Absent nasal bone in fetus
Reading File
Finding Sources
Searching PubMed
"nasal bone" AND fetus AND "Down syndrome"
Reading File
Reading File
Searching PubMed
"nasal bone" AND prenatal AND trisomy
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough, textbook-based summary of absent nasal bone in the fetus.
Absent Nasal Bone in the Fetus
Background / Pathophysiology
Absent nasal bone (NB) on prenatal ultrasound reflects delayed or absent ossification of the fetal nasal bone. The flat nasal bridge is a well-recognized feature of Down syndrome (trisomy 21), and histopathologic studies confirm that NB ossification is absent in about one-quarter of Down syndrome fetuses evaluated between 15-40 weeks' gestation (Stempfle et al.), and absent in one-third by radiographic-pathologic analysis (Tuxen et al.). - Creasy & Resnik's Maternal-Fetal Medicine, p. 649
When and How It Is Assessed
First Trimester (11-13+6 weeks)
Assessment is done in the midsagittal plane with the transducer at ~45 degrees to the profile.
Technical criteria (Fetal Medicine Foundation):
- Image magnified so each caliper movement = 0.1 mm change
- Midsagittal view of fetal profile (tip of nose, 3rd/4th ventricles visible; orbit and zygoma NOT seen)
- Transducer parallel to the direction of the nose, tilted side-to-side to confirm NB is separate from overlying skin
How to call "absent":
