alopecia areata treatment
Reading File
Finding Sources
Searching PubMed
"alopecia areata"[MeSH Terms] AND treatment
Searching the Web
alopecia areata treatment guidelines 2025 JAK inhibitors baricitinib ritlecitinib
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive, up-to-date overview of alopecia areata treatment.
Alopecia Areata - Treatment
Pathophysiology (Why the Treatments Work)
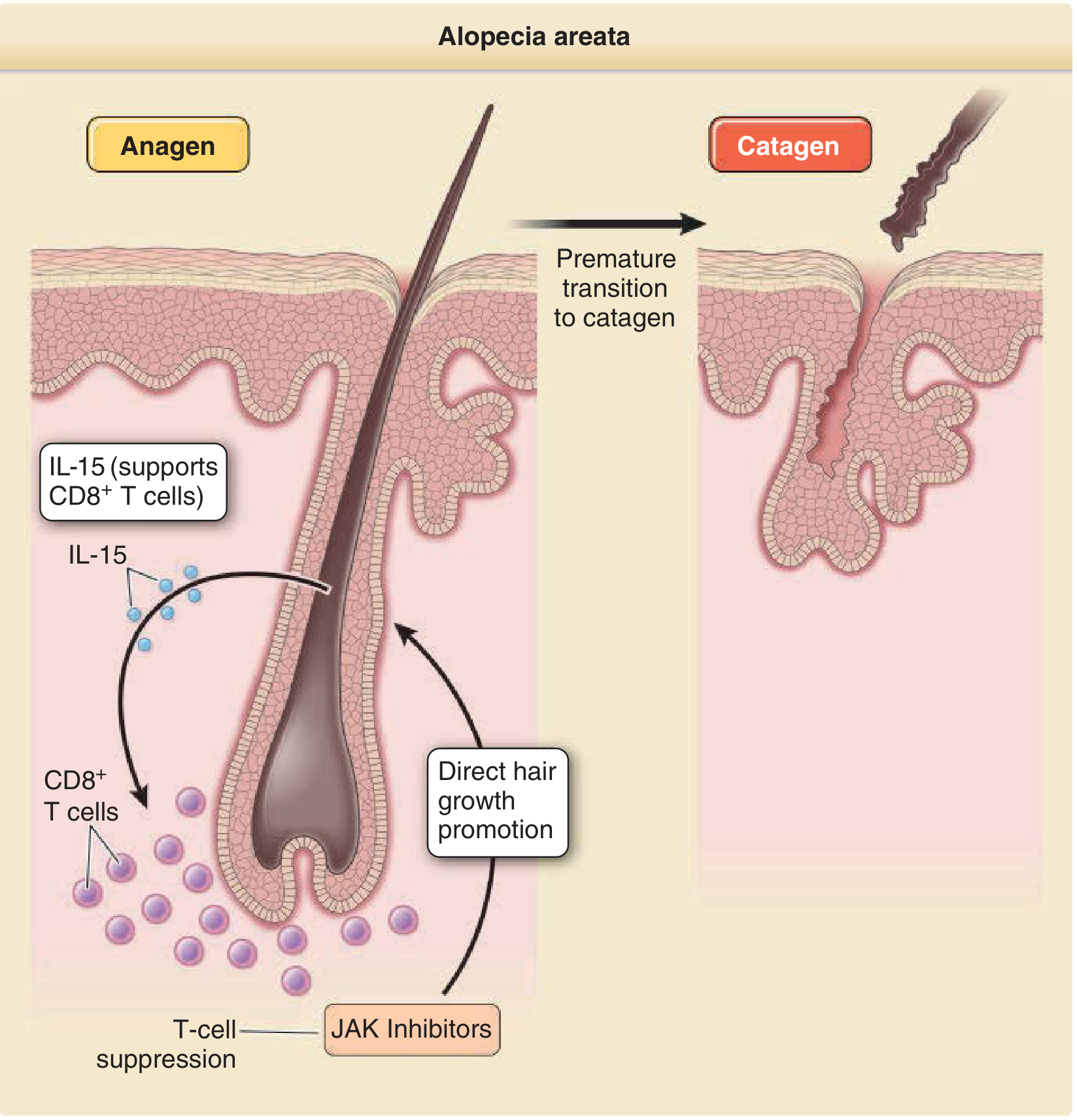
Alopecia areata (AA) results from collapse of the normal immune privilege of the hair follicle. CD8+ NKG2D+ T cells, supported by IL-15 and driven by IFN-γ signaling, attack follicular melanocytes in the anagen bulb, causing premature catagen transition and hair loss. The JAK/STAT pathway is central to this CD8+ T-cell activation, which is why JAK inhibitors are now the primary therapeutic target.
