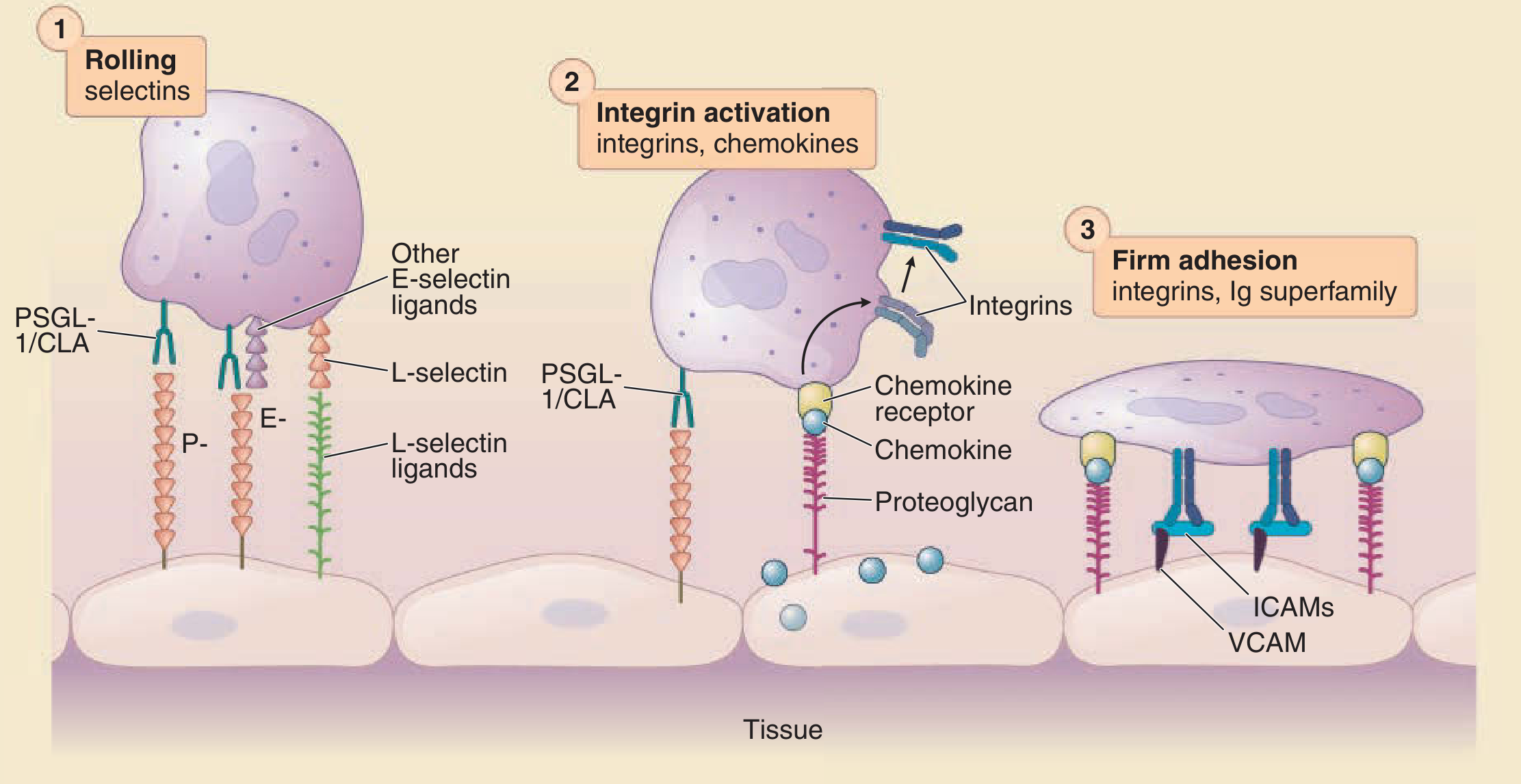
Step 1 - Rolling: Selectins (P-, E-, L-selectin) mediate transient tethering of leukocytes to activated endothelium via PSGL-1 and sialyl-Lewis X ligands. The leukocyte "rolls" along the vessel wall.