When a normal NB is present, three echogenic lines are visible - the NB and overlying skin form an "equal sign" (=). The NB echogenicity is greater than (or at least equal to) the overlying skin. If the NB echo is less echogenic than the skin edge and thinner than the overlying skin, it is not yet ossified and is classified as absent.
Note: The echogenic skin edge can be mistaken for the nasal bone. Careful tilting technique is essential.
It takes an average of 80 studies for a clinician to become proficient in NB assessment.
Ultrasound Images
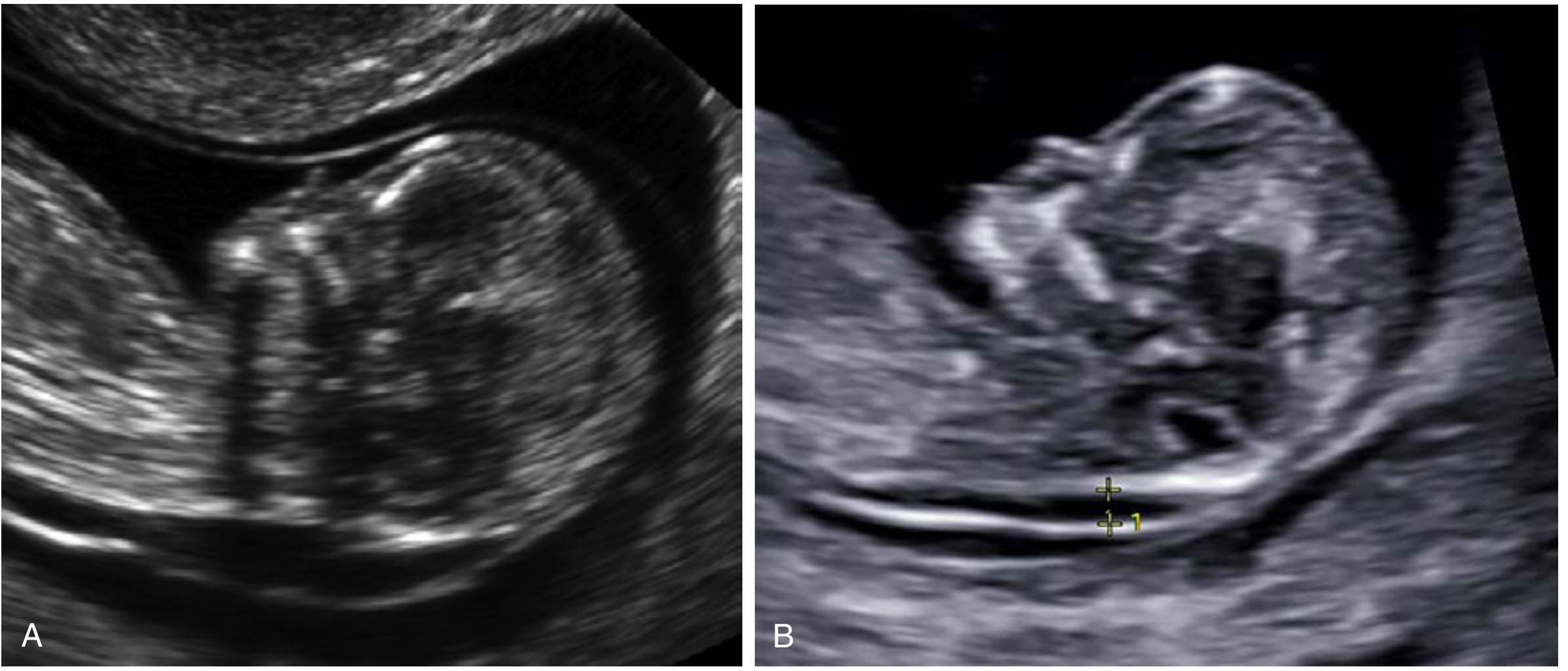
Fig 29.22 - Absent nasal bone in two different fetuses with trisomy 21. (A) Absent NB with enlarged NT. (B) Absent NB; the echogenic skin edge could be mistaken for the NB. - Creasy & Resnik's MFM
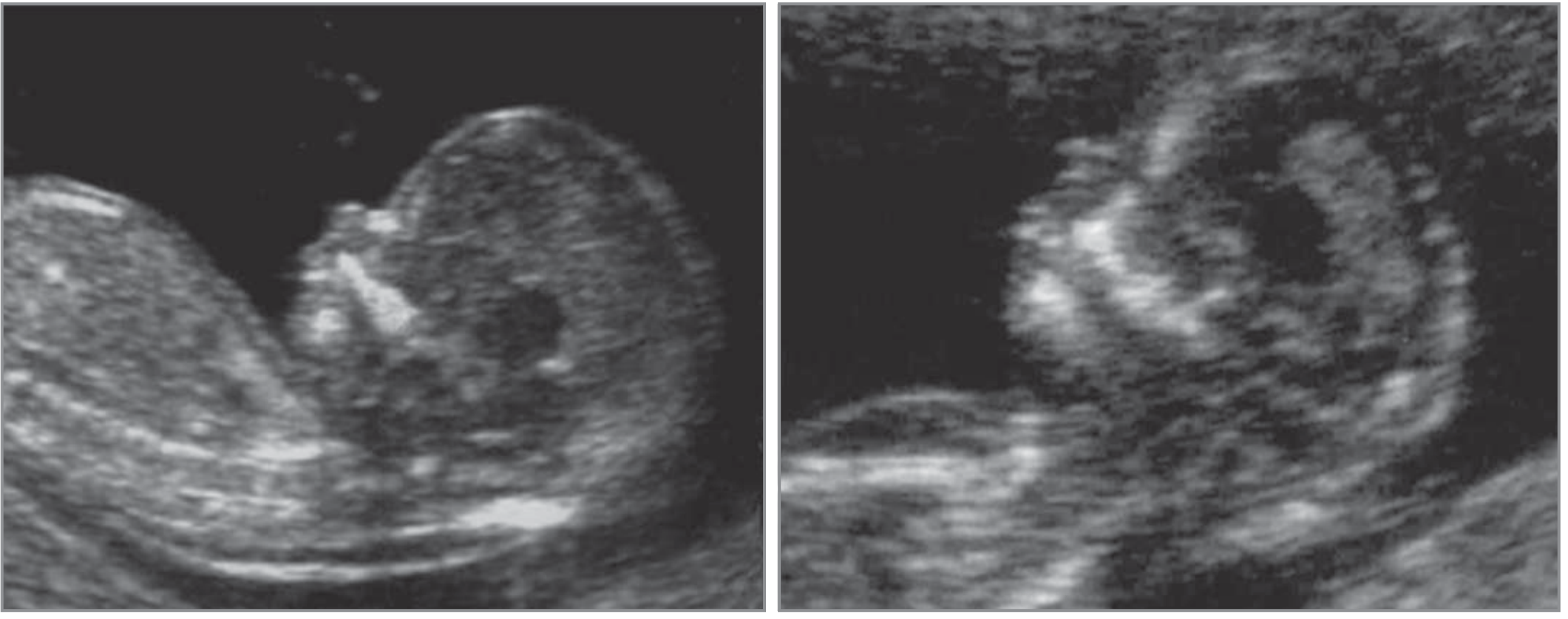
Fig 30.5 - First-trimester ultrasound: euploid fetus (left, NB present) vs. trisomy 21 fetus (right, NB absent). - Creasy & Resnik's MFM
Performance as a Screening Marker
First Trimester
| Parameter | Value |
|---|---|
| Absent NB in trisomy 21 fetuses | 73% |
| Absent NB in euploid fetuses | 0.5% |
| Sensitivity (NB alone for trisomy 21) | 65% |
| False-positive rate | 0.8% |
| Positive predictive value | ~54% (1 in 2 fetuses with absent NB had T21) |
| Likelihood ratio increase for trisomy 21 | 87-fold |
| Negative likelihood ratio | 0.35 |
Sonek et al. found that combining NB + NT + maternal age gives a 93% detection rate for Down syndrome at a 5% false-positive rate; adding serum biochemistry can push detection to 97% in high-risk populations.
