classify flaps. write in detail the various flaps used in head and neck surgery in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
flap reconstruction head neck surgery free flap pedicled flap
Reading File
Reading File
Loading Image
Loading Image
The images loaded perfectly. Here is the complete, exam-ready answer:
CLASSIFICATION AND FLAPS IN HEAD & NECK SURGERY
Comprehensive Answer for 50 Marks (RGUHS Standard)
INTRODUCTION
A flap is a unit of tissue transferred from a donor site to a recipient site while maintaining its own blood supply, either through an intact vascular pedicle or through microvascular re-anastomosis. Flaps are essential in head and neck (H&N) surgery for reconstruction after oncologic resection, trauma, and congenital anomalies.
The approach to reconstruction is guided by the Reconstructive Ladder (Mathes & Nahai):
╔═══════════════════════════════════════════════════════╗
║ THE RECONSTRUCTIVE LADDER ║
║ SIMPLE ─────────────────────────────── COMPLEX ║
║ ║
║ 1. Secondary intention healing ║
║ 2. Primary closure ║
║ 3. Skin graft (STSG / FTSG) ║
║ 4. Local flap ║
║ 5. Regional pedicled flap ║
║ 6. Distant pedicled flap ║
║ 7. Free microvascular tissue transfer ║
╚═══════════════════════════════════════════════════════╝
(Scott-Brown's ORL H&N Surgery; Cummings Otolaryngology H&N Surgery)
CLASSIFICATION OF FLAPS
A. Based on Blood Supply (Mathes & Nahai, 1997)
┌─────────────────────────────────────────────────────────────┐
│ CLASSIFICATION BY BLOOD SUPPLY │
├─────────────────────┬───────────────────────────────────────┤
│ RANDOM PATTERN │ AXIAL PATTERN │
│ (subdermal plexus) │ (named vessel in pedicle) │
├─────────────────────┼───────────────────────────────────────┤
│ • Rhomboid flap │ • Forehead flap (supratrochlear a.) │
│ • Z-plasty │ • Nasolabial (facial/angular a.) │
│ • Rotation flap │ • PMMC (thoracoacromial a.) │
│ • Advancement flap │ • Deltopectoral (int. mammary perfs.) │
│ • Bilobed flap │ • RFFF (radial artery) │
│ │ • ALT (LCFA descending branch) │
│ │ • Fibula (peroneal artery) │
└─────────────────────┴───────────────────────────────────────┘
In H&N, the superior blood supply allows random flap length:width ratios up to 3:1 (vs. 1:1 in the trunk).
B. Based on Tissue Composition
| Type | Components | Example |
|---|---|---|
| Cutaneous | Skin + subcutaneous fat | Rhomboid, forehead |
| Fasciocutaneous | Skin + fascia | RFFF, SAI flap |
| Myocutaneous | Muscle + overlying skin | PMMC, latissimus dorsi |
| Osseocutaneous | Bone + skin | Fibula free flap |
| Musculofascial | Muscle + fascia (no skin) | Temporalis flap |
| Visceral | Hollow organ | Jejunum |
| Composite/Chimeric | Multiple types on one pedicle | Subscapular chimeric flap |
(Cummings Otolaryngology H&N Surgery, Chapter 78)
C. Based on Location
LOCAL → Immediately adjacent to defect (nasolabial, forehead, bilobed)
↓
REGIONAL → Same anatomical region (PMMC, deltopectoral, SCM, trapezius)
↓
DISTANT → Remote site with intact pedicle (latissimus dorsi pedicled)
↓
FREE → Completely detached; microsurgical anastomosis (RFFF, ALT, fibula)
D. Based on Method of Transfer (KEY FOR EXAMS)
┌────────────────────────────────────────────────────────────────┐
│ METHOD OF MOVEMENT │
├──────────────┬─────────────────────────────────────────────────┤
│ ADVANCEMENT │ Tissue moved forward in straight line │
│ │ e.g., V-Y plasty, Rintala flap, H-flap │
├──────────────┼─────────────────────────────────────────────────┤
│ ROTATION │ Pivots in an arc around a fixed pivot point │
│ │ e.g., Cervicofacial rotation, scalp rotation │
├──────────────┼─────────────────────────────────────────────────┤
│TRANSPOSITION │ Jumps laterally over intervening intact skin │
│ │ e.g., Rhomboid (Limberg), Z-plasty, bilobed │
├──────────────┼─────────────────────────────────────────────────┤
│INTERPOLATION │ Crosses intact skin on a pedicle; 2-stage │
│ │ e.g., Forehead flap, nasolabial interpolation │
└──────────────┴─────────────────────────────────────────────────┘
(Scott-Brown's ORL H&N Surgery, block 11)
E. Mathes & Nahai Classification of Muscle Flaps (1981)
| Type | Vascular Pattern | Example |
|---|---|---|
| I | One vascular pedicle | Gastrocnemius, tensor fascia lata |
| II | One dominant + minor pedicles | Gracilis, PMMC, trapezius |
| III | Two dominant pedicles | Gluteus maximus, rectus abdominis |
| IV | Segmental pedicles | Sartorius, tibialis anterior |
| V | One dominant + secondary segmental | Latissimus dorsi, pectoralis major |
FLAP SELECTION FLOWCHART
HEAD & NECK DEFECT REQUIRING RECONSTRUCTION
│
┌────────────────────┼───────────────────┐
▼ ▼ ▼
SMALL (<2cm) MEDIUM (2-6cm) LARGE / COMPLEX
Superficial Moderate depth Deep or composite
│ │ │
Primary closure Local flap ┌────┴─────┐
or FTSG/STSG (advancement, REGIONAL FREE FLAP
rotation, PEDICLED
transposition, (PMMC, DP,
interpolation) Trapezius,
SAI flap)
│
Previous surgery / RT?