Step 2 - Activation: Chemokines (e.g., IL-8, CXCL12) secreted by endothelial cells bind proteoglycans and engage chemokine receptors on the rolling leukocyte. This triggers inside-out signaling → integrin activation (conformational change from bent → extended).
Step 3 - Firm adhesion: Activated β2 integrins (LFA-1, Mac-1) bind ICAM-1/ICAM-2 on endothelium; α4β1/α4β7 integrins bind VCAM-1/MAdCAM-1. The leukocyte arrests.
Step 4 - Transmigration (diapedesis): The leukocyte squeezes between endothelial cells, guided by PECAM-1 (CD31) and JAM proteins, into the tissue.
(Fitzpatrick's Dermatology; Henry's Clinical Diagnosis and Management by Laboratory Methods)
Clinical Significance
| Context | CAM involved | Mechanism |
|---|---|---|
| Leukocyte adhesion deficiency (LAD) | β2 integrin (CD18) mutation | Absent LFA-1/Mac-1 → failure of neutrophil extravasation → recurrent infections |
| Cancer metastasis | Loss of E-cadherin; altered integrins | Loss of tissue anchoring → invasion and hematogenous spread |
| Atherosclerosis | VCAM-1, ICAM-1 upregulation | Monocyte recruitment into subintimal space |
| Venous thromboembolism (DVT) | P-selectin (sP-sel ≥ 90 ng/mL) | Biomarker; sP-sel + Wells score improves DVT diagnosis (PPV 91%) |
| IBD / Multiple sclerosis | α4 integrins (α4β1, α4β7) | Targeted by natalizumab (anti-α4) and vedolizumab (anti-α4β7) |
| Platelet aggregation | αIIbβ3 (GPIIb/IIIa) | Blocked by abciximab, eptifibatide, tirofiban in ACS |
(Henry's Clinical Diagnosis and Management by Laboratory Methods; Mulholland & Greenfield's Surgery)
Key Points (Summary)
- CAMs are divided into cadherins, integrins, selectins, IgSF, and mucins
- Cadherins (Ca²⁺-dependent, homophilic) maintain epithelial integrity via catenin linkage to the cytoskeleton; their loss promotes cancer invasion
- Integrins (α/β heterodimers) mediate bidirectional signaling between ECM and cytoskeleton; activation is regulated by inside-out (chemokine-driven) conformational change
- Selectins mediate rolling via lectin-carbohydrate bonds strengthened by shear stress
- IgSF CAMs (ICAM-1, VCAM-1) mediate firm arrest of leukocytes and are upregulated by inflammatory cytokines
- The leukocyte adhesion cascade (rolling → activation → firm adhesion → diapedesis) is the molecular basis of all inflammatory cell trafficking and is a major pharmacologic target
Malignant breast carcinoma from WHO.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive answer. Let me compile it.
Malignant Breast Carcinoma - WHO Classification
The WHO Classification of Tumours (5th edition, Breast Tumours) recognizes breast cancer as a heterogeneous disease subclassified by histologic type, grade, and biomarker expression (ER, PR, HER2). The vast majority are adenocarcinomas.
Overview and Epidemiology
Breast cancer is the most common malignancy globally - in 2020 it surpassed lung cancer with an estimated 2.3 million new cases, accounting for ~12% of all new cancer diagnoses worldwide. The lifetime risk for a female is 1 in 8 (to age 90). Incidence continues rising in low-resource countries due to delayed childbearing, reduced breastfeeding, and late presentation.
