Pulsus paradoxusus
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough summary of pulsus paradoxus from authoritative medical textbooks.
Pulsus Paradoxus
Definition
Pulsus paradoxus is a fall in systolic blood pressure >10 mm Hg during inspiration. It is an exaggeration of the normal physiologic inspiratory decrease in systolic BP (normally ≤10 mm Hg). An abnormal value is generally taken as >12 mm Hg, though some sources use >10 mm Hg as the cut-off.
- Harrison's Principles of Internal Medicine 22E, p. 1906
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 44
Pathophysiology
The physiology is best understood through ventricular interdependence and three simultaneous effects of inspiration:
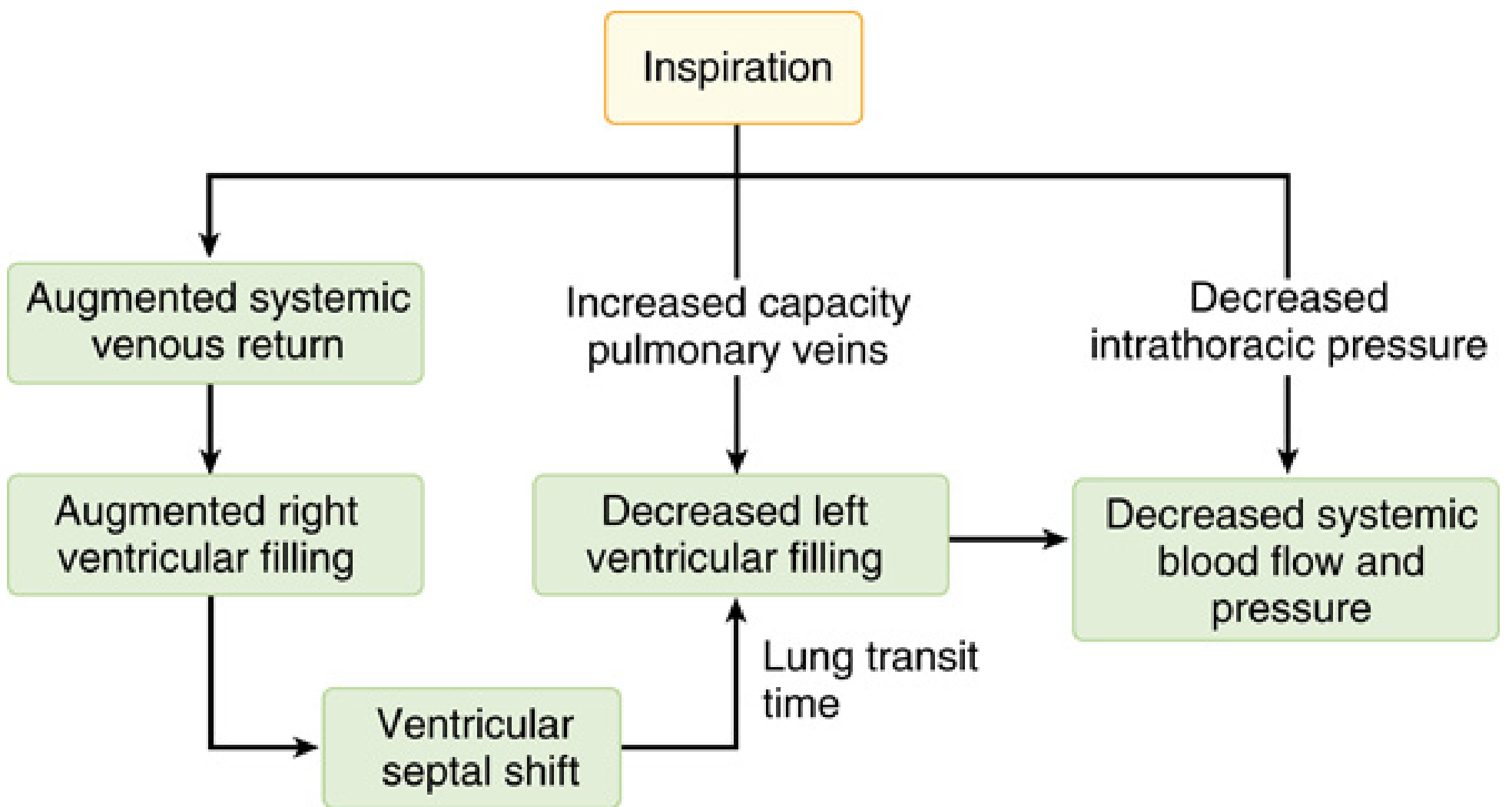
Physiology of paradoxical pulse (Miller's Anesthesia, 10e, Fig. 50.68)
- Augmented systemic venous return → increased RV filling → interventricular septal shifts leftward ("septal shift") → decreased LV filling
- Increased pulmonary vein capacitance → pulmonary veins pool blood → less blood reaching the left heart (also compounded by lung transit time delay)
- Decreased intrathoracic pressure → the aorta "hangs" in the thorax; decreased pressure does not transmit as effectively to systemic circulation
The net result of all three mechanisms is decreased LV stroke volume and systolic BP during inspiration - the "paradox" being that the heart still beats but the pulse disappears or diminishes.