YES → FREE FLAP preferred
NO → Pedicled acceptable
I. LOCAL FLAPS IN HEAD & NECK
1. Advancement Flaps
a. V-Y Advancement Flap
- Island of tissue advanced forward; V-shaped incision closed as Y
- Flap designed ~2x defect size
- Uses: nasal tip, columella, cheek, periorbital defects
b. Rintala Flap (Vertical Forehead Advancement)
- Midline vertical advancement from nasion to hairline
- Used for nasal dorsum defects up to 2 cm
- (Scott-Brown's block 12, line 4160)
c. Cheek Advancement (Mustarde)
- Large skin mobilized from cheek and neck
- Used for lower eyelid and malar defects
- Extended with Z-plasty / back-cut for better reach
2. Rotation Flaps
Cervicofacial Rotation Flap
- Skin from cheek-neck rotated superiorly
- Based on facial artery perforators
- Uses: large cheek, malar, lower eyelid defects
- Danger: facial nerve branches in the flap
3. Transposition Flaps
a. Z-plasty
- Two equilateral triangular flaps transposed across central limb
- 60° angles give 75% scar lengthening
- Uses: scar revision, contracture release, lengthening oral commissure
b. Rhomboid (Limberg) Flap
- Parallelogram-shaped transposition flap
- Four possible flap orientations for any rhomboid defect
- Uses: cheek, temple, lateral nose, postauricular, scalp
c. Bilobed Flap (Zitelli Modification)
- Two lobes: first fills primary defect, second fills first donor
- Each lobe at 45° arc (Zitelli); originally 90° (McGregor)
- Uses: nasal tip, alar reconstruction - preferred for defects <1.5 cm alar
- (Scott-Brown's block 11)
d. Banner Transposition Flap
- Long, narrow flap transposed 90-180°
- Used for small nasal, eyelid defects
4. Interpolation Flaps
a. Forehead (Paramedian Forehead) Flap
- Based on supratrochlear artery (axial pattern)
- Oldest flap in surgery - described by Susruta, 600 BC
- Oblique or vertical design across forehead
- Two-stage procedure: Stage 1 - flap raised, tip inset; Stage 2 at 3 weeks - pedicle divided
- Optional Stage 3 for nasal tip thinning and refinement
- Donor: primary closure if width <2.5 cm; STSG or secondary healing if wider
- Primary indication: nasal reconstruction (subtotal and total nasal defects)
- (Scott-Brown's ORL H&N Surgery, block 12, line 4172-4175)
b. Nasolabial Flap
- Superiorly based: angular artery (branch of facial artery)