Fundamental Classification Framework
Three complementary systems define breast cancer subtype:
| Approach | What it assesses | Output |
|---|---|---|
| Histologic type | Morphology / architecture | ~20 subtypes (see below) |
| Histologic grade | Differentiation (Nottingham Score) | Grade 1-3 |
| Biomarker profile | ER, PR, HER2 expression | 3 clinical groups |
| Molecular subtype | Gene expression profiling | 6 intrinsic subtypes |
Part I: Histologic Types
A. In Situ Carcinomas (Non-Invasive)
1. Ductal Carcinoma In Situ (DCIS)
- Malignant epithelial cells confined within ducts, without basement membrane breach
- Most often found on mammographic screening as calcifications
- A direct precursor to invasive ductal carcinoma (develops in the same breast)
- Classified by architecture: solid, cribriform, micropapillary, papillary, and comedo (the last with central necrosis)
2. Lobular Carcinoma In Situ (LCIS)
- Marker of increased risk AND a precursor lesion
- When invasive carcinoma subsequently develops: 2/3 in same breast, 1/3 contralateral
- Hallmark: loss of E-cadherin expression (CDH1 mutation)
B. Invasive (Malignant) Carcinomas
1. Invasive Carcinoma of No Special Type (NST) - formerly "Invasive Ductal Carcinoma NOS"
The most common invasive breast cancer, accounting for ~75% of all cases. This heterogeneous group is defined by exclusion - tumors that do not meet criteria for any special type.
Gross and imaging features:
- Hard, irregular, radiodense mass with spiculated margins on mammography
- Grating sound when cut due to desmoplastic stroma with chalky-white areas and calcifications
- Less commonly: well-circumscribed mass with scant stroma, or imperceptible scattered glands
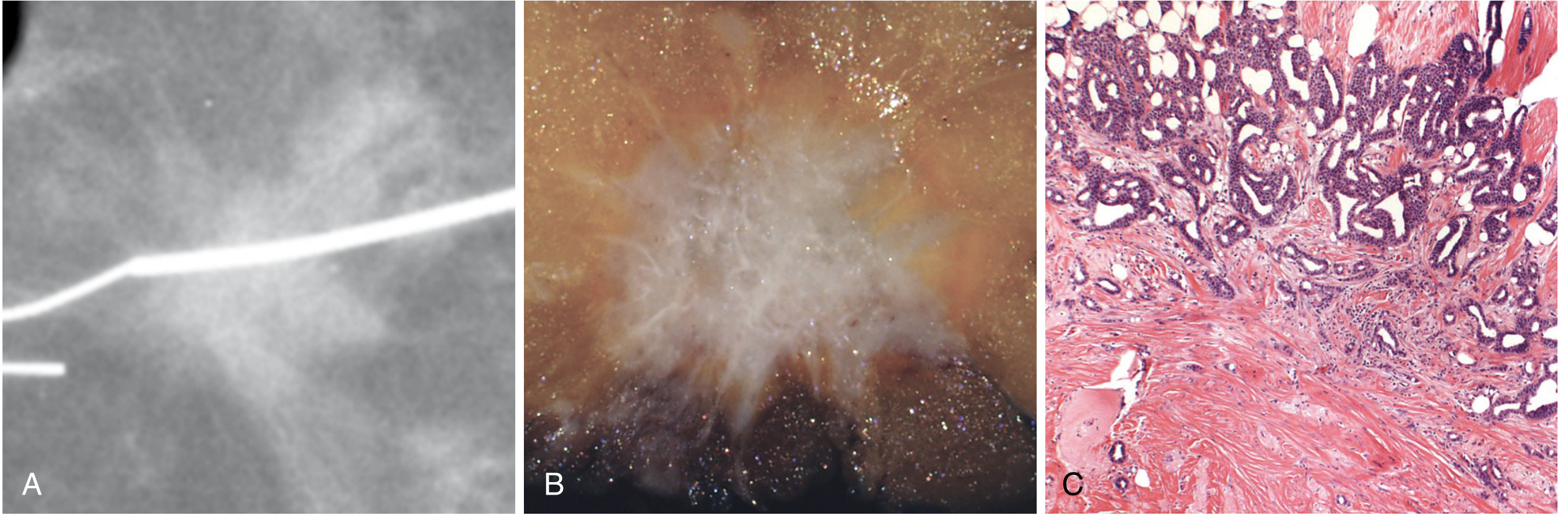
Fig. 23.20 - Invasive carcinoma of no special type showing spiculated mammographic appearance (A), gross stellate morphology (B), and desmoplastic stromal response microscopically (C)
Note on Medullary Carcinoma: High-grade NST tumors with prominent tumor-infiltrating lymphocytes (TILs) were formerly termed "medullary carcinoma" but this entity was removed from the WHO classification as it was not diagnostically reproducible. These are now classified as invasive carcinoma of no special type with "medullary pattern."
