NASAL POLYP DEFINITION, ETIOPATHOGENESIS CHART , CLINICAL FEATURES, TYPES, DIAGNOSIS, DIFFERENTIAL DIAGNOSIS, MANAGEMENT WHICH INCLUDES MEDICAL AND SURGICAL MANAGEMENT ENT
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
nasal polyp definition etiopathogenesis types clinical features diagnosis management ENT
Searching PubMed
nasal polyps chronic rhinosinusitis management
Finding Sources
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK560746/
Finding Sources
Reading Web Page
https://www.mdpi.com/2673-351X/8/2/6
Searching Images
nasal polyp endoscopy appearance bilateral ethmoid
I now have comprehensive information from multiple authoritative sources. Let me compile the complete ENT guide on nasal polyps.
🫁 NASAL POLYPS — Complete ENT Guide
1. DEFINITION
Nasal polyps are benign, inflammatory, hyperplastic outgrowths of the sinonasal mucosa arising from the mucous membrane lining of the nose and paranasal sinuses. They are pedunculated or sessile, semi-translucent, gelatinous masses most commonly originating from the ethmoid sinuses and middle meatus. They are typically bilateral, insensate (no pain on probing), avascular, and associated with Chronic Rhinosinusitis with Nasal Polyposis (CRSwNP).
Cummings Otolaryngology Head and Neck Surgery — Nasal polyps represent a subgroup of chronic rhinosinusitis characterized by Th2-driven eosinophilic mucosal inflammation.
2. ETIOPATHOGENESIS CHART
A. Predisposing Conditions / Risk Factors
| Category | Specific Conditions |
|---|---|
| Inflammatory | Chronic rhinosinusitis (CRS), allergic rhinitis |
| Immunologic | Asthma (30–50% of polyp patients), Churg-Strauss syndrome (eosinophilic granulomatosis with polyangiitis) |
| Drug-related | Aspirin-Exacerbated Respiratory Disease (AERD / Samter's triad) |
| Genetic/Systemic | Cystic fibrosis (CF — in children), Primary Ciliary Dyskinesia, Young's syndrome |
| Infective | Staphylococcus aureus colonization (superantigen stimulation) |
| Fungal | Allergic Fungal Sinusitis (AFS) |
B. Pathogenesis Flowchart
TRIGGER (allergen / infection / environmental irritant)
↓
Epithelial barrier dysfunction
(↑ permeability, ↓ tight junction proteins)
↓
Innate lymphoid cells type 2 (ILC2) activation
Epithelial cytokines: TSLP, IL-25, IL-33 released
↓
Th2-polarized immune response (predominantly in Western populations)
↓ IL-4, IL-5, IL-13 released
↓ IgE ↑ (mast cell / basophil activation)
↓ Eosinophil recruitment & activation (↑ IL-5)
↓ Tissue eosinophilia
↓
Chronic mucosal edema → pseudocyst formation
(Accumulation of albumin-rich fluid in subepithelial stroma)
↓
Stromal remodeling → polyp growth
(Fibroblast activation, ↑ vascular permeability)
↓
NASAL POLYP
────────────────────────────────────────
NOTE: In Asian populations / children with CF:
Th1/Neutrophilic endotype predominates
(TNF-α, IFN-γ driven; less eosinophilic;
more fibrotic; corticosteroid-resistant)
────────────────────────────────────────
C. Samter's Triad (AERD)
- Aspirin / NSAID sensitivity + Asthma + Nasal polyps
- Mechanism: Arachidonic acid shunted to lipoxygenase pathway → excess leukotrienes (LTC4, LTD4)
3. TYPES OF NASAL POLYPS
Classification 1: By Etiology (Sturman & Hughes)
| Type | Origin | Features |
|---|---|---|
| Ethmoidal (Allergic) | Ethmoid sinuses → middle meatus | Most common, bilateral, pale/grey, multiple, soft/gelatinous, associated with allergy/asthma |
| Antrochoanal Polyp (Killian's polyp) | Maxillary antrum → choana | Unilateral, single, extends to nasopharynx, seen in younger patients/children, no allergy association |
| Sphenochoanal Polyp | Sphenoid sinus | Rare, extends through sphenoethmoidal recess |