- Inferiorly based: labial vessels
- Rich blood supply; one of the most reliable local flaps
- Can be folded on itself for through-and-through defects
- Uses: alar reconstruction, floor of mouth, buccal mucosa, palate
- Pedicle divided at 3 weeks
- (Scott-Brown's block 11, line 8174)
II. REGIONAL PEDICLED FLAPS
1. Deltopectoral (DP) Flap
- Described by Bakamjian (1965) - first major axial skin flap described
- Based on 2nd, 3rd, 4th perforators of internal mammary artery
- Fasciocutaneous; extends from sternum across chest to deltoid
- Dimensions: ~20 x 9 cm
- Two-stage: flap raised and inset → pedicle divided at 3 weeks
- Uses: pharyngeal reconstruction, cervical esophagus, neck skin cover, salvage after PMMC failure
- Disadvantage: hair-bearing in men; limited arc of rotation; donor site requires STSG
2. Pectoralis Major Myocutaneous Flap (PMMC)
- Described by Ariyan (1979) - transformed H&N reconstruction
- Blood supply: Pectoral branch of thoracoacromial artery (dominant) + lateral thoracic artery
- Mathes & Nahai Type V muscle
- Pivot point: below medial clavicle
- Skin paddle designed over lower pectoralis muscle, overlying 4th-6th ribs
- Can include a segment of rib (composite flap)
PMMC FLAP ANATOMY:
┌──────────────────────────┐
Thoracoacromial ──► PECTORALIS MAJOR │
artery MUSCLE │
(pectoral branch) │ │
│ [SKIN PADDLE] │
│ (over lower 1/3) │
└──────────────────────────┘
│
TUNNELLED UNDER
SKIN OF CHEST/NECK
│
DEFECT SITE
(oral cavity /
pharynx / neck)
Advantages:
- Reliable blood supply
- Large volume of tissue
- Single-stage, same operative field
- Can protect carotid artery (muscle-only)
- Can include rib for composite reconstruction
Disadvantages:
- Bulky (especially obese, large-breasted patients)
- Hair-bearing in males
- Limited reach to skull base
- Poor colour/texture match for face
- Shoulder weakness in some patients
Indications:
- Total/subtotal glossectomy
- Hypopharyngeal defects
- Skin cover post-neck dissection
- Carotid blowout protection
- Salvage after free flap failure
3. Sternocleidomastoid (SCM) Flap
- Blood supply: occipital artery (superior third), superior thyroid artery (middle), transverse cervical artery (inferior)
- Used as muscle-only or myocutaneous flap