Histologic Grading (Nottingham Score - applies to all invasive carcinomas)
All invasive carcinomas are graded on three parameters:
| Parameter | Score 1 | Score 2 | Score 3 |
|---|---|---|---|
| Tubule formation | >75% | 10-75% | <10% |
| Nuclear pleomorphism | Small uniform | Moderate variation | Marked variation |
| Mitotic rate | Low | Intermediate | High |
- Grade 1 (3-5 pts) - Well differentiated: tubular/cribriform growth, small uniform nuclei, rare mitoses
- Grade 2 (6-7 pts) - Moderately differentiated: mixed solid nests and tubules, moderate pleomorphism
- Grade 3 (8-9 pts) - Poorly differentiated: ragged sheets, marked pleomorphism, tumor necrosis, frequent mitoses
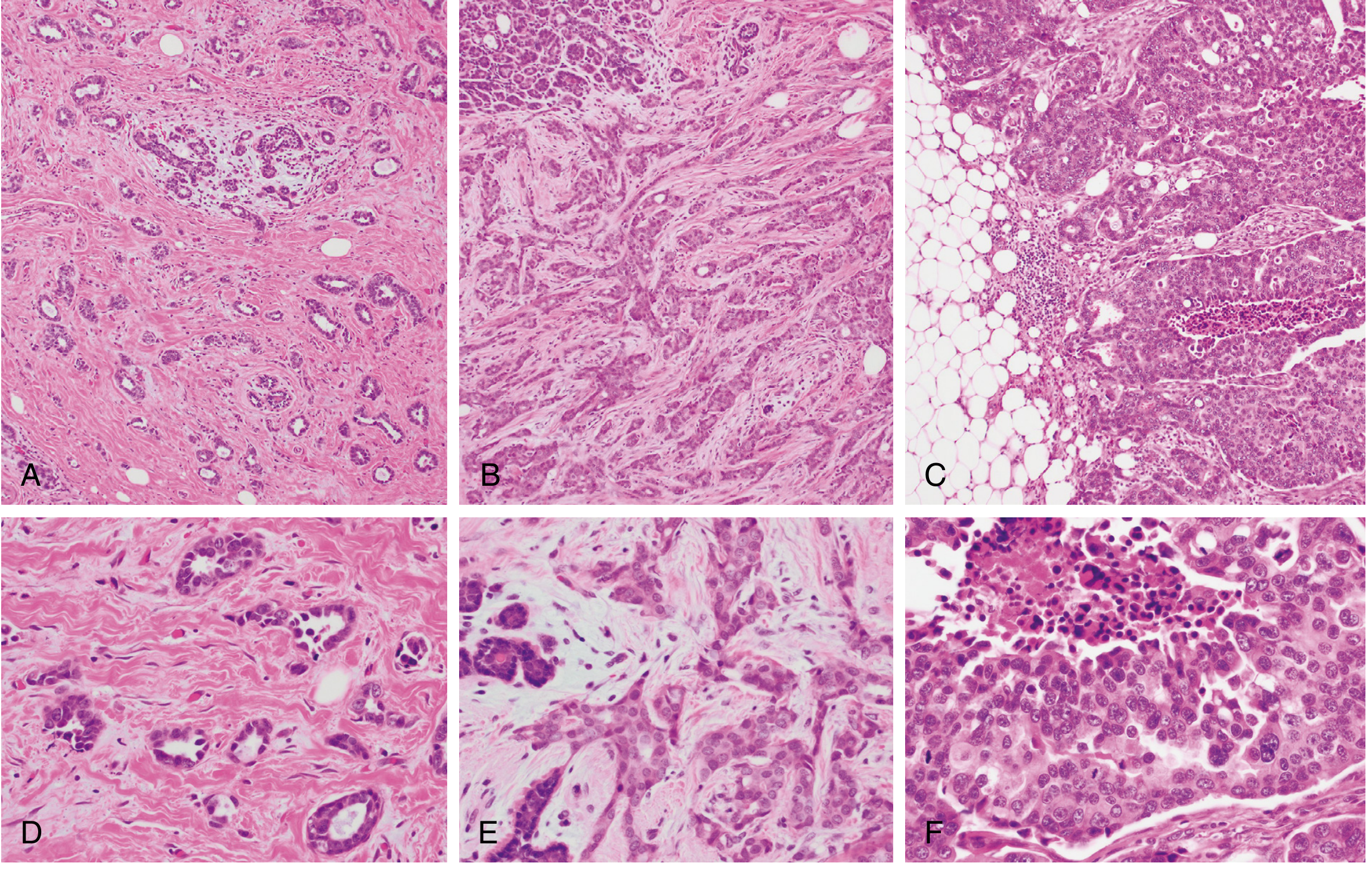
Fig. 23.21 - Histologic grading at low (A-C) and high (D-F) magnification.
2. Special Histologic Subtypes
These morphologically distinct subtypes harbor unique genetic signatures and differ in prognosis and behavior. They are organized by their biomarker profile:
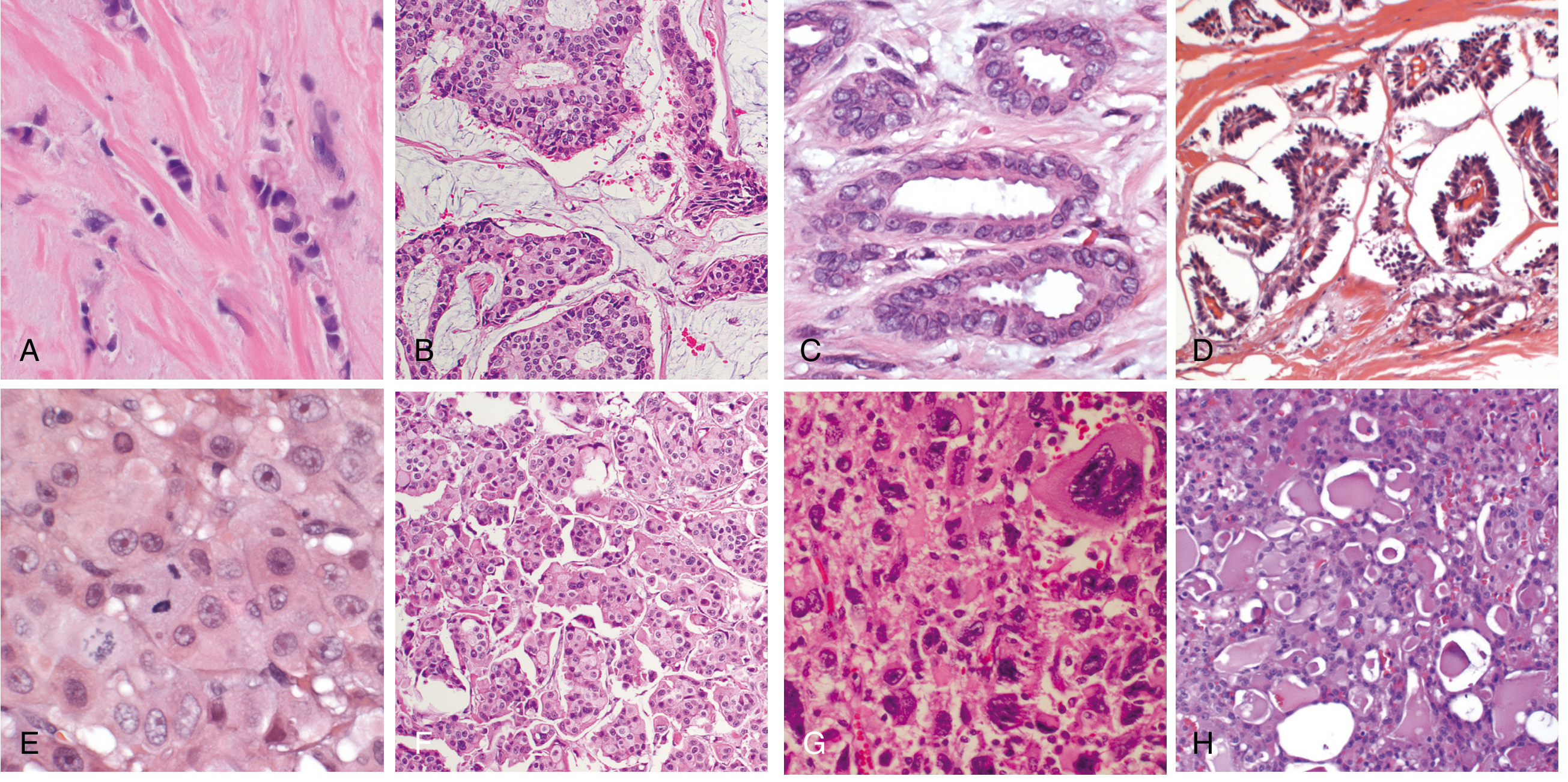
Fig. 23.22 - Special histologic subtypes of invasive carcinoma.
Usually ER-positive / HER2-negative (Luminal):
| Subtype | Key Features | Prognosis |
|---|---|---|
| Invasive Lobular Carcinoma | ~15% of cases; dyscohesive cells in single-file "Indian file" cords; signet ring cells; E-cadherin loss (CDH1); minimal desmoplasia; insidious spread | Favorable per grade |
| Mucinous (Colloid) Carcinoma | Soft/gelatinous mass; tumor cell clusters floating in large lakes of extracellular mucin | Favorable |
| Tubular Carcinoma | Exclusively well-formed open tubules; may mimic benign sclerosing lesion | Excellent |