Treatment by Disease Extent
1. Localized / Patchy AA (< 50% scalp involvement)
Intralesional corticosteroids - first-line for cosmetically significant patches
- Triamcinolone acetonide 2.5-10 mg/mL, injected intradermally or in superficial subcutaneous tissue
- Higher concentrations and larger volumes carry greater risk of local atrophy
- Injection under high pressure (small-bore syringe) risks retinal artery embolization
Topical corticosteroids - high-potency (e.g., clobetasol) as a safer first-line alternative, though less reliable than injections
Topical minoxidil - can be used as monotherapy or combined with other treatments
Contact immunotherapy (refractory cases)
- Squaric acid dibutylester (SADBE), diphencyprone (DPCP), dinitrochlorobenzene (DNCB)
- Induces a low-grade allergic contact dermatitis that "distracts" the immune attack on follicles
Short-contact anthralin 1% - applied 15-20 min then washed off; mild benefit
2. Moderate-to-Severe / Rapidly Progressing AA
FDA-Approved JAK Inhibitors (the major advance of the 2020s)
Three oral JAK inhibitors are now FDA-approved for severe AA:
| Drug | Approval | JAK Target | Key Trial | Efficacy (SALT ≤ 20) |
|---|---|---|---|---|
| Baricitinib (Olumiant) | 2022 | JAK1/2 | BRAVE-AA1/AA2 | ~35-40% at week 36; sustained to 5 years |
| Ritlecitinib (Litfulo) | 2023 | JAK3/TEC | ALLEGRO | 32% at week 24; 61% at 2 years; approved age ≥12 |
| Deuruxolitinib (Leqselvi) | 2024 | JAK1/2 | THRIVE-AA1/AA2 | ~41% at week 24; improving through 68 weeks |
Class-wide boxed warning applies to all three: serious infections, malignancy, major adverse cardiovascular events, thrombosis, and mortality - though phase 3 AA trial data have not shown unexpected signals, and absolute event rates are low.
- Baricitinib has the longest safety track record (prior RA/atopic dermatitis approvals)
- Ritlecitinib's JAK3/TEC profile may cause less dyslipidemia than JAK1/2 agents; the only approved option for adolescents
- Deuruxolitinib requires CYP2C19 genotyping before initiation (metabolized by CYP2C19)
Off-label oral/topical JAK inhibitors
- Tofacitinib (JAK1/3) - ~58% achieving ≥50% SALT response off-label
- Ruxolitinib (JAK1/2) - topical formulation showing promise in off-label use (2025 systematic review, PMID 40192197)
3. Alopecia Totalis / Universalis / Ophiasis
These extensive forms are much harder to treat. Historically, response rates are poor with conventional options, but JAK inhibitors have shown meaningful benefit even in totalis/universalis - this is supported by transcriptional profiling showing active (not end-stage) disease in AAT/AAU skin.
Pulsed systemic corticosteroids - e.g., methylprednisolone 500 mg/day x 3 days monthly
-
60% of widespread patchy AA responds; ~50% of totalis, ~25% of universalis
- Ophiasic pattern does NOT respond
- Predictors of response: disease duration ≤ 6 months, onset < 10 years, multifocal pattern
PUVA (psoralen + UVA) - oral or topical methoxalen; option for refractory/widespread disease
Cyclosporine - alone or with PUVA; systemic immunosuppression
Methotrexate - psoriatic doses; some benefit
Sulfasalazine - up to 1.5 g TID; modest benefit
Treatment Algorithm Summary
Localized AA (patches)
└─ Intralesional triamcinolone ± topical steroids ± minoxidil
Moderate-severe / rapidly progressing
└─ Oral JAK inhibitor (baricitinib, ritlecitinib, or deuruxolitinib)
├─ Consider disease duration, comorbidities, age (ritlecitinib ≥12 yr)
└─ Monitor for boxed-warning adverse effects
Refractory / extensive (totalis, universalis)
└─ JAK inhibitor (first choice based on current evidence)
└─ Contact immunotherapy (DPCP/SADBE) if JAK inhibitor unavailable/contraindicated
└─ Pulsed systemic corticosteroids, PUVA, cyclosporine as alternatives
What Does NOT Work Well
- Biologics (TNF inhibitors, IL-17/23 inhibitors): largely disappointing results; AA has paradoxically developed during biologic therapy for other diseases
- Spontaneous remission is common in mild patchy disease (most recover within 1-2 years without treatment), so anecdotal "treatment successes" must be interpreted cautiously
Emerging / Investigational
- Additional JAK inhibitors and selective TYK2 inhibitors in trials
- IL-2 pathway modulators (based on GWAS findings at IL2/IL21 loci)
- 308-nm excimer laser: some reports of regrowth after ~11-12 sessions; evidence limited
Key Recent Evidence
- Cochrane network meta-analysis (PMID 37870096, Oct 2023): JAK inhibitors superior to conventional therapies for moderate-severe AA
- JAK inhibitor systematic review/meta-analysis (PMID 37368402, JAMA Network Open 2023): confirmed efficacy of JAK inhibitors across AA subtypes
- Ritlecitinib vs baricitinib indirect comparison (PMID 39445776, JEADV 2025): both agents effective; cross-trial comparisons suggest broadly similar SALT response rates
- Network meta-analysis of monotherapies (PMID 40231941, 2025): JAK inhibitors rank highest among current options
- Long-term data (EADV 2025): baricitinib shows sustained efficacy to 5 years; ritlecitinib shows 61% SALT ≤20 at 2 years with 84% sustainability among initial responders at 3 years
Sources: Andrews' Diseases of the Skin, p. 868-869; Fitzpatrick's Dermatology Vol. 1-2, p. 229-230; current FDA approvals and 2023-2025 systematic reviews.
patchy loss of hair in young male
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
patchy hair loss young male differential diagnosis alopecia areata tinea trichotillomania
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.