Classification 2: By Distribution
| Type | Description |
|---|---|
| Localized | Reactive — from inflammatory or neoplastic processes |
| Diffuse | Bilateral — associated with CRSwNP, systemic disease |
| Systemic | Associated with CF, AERD, PCD, Churg-Strauss |
Classification 3: By Histology
| Histological Type | Features |
|---|---|
| Edematous (allergic/eosinophilic) | Loose stroma, prominent eosinophils, thin epithelium — most common |
| Fibrotic | Dense fibrous stroma, few inflammatory cells — seen in CF/Asian patients |
| Glandular | Abundant glands, less edema |
| Angiomatous | Rich vascular stroma, may bleed |
4. CLINICAL FEATURES
Symptoms
| Symptom | Details |
|---|---|
| Nasal obstruction | Progressive, bilateral, most common presenting symptom |
| Hyposmia / Anosmia | Due to blockage of olfactory cleft — hallmark symptom |
| Rhinorrhea | Watery or mucoid (purulent if superinfected) |
| Postnasal drip | Sensation of secretions draining into throat |
| Nasal voice (rhinolalia clausa) | Hyponasal speech |
| Headache / facial pressure | Due to sinus ostial blockage |
| Snoring / mouth breathing | In severe obstruction |
| Taste disturbance | Related to anosmia |
| Recurrent sinusitis | Due to impaired mucociliary drainage |
Signs
| Sign | Details |
|---|---|
| Anterior rhinoscopy | Pale/grey, glistening, grape-like masses in nasal cavity |
| Bilateral masses | Arising from middle meatus — typically bilateral (unilateral = red flag) |
| Insensate on probing | No pain when touched (differentiates from turbinates) |
| Mobile on probing | Soft, compressible, move on touching |
| "Frog-face deformity" | In longstanding bilateral polyps with broadening of nasal bridge (especially children) |
| Broadening of nasal bridge | In massive polyposis — widened nasal dorsum |
Associated Features
- Asthma (30–50%)
- Allergic rhinitis
- Aspirin sensitivity
- In children: suspect cystic fibrosis (sweat chloride test mandatory)
5. DIAGNOSIS
Clinical Diagnosis
- Based on history + anterior rhinoscopy / nasal endoscopy (gold standard for visualization)
- Presence of polyps + ≥2 cardinal CRS symptoms (obstruction, discharge, facial pain/pressure, olfactory loss) lasting >12 weeks confirms CRSwNP
Investigations
| Investigation | Purpose |
|---|---|
| Anterior rhinoscopy | Initial visualization — pale grey masses |
| Rigid/Flexible nasal endoscopy | Gold standard — visualize extent, origin, osteomeatal complex involvement |
| CT Paranasal Sinuses (Coronal) | Extent of disease, pre-surgical planning, Lund-Mackay scoring; shows opacification of sinuses and polyps |
| MRI | To distinguish polyps from tumours, fungal disease; soft tissue differentiation |
| Biopsy + Histopathology | Mandatory if unilateral, suspected malignancy, atypical appearance; shows eosinophilic infiltration |
| Allergy testing (skin prick / RAST) | Identify allergen triggers |
| Spirometry | Assess for comorbid asthma |
| Sweat chloride test | In children — rule out cystic fibrosis |
| Aspirin provocation test | If AERD suspected |
| Total IgE, blood eosinophils | Assess type 2 inflammation (IgE ≥100, eos ≥250/μL → biologic criteria) |
| Smell testing (Sniffin' Sticks, UPSIT) | Quantify olfactory loss |
Grading / Staging
Nasal Polyp Score (NPS) — Endoscopic grading:
| Grade | Description |
|---|---|
| 0 | No polyp |
| 1 | Small polyp confined to middle meatus |
| 2 | Polyp reaching below middle turbinate |
| 3 | Polyp reaching below inferior turbinate |
| 4 | Polyp completely obstructing nasal cavity |
CT — Lund-Mackay Score: Scores each sinus 0–2 (total max 24) for extent of opacification.
6. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Features |
|---|---|
| Hypertrophied inferior turbinate | Pink/reddish, sensitive on probing, shrinks with vasoconstrictor, bilateral |
| Antrochoanal polyp | Unilateral, single, extends to post-nasal space in children |
| Rhinosporidiosis | Vascular, bleeds easily, strawberry appearance, endemic (South Asia); Rhinosporidium seeberi on histology |
| Inverted papilloma | Unilateral, irregular surface, harder, friable, bleeds; CT shows bony destruction |
| Nasopharyngeal angiofibroma (JNA) | Adolescent males, pulsatile mass, profuse epistaxis, CT/MRI diagnostic |
| Carcinoma of maxillary sinus | Unilateral, bony destruction on CT/MRI, irregular/friable mass, older patient |
| Encephalocele / Meningocele | Pulsatile, compressible, increases with crying/Valsalva, seen in children, CT/MRI shows defect |
| Nasal glioma | In newborns/infants, does not pulsate, does not enlarge with Valsalva |
| Mucocele | CT shows cystic expansion of sinus, eggshell bony walls |
| Lymphoma / Granulomatosis | Systemic features, ANCA testing (GPA = Wegener's) |
| Fungal ball (mycetoma) | Unilateral maxillary, CT shows calcification |
⚠️ Red flags for malignancy: Unilateral polyp, epistaxis, bony erosion on CT, facial deformity, proptosis, cranial nerve palsy → biopsy mandatory
7. MANAGEMENT
A. MEDICAL MANAGEMENT
Step 1: Topical (Intranasal) Corticosteroids — First-Line
- Drugs: Mometasone furoate, Fluticasone propionate, Budesonide, Beclomethasone
- Mechanism: Reduce eosinophilic inflammation, decrease polyp size
- Dose: 2 sprays each nostril OD/BD — long-term maintenance
- Evidence: Strongest evidence base; reduces polyp size, improves smell and nasal airflow
- Works best when polyp does not completely block access
Step 2: Saline Nasal Irrigation
- Isotonic or hypertonic saline rinses
- Clears secretions, improves mucociliary function, enhances delivery of topical steroids
Step 3: Systemic (Oral) Corticosteroids — For acute control / pre-op reduction
- Prednisolone 0.5–1 mg/kg/day × 10–14 days ("medical polypectomy")
- Rapidly reduces polyp burden before surgery or when topically inadequate
- Repeated courses with caution — risk of adrenal suppression, osteoporosis
Step 4: Antibiotics
- Doxycycline (low-dose, 20 mg BD × 3 weeks) — anti-inflammatory/anti-Staphylococcal effect, reduces polyp size short-term
- Systemic antibiotics for acute exacerbations (amoxicillin-clavulanate, clarithromycin)
- Long-term macrolides (azithromycin) — immunomodulatory effect, especially in non-eosinophilic/Th1 phenotype
Step 5: Antihistamines / Leukotriene Receptor Antagonists
- Antihistamines (cetirizine, loratadine) — for allergic component
- Montelukast (leukotriene antagonist) — especially useful in AERD/aspirin-sensitive patients; reduces relapse
Step 6: Aspirin Desensitization (AERD)
- Indicated in Samter's triad when surgery and steroids inadequate
- Gradual oral aspirin challenge under supervision → maintained on aspirin 325–650 mg BD