- Superior-based SCM flap: parotid region, lower face
- Inferior-based SCM flap: hypopharynx, tracheostoma reconstruction
- Critical limitation: NOT reliable after radical neck dissection (Type III) - accessory nerve divided; SCM devascularized
- Uses: small pharyngeal defects, parotidectomy cover, orocutaneous fistula closure
4. Trapezius Flap
Three anatomically distinct variants:
| Variant | Blood Supply | Reach | Use |
|---|---|---|---|
| Superior trapezius | Occipital artery | Posterior scalp, occiput | Posterior scalp/neck |
| Middle trapezius | Transverse cervical artery | Neck, lower face | Lateral neck skin |
| Lower trapezius island | Deep branch transverse cervical (dorsal scapular a.) | Skull base, oropharynx | Greatest reach |
5. Latissimus Dorsi Flap
- Thoracodorsal artery (branch of subscapular system)
- Mathes & Nahai Type V
- Can provide up to 25 x 15 cm skin paddle + large muscle volume
- Can be used as pedicled (posterior neck, scalp) or free flap
- Uses: scalp reconstruction (entire scalp), posterior neck, large trunk defects
6. Temporalis Muscle Flap
- Deep temporal artery (branch of internal maxillary artery)
- Rotation through infratemporal fossa (coronoid removed for access)
- Provides thin, pliable musculofascial tissue
- Uses: orbital exenteration lining, palate reconstruction, maxillary defects, facial nerve reanimation
- Disadvantage: temporal hollowing at donor site
7. Supraclavicular Artery Island (SAI) Flap
- Described by Lamberty (1979), systematized by Pallua
- Based on branch of transverse cervical artery
- Pedicle origin within the triangle: posterior border SCM (anterior), external jugular vein (posterior), clavicle (inferior)
- Dimensions: up to 30 cm length, 12 cm width
- Fasciocutaneous flap from shoulder and supraclavicular area
(Diagram from Scott-Brown's ORL H&N Surgery, Vol 3):
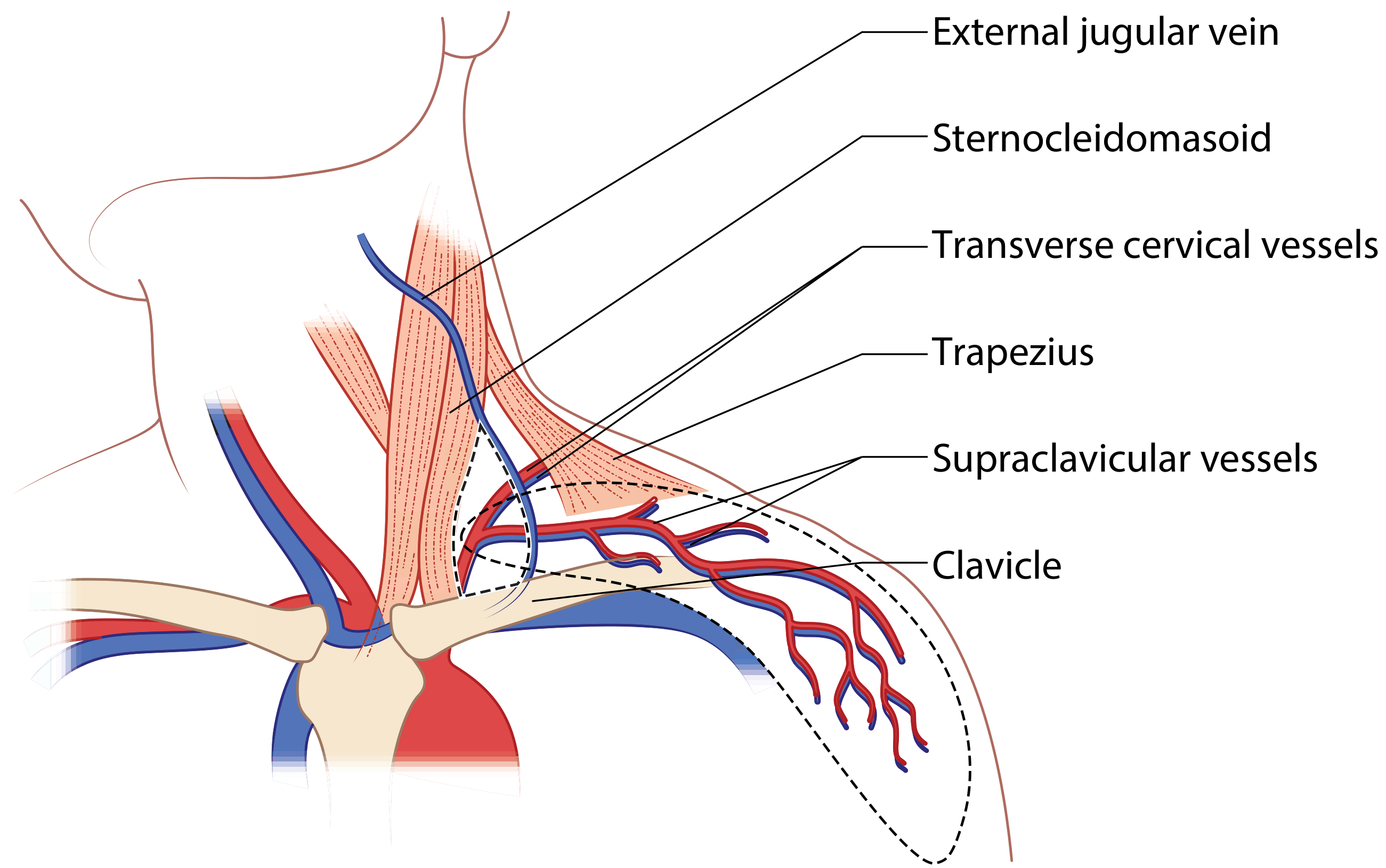
Uses: hypopharyngeal defects, cervical esophagus, neck skin cover after radical resection
Advantages: thin/pliable, same skin colour as H&N, single-stage, avoids microsurgery
(Scott-Brown's block 12, lines 4941-4975)
III. FREE FLAPS (MICROVASCULAR TISSUE TRANSFER)
Free flaps represent the standard of care for complex H&N reconstruction. Success rates exceed 95% at experienced centres.