| Cribriform Carcinoma | Invasive nests with cribriform (sieve-like) architecture | Favorable |
| Papillary Carcinoma | True papillary fronds with fibrovascular cores lined by tumor cells | Good |
More likely HER2-positive:
| Subtype | Key Features |
|---|---|
| Apocrine Carcinoma | Cells resemble sweat gland epithelium; enlarged round nuclei with prominent nucleoli; abundant eosinophilic granular cytoplasm |
| Invasive Micropapillary Carcinoma | Hollow balls of cells floating in intercellular fluid; mimic papillae but lack fibrovascular cores; high rate of lymph node metastasis |
Usually Triple Negative (ER/PR/HER2-negative):
| Subtype | Key Features | Prognosis |
|---|---|---|
| Metaplastic Carcinoma | Squamous or mesenchymal (spindle, chondroid, osseous) differentiation; myoepithelial gene expression; poor prognosis (except rare low-grade variants) | Poor |
| Adenoid Cystic Carcinoma | Identical to salivary gland counterpart; cribriform basaloid pattern | Favorable |
| Secretory Carcinoma | Abundant intracellular/extracellular secretions; identical to salivary gland type; often carries ETV6-NTRK3 fusion | Favorable |
| Mucoepidermoid Carcinoma | Salivary gland-like; rare | Variable |
3. Inflammatory Breast Carcinoma (IBC)
Not a distinct histologic type but a clinical presentation caused by extensive dermal lymphovascular invasion:
- Diffuse breast erythema, swelling, skin thickening
- Classic peau d'orange appearance (skin dimpling from tethered Cooper ligaments)
- No discrete palpable mass; high-grade and diffusely infiltrative
- Often misdiagnosed as cellulitis - "inflammatory" is a misnomer (no true inflammation)
- Accounts for 1-5% of cases; particularly poor prognosis