- Reduces polyp recurrence, improves nasal symptoms
Step 7: Biologics — For Severe Refractory CRSwNP (uncontrolled despite maximal medical/surgical treatment)
| Biologic | Target | Evidence |
|---|---|---|
| Dupilumab (Dupixent) | IL-4Rα (blocks IL-4 + IL-13) | FDA-approved; superior to surgery in some meta-analyses [PMID: 39149992]; reduces polyp score, improves olfaction |
| Mepolizumab (Nucala) | IL-5 | FDA/EMA approved for CRSwNP |
| Benralizumab | IL-5Rα | Studied in trials |
| Omalizumab (Xolair) | IgE | FDA-approved for CRSwNP; especially if high IgE/atopy |
Biologic criteria (EPOS 2020):
- Refractory to ≥2 courses oral steroids or contraindication
- NPS ≥5/8 (bilateral), SNOT-22 ≥40
- At least 2 of: tissue eos ≥10/hpf, blood eos ≥250/μL, IgE ≥100 IU/mL, anosmia, comorbid asthma
B. SURGICAL MANAGEMENT
Indications for Surgery
- Failed adequate medical therapy (≥3 months intranasal steroids + oral steroid courses)
- Massive polyposis with complete obstruction
- Complications (sinusitis, orbital/intracranial extension)
- Unilateral polyp (rule out malignancy — diagnostic excision)
- Antrochoanal polyp (does not respond to medical therapy)
Surgical Procedures
| Procedure | Description | Indication |
|---|---|---|
| Simple Nasal Polypectomy | Avulsion of polyps with Luc's forceps or suction snare under local/general anaesthesia | Historically done; high recurrence — now largely replaced |
| Endoscopic Sinus Surgery (ESS) / FESS | Functional Endoscopic Sinus Surgery — gold standard; endoscopic removal of polyps + diseased sinus mucosa; restores normal drainage via osteomeatal complex | CRSwNP, bilateral polyposis |
| FESS Components | Uncinectomy → anterior ethmoidectomy → maxillary antrostomy → posterior ethmoidectomy → sphenoidotomy → frontal recess surgery (as needed) | |
| Caldwell-Luc operation | Radical antrostomy via sublabial approach | Antrochoanal polyp (open alternative), chronic maxillary sinusitis |
| Powered Microdebrider | Suction-cutting device for precise tissue removal with less mucosal stripping | Reduces recovery time, improves results |
| Draf III (Modified Lothrop) | Extended frontal sinusotomy for frontal sinus polyps | Frontal sinus polyposis, recurrent disease |
| Image-guided surgery (IGS) | Intraoperative CT-based navigation | Revision surgery, extensive disease, close proximity to orbit/skull base |
| Antrochoanal Polyp excision | Endoscopic removal of cyst from maxillary sinus + avulsion of pedicle through middle meatus | Antrochoanal polyp — must remove intramaxillary cyst to prevent recurrence |
Principles of FESS
- Restore mucociliary drainage (not just remove polyps)
- Open osteomeatal complex (OMC) — the key drainage pathway
- Conservative mucosa preservation
- Aimed at sinus ventilation, not radical resection
- Post-op care: Saline rinses + intranasal corticosteroids mandatory to prevent recurrence
Post-Surgical Medical Therapy (Mandatory)