FREE FLAP SELECTION FLOWCHART:
COMPLEX H&N DEFECT REQUIRING FREE FLAP
│
┌───────────────────┼──────────────────┐
▼ ▼ ▼
SOFT TISSUE BONY DEFECT VISCERAL TUBE
DEFECT ONLY (+/- soft tissue) (pharynx/esophagus)
│ │ │
┌────┴────┐ ┌────┴────┐ ┌────┴────┐
│ THIN │ │MANDIBLE │ │Jejunum │
│→ RFFF │ │→ Fibula │ │OR tubed │
│ or │ │ free │ │RFFF/ALT │
│Scapular │ │ flap │ └─────────┘
└────┬────┘ │MAXILLA │
│ │→ Fibula │
┌────┴────┐ │ Scapula │
│ BULKY │ │ Iliac │
│→ ALT or │ └─────────┘
│ TRAM/ │
│ DIEP │
└─────────┘
1. Radial Forearm Free Flap (RFFF / "Chinese Flap")
- Described by Yang et al. (1981)
- Based on radial artery + paired venae comitantes + cephalic vein
- Fasciocutaneous; thin and pliable
- Dimensions: up to 10 x 35 cm
- Allen test mandatory before harvest (confirm ulnar collateral adequacy)
- Donor site requires STSG for defects >4 cm
Advantages:
- Thin, pliable - ideal for mucosal lining
- Long pedicle (up to 20 cm)
- Reliable, consistent anatomy
- Can be made sensate (medial/lateral cutaneous nerve of forearm)
- Can be tubed for pharyngeal/cervical esophageal reconstruction
Disadvantages:
- Sacrifice of radial artery
- Donor site morbidity (cold intolerance, STSG cosmesis)
- Not suitable for large volumetric defects
Uses in H&N: tongue (most common), floor of mouth, buccal mucosa, soft palate, pharynx
2. Anterolateral Thigh Flap (ALT Flap)
- Described by Song et al. (1984)
- Based on descending branch of lateral circumflex femoral artery (LCFA)
- Perforators run through or between vastus lateralis and rectus femoris
- Can be raised as fasciocutaneous, myocutaneous (with vastus lateralis), or chimeric
- Dimensions: up to 25 x 15 cm
- Now the most commonly used free flap for H&N reconstruction worldwide
Advantages:
- Large, adjustable skin paddle
- Minimal donor morbidity (primary closure if <8 cm width)
- Can include fascia lata as sling, or include motor nerve to VL
- Chimeric options (multiple paddles, muscle component)
- Can be thinned for mucosal lining
- Simultaneous two-team surgery possible
Disadvantages:
- Variable perforator anatomy (5-10% may need to abandon ALT)
- Thick in obese patients (may need thinning/defatting)
Uses: large pharyngeal/hypopharyngeal defects, total glossectomy, base of tongue, massive skin defects, facial/scalp resurfacing; can be tubed for pharyngeal reconstruction
3. Fibula Free Flap (Osteocutaneous Fibula)
- Described by Hidalgo (1989)
- Based on peroneal artery (septocutaneous or musculocutaneous perforators to skin paddle)
- Provides up to 25 cm of bicortical bone (most donatable bone in the body)
- Gold standard for mandibular reconstruction (Cummings, block 16; Molteni et al. 2023 systematic review [PMID 37269408])
- Preoperative CTA or Duplex to confirm 3-vessel flow and perforator location
- Multiple osteotomies possible (periosteum preserved between cuts)
- Adequate bone stock for dental implants
(From Cummings Otolaryngology H&N Surgery, Chapter 78 - Osteocutaneous fibula free flap):
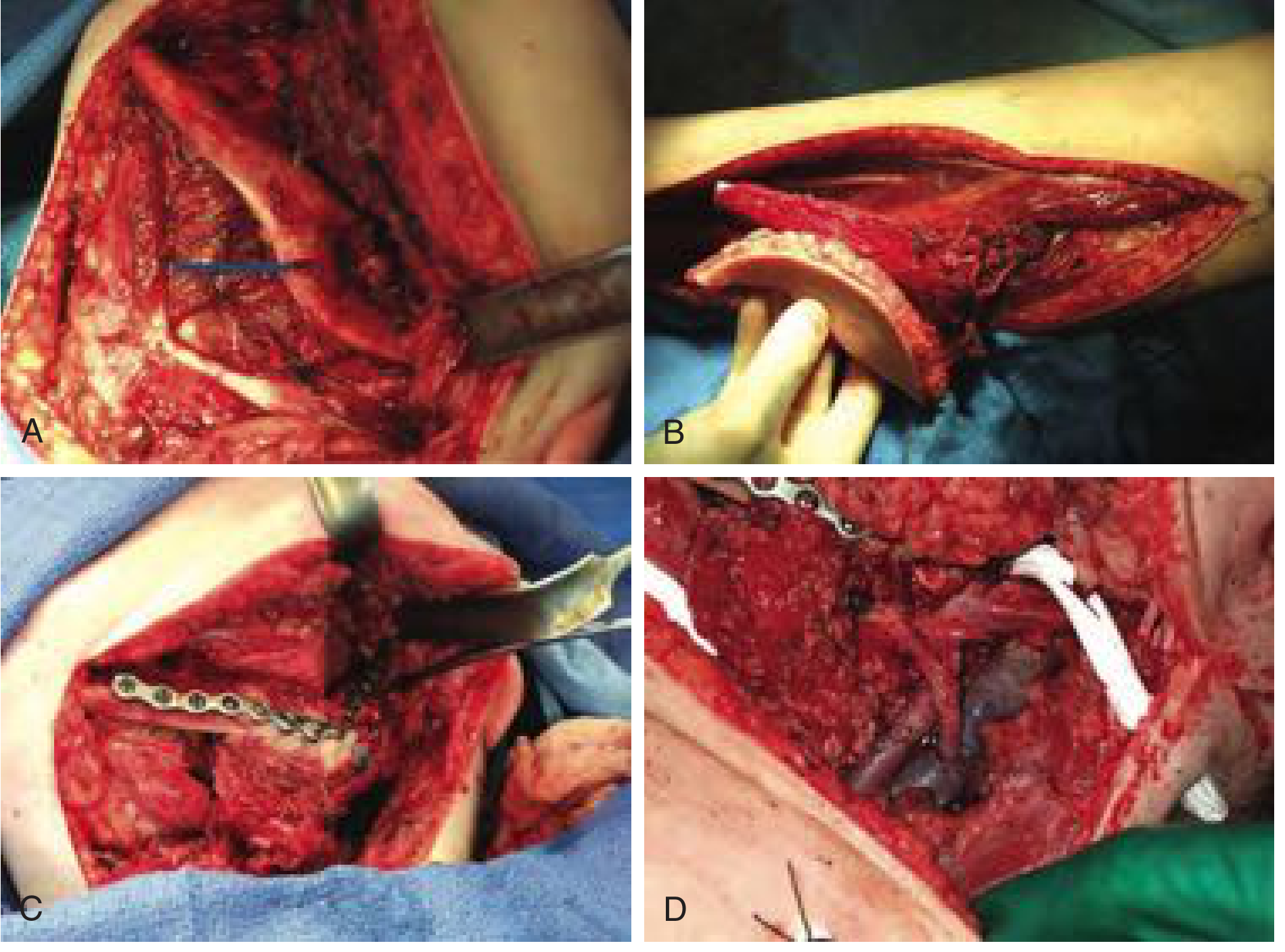
Uses: mandibular reconstruction (primary), maxillary reconstruction, skull base
Disadvantages: variable skin paddle, limited soft tissue bulk, prolonged ambulation difficulty postop
4. Rectus Abdominis Free Flap (TRAM / DIEP)