Adding NB to the standard combined first-trimester screen (NT + biochemistry) reduces the false-positive rate from 5% to 2.5% while maintaining 90% detection.
Second Trimester
- Hypoplastic or absent NB occurs in up to 60% of Down syndrome pregnancies imaged in the second trimester
- Complete absence: ~37% of affected cases
- Hypoplasia: ~50% of affected cases
- In normal pregnancies: absence in 0.9%, hypoplasia in 2.4%
- May be the best single ultrasound marker for second-trimester risk assessment when performed by experienced operators
Second-trimester markers associated with Down syndrome (Box 30.2) include: brachycephaly, increased nuchal thickness, CHD, hyperechoic bowel, shortened femur/humerus, renal pyelectasis, duodenal atresia, hypoplastic 5th digit midphalanx, echogenic intracardiac focus, sandal gap foot, and short or absent nasal bone.
Ethnic Variation
This is a critical confounder. Absent NB is more common in Afro-Caribbean and southern Asian fetuses, even without aneuploidy:
| Ethnicity | Absent NB in euploid pregnancies | LR for Trisomy 21 |
|---|---|---|
| White/Caucasian | 2.5% | 31.3 |
| Afro-Caribbean | 9.0% | 8.8 |
| Southern Asian | 5.0% | 14.2 |
The NB is also more likely to be absent with increasing NT thickness in euploid pregnancies.
Proposed Screening Strategy (Two-Stage Approach)
Nikolaides et al. proposed using NB as a contingency (second-stage) marker rather than a universal first-tier screen:
- Risk ≥ 1:100 after NT + biochemistry → offer CVS directly
- Risk < 1:1000 → reassurance, no further testing
- Risk 1:101 to 1:1000 → perform NB assessment (applies to ~15% of pregnancies)
This achieves 90% DS detection at 2.5% false-positive rate without requiring universal NB assessment by all operators.
Clinical Management When Absent NB Is Found
- Isolated absent NB in first trimester (NT < 95th percentile): Low likelihood of chromosomal microarray (CMA) abnormality; not routinely an indication for invasive testing alone
- Isolated absent NB in euploid fetus without other second-trimester anomalies: Usually associated with good neonatal outcome
- Absent NB + increased NT or other markers: Significantly increases aneuploidy risk; discuss invasive diagnostic testing (CVS/amniocentesis) and/or cell-free DNA (cfDNA)
- Credentialed providers only: The NTQR and Fetal Medicine Foundation offer certification for NB assessment
Other Aneuploidies
While trisomy 21 is the primary association, absent NB has also been observed in other chromosomal anomalies. Recent chromosomal microarray studies (PMID 35506821, 38766695) show that even in second-trimester isolated absent/hypoplastic NB, pathogenic copy number variants can occasionally be found, supporting the value of CMA when combined with other risk factors.
Summary Points
- Absent NB is a first- and second-trimester soft marker strongly associated with trisomy 21
- It is assessed in the midsagittal plane at 45 degrees; the NB must be less echogenic than the overlying skin to call it absent
- Sensitivity for trisomy 21: ~65-73% (first trimester), ~60% (second trimester); false-positive rate: <1%
- Ethnic variation significantly alters the likelihood ratio - always adjust for race
- Best used as a contingency marker in intermediate-risk patients, not universal first-tier screening
- Isolated absent NB with normal NT and no other anomalies has a generally favorable prognosis
- Combined screening (NT + biochemistry + NB) achieves ~93-97% DS detection
Source: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, Chapters 18, 29, 30
Fetal medicine counselling
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.