- Intranasal steroids — lifelong in most patients; prevents recurrence
- Saline irrigation — daily to remove debris and crusts
- Short oral steroid courses for early recurrence
- Biologics — if recurrence despite FESS + medical therapy (biologics now rival surgery for controlled disease)
Complications of Surgery
| Complication | Details |
|---|---|
| CSF leak | Breach of cribriform plate/fovea ethmoidalis |
| Orbital injury | Damage to medial rectus, optic nerve, periorbita |
| Haemorrhage | From anterior ethmoidal artery, sphenopalatine artery |
| Synechiae (adhesions) | Leading to re-obstruction |
| Recurrence | Most common "complication" — ~40–60% at 5 years without maintenance therapy |
8. ENDOSCOPIC / CLINICAL IMAGES
Nasal Polyps on Endoscopy — Bilateral Ethmoid Polyps:
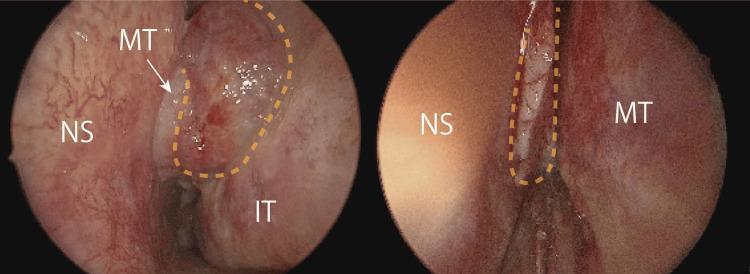
Left: Large nasal polyp (NS = nasal septum, MT = middle turbinate) | Right: Polyp in olfactory cleft — classic bilateral CRSwNP appearance
Nasal Polyp + CT Correlation:
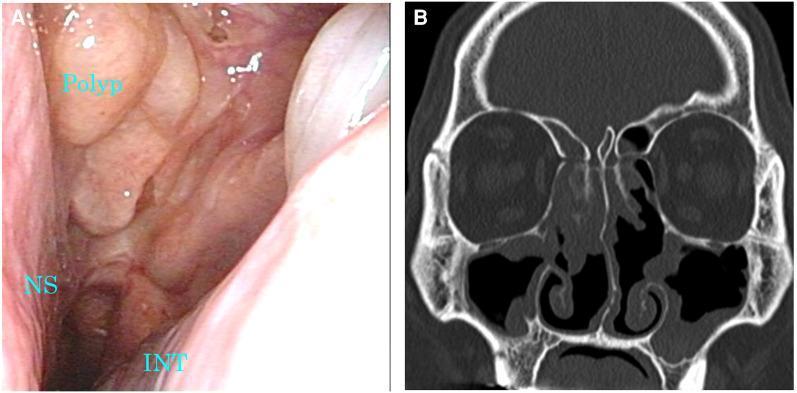
CT (Lund-Mackay scoring): bilateral ethmoid + maxillary opacification with nasal polyps on endoscopy
CT Paranasal Sinuses — Extensive Bilateral Polyposis:
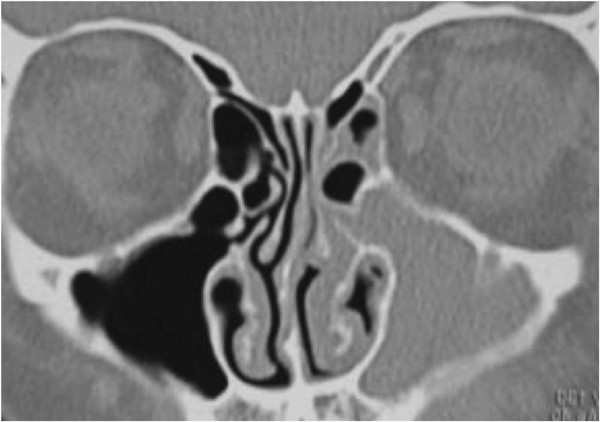
Coronal CT: Complete opacification of bilateral ethmoids and maxillary sinuses with expansion of ethmoidal air cells — classic CRSwNP
Dupilumab Response (Biologic Therapy):
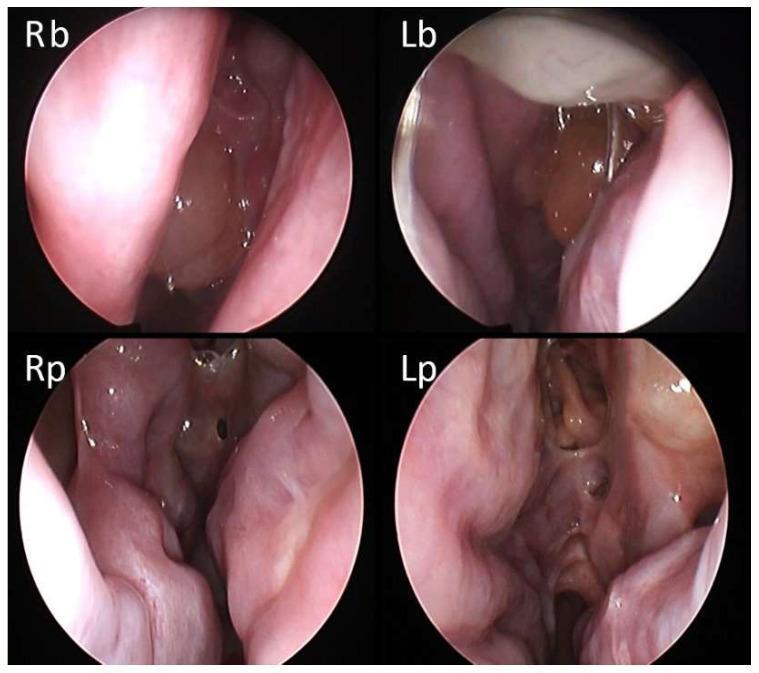
Top: Baseline NPS 5/8 | Bottom: Post-dupilumab — complete polyp regression at 1 month
9. QUICK SUMMARY TABLE
| Feature | Ethmoidal Polyp | Antrochoanal Polyp |
|---|---|---|
| Age | Adults 30s–50s | Children / young adults |
| Laterality | Bilateral | Unilateral |
| Number | Multiple | Single |
| Origin | Ethmoid sinuses | Maxillary antrum |
| Extension | Anterior nares | Posterior choana / nasopharynx |
| Allergy | Present (60–70%) | Absent |
| Histology | Eosinophilic edema | Cystic / fibrotic stroma |
| CT | Bilateral sinus opacification | Cystic mass in maxillary sinus + choana |
| Treatment | Medical (steroids) + FESS | Surgery (Caldwell-Luc or endoscopic with antral cyst removal) |
| Recurrence | High (40–60%) | Low if completely excised |
Recent Evidence (PubMed 2024–2025)
- Dupilumab vs Surgery [PMID: 39149992] — A 2024 systematic review and meta-analysis in Am J Rhinol Allergy found dupilumab comparable or superior to FESS for polyp score reduction and symptom control in CRSwNP
- Biologics in pediatric CRS [PMID: 38488239] — 2024 systematic review supports emerging role of biologics in pediatric refractory CRSwNP
- Biologic treatment landscape [PMID: 40861204] — 2025 bibliometric review confirms dupilumab as the dominant biologic, with growing evidence for mepolizumab and omalizumab
Sources: Cummings Otolaryngology Head and Neck Surgery; K.J. Lee's Essential Otolaryngology; StatPearls (NBK560746); MDPI — "What We Know about Nasal Polyposis" 2023; EPOS 2020 Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.