Part II: Molecular (Biomarker) Classification
3 Clinical Groups (ER, PR, HER2 testing)
| Group | Biomarkers | Characteristics |
|---|---|---|
| Luminal | ER+/HER2- | Most common; older women; lower grade; best prognosis |
| HER2 | HER2+ (any ER/PR) | More aggressive; responds to HER2-targeted therapy (trastuzumab) |
| TNBC | ER-/PR-/HER2- | Younger women; high grade; basal-like; no targeted therapy; worst prognosis |
6 Intrinsic Molecular Subtypes (Gene Expression Profiling)
| Subtype | Correlates with | Key features |
|---|---|---|
| Luminal A | ER+/PR+/HER2-, low Ki-67 | Low grade, best prognosis |
| Luminal B | ER+, HER2- or HER2+, higher Ki-67 | Higher proliferation, worse than Luminal A |
| HER2-enriched | HER2+ / ER- | Aggressive; responds to anti-HER2 therapy |
| Basal-like | ER-/PR-/HER2- | Overlaps with TNBC; BRCA1 associated; high grade |
| Claudin-low | ER-/PR-/HER2- | Stem cell-like; immune infiltration |
| Normal-like | ER+/HER2- | Resembles normal breast tissue |
Part III: Prognostic and Predictive Factors
Primary Prognostic Factors (AJCC 8th Edition Staging)
| Factor | Significance |
|---|---|
| Distant metastases (M stage) | Most important - present in 5% at diagnosis; cure unlikely |
| Lymph node status | Number of positive nodes, extra-nodal extension |
| Tumor size (T stage) | Larger tumors = worse prognosis |
| Histologic grade | Grade 3 = higher risk of relapse and death |
| ER/PR status | ER+ = better prognosis; predicts response to endocrine therapy |
| HER2 status | Predictive of response to trastuzumab/pertuzumab |
| Ki-67 / proliferation index | Higher = more aggressive |
| Tumor-infiltrating lymphocytes (TILs) | High TILs (especially in TNBC) = better prognosis |