Causes
| Category | Examples |
|---|---|
| Cardiac tamponade | Most classic cause; marked pulsus (20-30+ mm Hg) |
| Obstructive lung disease | Severe asthma, COPD |
| Tension pneumothorax | Wide swings in intrathoracic pressure |
| Massive pulmonary embolism | |
| Hemorrhagic/hypovolemic shock | |
| Constrictive pericarditis | (less commonly) |
- Miller's Anesthesia, 10e, p. 7763; Harrison's 22E, p. 1906
Conditions Where Pulsus Paradoxus is Absent Despite Tamponade
Pulsus paradoxus may be absent in cardiac tamponade when:
-
Aortic insufficiency (AI) is coexistent - AR creates its own aortic flow dynamics
-
Atrial septal defect (ASD) - equalizes pressures between chambers
-
Pre-existing elevated LVEDP from LV hypertrophy or dilatation - the LV is already stiff and cannot fill more during expiration, so there is no baseline to exaggerate
-
Miller's Anesthesia, 10e, p. 7763
Measurement Technique
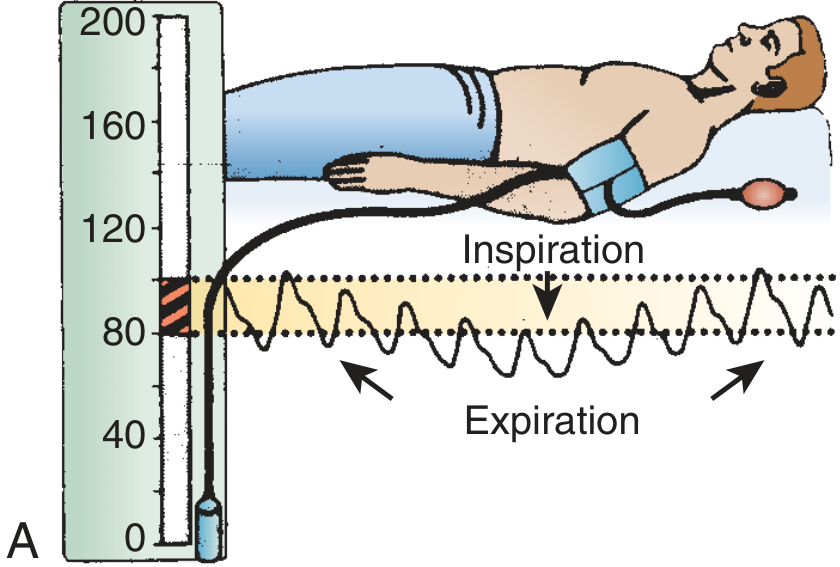
Blood pressure cuff method showing systolic variation with respiration (Roberts and Hedges)
Step-by-step sphygmomanometer method:
- Patient reclines at 30-45 degrees, breathing normally.
- Inflate BP cuff above systolic pressure.
- Slowly deflate - note the pressure at which Korotkoff sounds first appear (during expiration only).
- Continue deflating - note the pressure at which Korotkoff sounds are heard throughout the full respiratory cycle (both inspiration and expiration).
- The difference between these two pressures = pulsus paradoxus in mm Hg.
Key numbers:
- Normal: ≤10 mm Hg variation
- Abnormal: >12 mm Hg
- Moderate-severe tamponade: typically 20-30 mm Hg or more
- Palpable at the brachial or femoral artery when the difference exceeds ~15 mm Hg
Alternative methods: Pulse oximetry plethysmography - visually observe loss and reappearance of the waveform during the respiratory cycle (validated in ICU settings).
Limitations of measurement: Difficult to measure accurately in tachycardia, atrial fibrillation, or tachypnea.
- Roberts and Hedges, p. 44; Harrison's 22E, p. 1906
Clinical Significance
| Pulsus (mm Hg) | Interpretation |
|---|---|
| ≤10 | Normal |
| 10-20 | Mild-moderate tamponade or obstructive lung disease |
| >20-25 | Moderate-severe tamponade (in absence of hypotension: sensitive and specific) |
| >25 | High specificity for moderate/severe tamponade |
An echocardiographic validation study found pulsus paradoxus had a sensitivity of 79% and specificity of 40% for right ventricular diastolic collapse (a marker of significant tamponade). Note: in advanced tamponade with very narrow pulse pressure, the absolute pulsus paradoxus may be deceptively small (only 5-15 mm Hg) even with significant hemodynamic compromise.
Comparison: Pulsus Paradoxus vs. Pulsus Alternans
| Feature | Pulsus Paradoxus | Pulsus Alternans |
|---|---|---|
| Pattern | Respiratory variation in amplitude | Beat-to-beat variation, independent of respiration |
| Cause | Tamponade, obstructive lung disease, PE, shock | Severe LV systolic dysfunction |
| Mechanism | Ventricular interdependence, intrathoracic pressure swings | Cyclic changes in intracellular Ca²⁺ and action potential duration |
| Associated finding | Beck's triad (in tamponade) | ECG T-wave alternans (arrhythmic risk) |
- Harrison's Principles of Internal Medicine 22E, p. 1906-1907
This is a shared conversation. Sign in to Orris to start your own chat.