- TRAM: Transverse Rectus Abdominis Myocutaneous - based on deep inferior epigastric artery
- DIEP: pure perforator flap (skin + fat only, muscle spared) - less donor morbidity
- Large skin paddle with substantial soft tissue volume
- Uses in H&N: total glossectomy, skull base, massive scalp reconstruction, laryngectomy defects
- Disadvantage: bulky; abdominal hernia risk with TRAM; longer OR time
5. Jejunal Free Flap
- Segment of jejunum on superior mesenteric vessels
- Used for circumferential pharyngeal/esophageal reconstruction
- Provides mucosa-lined tube resembling native esophagus
- Requires laparotomy (bowel harvest + intestinal anastomosis)
- Being increasingly replaced by tubed RFFF or tubed ALT in experienced centres
- Disadvantages: laparotomy morbidity; "wet" pharyngeal voice; poor radiation tolerance; monitoring difficult
6. Scapular / Parascapular Free Flap
- Based on circumflex scapular artery (branch of subscapular system)
- Thin fasciocutaneous; skin paddle up to 14 x 10 cm
- Can be combined as chimeric subscapular system flap (with LD muscle and/or scapular bone)
- Uses: oral cavity, neck skin, scalp, composite midface
- Recent meta-analysis (McGregor et al. 2024, [PMID 39045822]): acceptable donor site morbidity, but shoulder abduction and flexion limited; physiotherapy is essential postoperatively
7. Temporoparietal Fascia (TPF) Flap
- Based on superficial temporal artery and vein
- Can be used as regional pedicled or free flap
- Thin vascularized fascial sheet (2-3 mm) - excellent for covering cartilage frameworks
- Uses: auricular reconstruction, tracheal reconstruction, orbital reconstruction, facial contouring
- Systematic review (Horen et al. 2021, [PMID 34387574]): highly reliable for complex 3D defects
IV. FLAP PHYSIOLOGY AND SURVIVAL
(Cummings Otolaryngology H&N Surgery, Chapter 77)
Zones of Perfusion (Johnson & Barker):
| Zone | Components | Clinical Relevance |
|---|---|---|
| Zone I | Macrovascular (arteries, veins, neural control) | Flap delay phenomenon occurs here |
| Zone II | Capillary microcirculation (arterioles, venules) | "No-reflow phenomenon" |
| Zone III | Interstitial space | Nutrient diffusion/convection |
| Zone IV | Cellular level | Ischemia-reperfusion injury |
Flap Delay Phenomenon:
- Preliminary surgery 2-3 weeks before definitive transfer
- Causes adrenergic desensitization → choke vessel vasodilation
- Converts random zones to axial pattern → increases survival 30-40%
Causes and Management of Flap Failure:
| Cause | Sign | Management |
|---|---|---|
| Arterial thrombosis | Pale, cool, no Doppler signal | Urgent re-exploration (<6 hrs) |
| Venous congestion | Dusky, swollen, brisker cap refill | Leech therapy, heparin |
| Vasospasm | Pale, intermittent Doppler | Papaverine, warming |
| Haematoma | Tense swelling | Surgical evacuation |
| Infection | Cellulitis, discharge | Debridement, antibiotics |
| Pedicle kinking/tension | Variable | Re-inset, release compression |
V. FREE FLAP MONITORING
(Cummings Otolaryngology H&N Surgery)
| Method | Principle | Advantage |
|---|---|---|
| Clinical (hourly) | Colour, turgor, capillary refill, temperature | Free, always available |
| Handheld Doppler | Perforator signal in skin paddle | Simple bedside tool |