Genetic Predisposition
- ~12% of breast cancers are caused by germline mutations
- BRCA1 / BRCA2 account for 50% of hereditary cases
- CDH1 germline mutations: risk of lobular breast carcinoma + gastric signet ring carcinoma
Metastatic Patterns by Subtype
- Luminal/ER+ - bone is the most common first site; late recurrences (>10 years)
- HER2+ - brain, lung, liver
- TNBC / basal-like - visceral and CNS; early recurrences
- Lobular carcinoma - peritoneum, retroperitoneum, leptomeninges, GI tract, ovaries, uterus
WHO Classification Summary Table
| Category | Subtype | ~Frequency | Grade | Biomarker |
|---|---|---|---|---|
| In situ | DCIS | Common | - | Variable |
| In situ | LCIS | Less common | - | Usually ER+ |
| Invasive NST | Carcinoma of no special type | ~75% | 1-3 | All groups |
| Special type | Invasive lobular carcinoma | ~15% | Usually low | Luminal |
| Special type | Mucinous carcinoma | Rare | Usually low | Luminal |
| Special type | Tubular carcinoma | Rare | 1 | Luminal |
| Special type | Cribriform carcinoma | Rare | 1 | Luminal |
| Special type | Papillary carcinoma | Rare | Variable | Luminal |
| Special type | Apocrine carcinoma | Rare | 2-3 | AR+/HER2+ |
| Special type | Micropapillary carcinoma | Rare | 2-3 | HER2+ |
| Special type | Metaplastic carcinoma | Rare | 3 | TNBC |
| Special type | Adenoid cystic / secretory | Very rare | Low | TNBC, good Px |
| Clinical | Inflammatory breast carcinoma | 1-5% | Usually 3 | Usually TNBC/HER2 |
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (p. 978-985); Robbins & Kumar Basic Pathology (p. 719)
This is a shared conversation. Sign in to Orris to start your own chat.