| Implantable Doppler (Cook-Swartz) | Continuous pedicle monitoring | Gold standard for buried flaps |
| Near-infrared spectroscopy (NIRS) | Tissue oxygen saturation | Non-invasive, continuous |
| Fluorescein/ICG angiography | Perfusion mapping intraoperatively | Real-time perfusion assessment |
VI. COMPREHENSIVE NAMED FLAP SUMMARY TABLE
| Flap | Blood Supply | Type | Primary H&N Indication |
|---|---|---|---|
| Paramedian forehead | Supratrochlear a. | Axial local | Nasal reconstruction |
| Nasolabial | Angular/facial a. | Axial local | Alar, floor of mouth |
| Glabellar | Angular a. | Axial local | Nasal root/upper bridge |
| Rhomboid (Limberg) | Random subdermal | Random local | Cheek, temple, scalp |
| Bilobed (Zitelli) | Random subdermal | Random local | Nasal tip and ala |
| Cervicofacial rotation | Facial perforators | Random/axial | Cheek, lower eyelid |
| Deltopectoral (Bakamjian 1965) | Int. mammary perforators 2-4 | Axial fasciocutaneous | Pharynx, neck skin |
| PMMC (Ariyan 1979) | Thoracoacromial pectoral br. | Myocutaneous | Oral cavity, pharynx, neck |
| SCM myocutaneous | Occipital / sup. thyroid a. | Myocutaneous | Parotid cover, hypopharynx |
| Trapezius | Transverse cervical / occipital | Myocutaneous | Skull base, posterior neck |
| Latissimus dorsi | Thoracodorsal a. | Myocutaneous | Scalp, posterior neck |
| Temporalis | Deep temporal a. | Musculofascial | Orbit, palate, midface |
| SAI flap (Lamberty 1979) | Transverse cervical branch | Fasciocutaneous | Hypopharynx, neck skin |
| RFFF (Yang 1981) | Radial artery | Fasciocutaneous free | Tongue, floor of mouth |
| ALT (Song 1984) | LCFA descending branch | Fasciocutaneous free | Pharynx, oral cavity, skin |
| Fibula (Hidalgo 1989) | Peroneal artery | Osseocutaneous free | Mandible, maxilla |
| Jejunum | Superior mesenteric a. | Visceral free | Pharynx, cervical esophagus |
| TRAM/DIEP | Deep inf. epigastric a. | Myocutaneous/perforator free | Total glossectomy, skull base |
| Scapular | Circumflex scapular a. | Fasciocutaneous free | Oral cavity, neck skin |
| TPF | Superficial temporal a. | Fascial (free/pedicled) | Ear, orbit, trachea |
VII. RECENT ADVANCES
-
Perforator Flaps - Pure fasciocutaneous flaps (DIEP, ALT, PAP) that spare underlying muscle; reduce donor site functional morbidity significantly compared to myocutaneous flaps.
-
Chimeric / Conjoined Free Flaps - Multiple tissue components harvested on a single vascular axis (e.g., subscapular system: scapula bone + LD muscle + parascapular skin) for complex composite 3D defects in a single-stage free flap.
-
Virtual Surgical Planning (VSP) + CAD/CAM Cutting Guides - Computer-planned osteotomies with pre-bent titanium plates and cutting guides for fibula mandibular reconstruction; now standard of care at major centres; improves symmetry and accuracy.
-
Pre-fabricated and Pre-laminated Flaps - Cartilage or bone frameworks implanted at donor site weeks before transfer; used for total nasal and auricular reconstruction.
-
Supermicrosurgery - Anastomosis of vessels <0.8 mm; enables perforator-to-perforator anastomoses; valuable in irradiated fields with limited conventional recipient vessels.
-
Robotic / Video-assisted Flap Harvest - Minimally invasive latissimus dorsi harvest; smaller scars, faster recovery.
-
Impact of Adjuvant Radiotherapy on Free Flaps - Meta-analysis (Pfister et al. 2024, [PMID 38401274]): adjuvant radiochemotherapy causes significant free flap volume reduction over time; counselling needed regarding long-term functional outcomes.
-
Mandibular Reconstruction - Systematic review (Molteni et al. 2023, [PMID 37269408]): fibula free flap confirmed gold standard; scapula preferred for composite midface; VSP improves outcomes.
-
Scapula Free Flap Morbidity - Meta-analysis (McGregor et al. 2024, [PMID 39045822]): scapular donor site shoulder abduction and flexion limitations; early physiotherapy is mandatory.
-
Postoperative ICU vs. Non-ICU Care for Free Flaps - Meta-analysis (Mashrah et al. 2022, [PMID 34992114]): non-ICU monitored settings with dedicated nursing protocols show comparable flap survival to ICU; enables resource optimization.
COMPLETE SUMMARY FLOWCHART
╔══════════════════════════════════════════════════════════════════╗
║ CLASSIFICATION OF FLAPS ║
╠══════════════════════════════════════════════════════════════════╣
║ │ ║
║ ┌──────────────────────┼──────────────────────┐ ║
║ ▼ ▼ ▼ ║
║ BY BLOOD BY TISSUE TYPE BY MOVEMENT ║
║ SUPPLY ──────────────── ──────────── ║
║ ───────── Cutaneous Advancement ║
║ Random pattern Fasciocutaneous Rotation ║
║ Axial pattern Myocutaneous Transposition ║
║ Osseocutaneous Interpolation ║
║ Visceral ║
║ Chimeric/Composite ║
║ ║
║ ┌────────────────┼───────────────────┐ ║
║ ▼ ▼ ▼ ║
║ LOCAL FLAPS REGIONAL FLAPS FREE FLAPS ║
║ ────────── ────────────── ────────── ║
║ Advancement Deltopectoral RFFF ║
║ Rotation PMMC ALT ║
║ Transposition SCM Fibula ║
║ Interpolation Trapezius Jejunum ║
║ Forehead Latissimus dorsi TRAM/DIEP ║
║ Nasolabial Temporalis Scapular ║
║ Rhomboid SAI flap TPF ║
║ Bilobed ║
╚══════════════════════════════════════════════════════════════════╝
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (8th Ed, Gleeson) - Chapters 85, 91, 92: Local flaps, nasal reconstruction, supraclavicular flap
- Cummings Otolaryngology Head and Neck Surgery (7th Ed, Flint) - Chapters 77-78: Skin flap physiology, free tissue transfer, osteocutaneous flaps
- Ariyan S. The pectoralis major myocutaneous flap. Plast Reconstr Surg 1979; 63:73-81
- Bakamjian VY. A two-stage method for pharyngoesophageal reconstruction. Plast Reconstr Surg 1965; 36:173
- Hidalgo DA. Fibula free flap: a new method of mandible reconstruction. Plast Reconstr Surg 1989; 84:71-79
- Song YG et al. The free thigh flap: a new free flap concept based on the septocutaneous artery. Br J Plast Surg 1984
- Mathes SJ, Nahai F. Classification of the vascular anatomy of muscles. Plast Reconstr Surg 1981; 67:177-187
- Molteni G et al. Mandibular reconstruction in HNC: which is the gold standard? Eur Arch Otorhinolaryngol 2023 (PMID 37269408)
- Pfister P et al. Impact of adjuvant radiochemotherapy on free flap volume in H&N reconstruction. J Plast Reconstr Aesthet Surg 2024 (PMID 38401274)
- McGregor S et al. Donor site morbidity after scapula free flap in H&N reconstruction. Head Neck 2024 (PMID 39045822)
- Mashrah MA et al. Postoperative care after head and neck free-flap surgery. BMJ Open 2022 (PMID 34992114)
- Horen SR et al. Temporoparietal Fascial Free Flap: A Systematic Review. Ann Plast Surg 2021 (PMID 34387574)
- Dhingra PL & Dhingra S - Diseases of ENT Head and Neck Surgery (6th Ed)
- Hazarika P - Textbook of ENT and Head & Neck Surgery (clinical integration)
RGUHS Exam Tip: This is a standard 50-mark question. Cover all four main sections: Classification (10 marks) → Local flaps with diagrams (10 marks) → Regional pedicled flaps - PMMC and DP in particular detail (15 marks) → Free flaps - RFFF, ALT, Fibula (10 marks) → Flap failure + monitoring + recent advances (5 marks). The Reconstructive Ladder, classification flowchart, PMMC anatomy diagram, and bilobed flap diagram are mandatory for full marks.
This is a shared conversation. Sign in to Orris to start your own chat.