Explain me in detail about pain management and all the conversation factors , as i need to manage my onco patients daily
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cancer pain" AND "pain management"
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Now I have comprehensive information from authoritative textbooks. Let me compile a thorough, clinically useful response.
Oncology Pain Management: A Comprehensive Clinical Guide
Pain is the most feared symptom in cancer patients — affecting up to 70–90% of those with advanced disease. Effective management requires understanding its classification, assessment, pharmacology, and the psychosocial dimensions that modulate it.
1. Classification of Cancer Pain
Understanding the type of pain guides analgesic selection:
| Type | Character | Cause | Preferred Agents |
|---|---|---|---|
| Somatic (bone/soft tissue) | Dull, aching, well-localized | Metastases, post-surgical | NSAIDs, opioids |
| Neuropathic – Type I | Sharp, stabbing, burning, "zinger-like," lancinating | Nerve compression/invasion | Anticonvulsants (gabapentin, carbamazepine, pregabalin) |
| Neuropathic – Type II | Dull, aching, dysesthetic | Peripheral nerve damage | Tricyclic antidepressants (amitriptyline, desipramine) |
| Visceral | Poorly localized, cramping, referred | Organ involvement, capsule stretch | Corticosteroids, opioids |
Over one-third of cancer patients have a neuropathic component — always screen for its character. — Cummings Otolaryngology Head & Neck Surgery
2. Pain Assessment — The Foundation of Management
Always assess before treating. Key dimensions (the "PQRST+"):
- P — Precipitating/Palliating factors (what makes it better/worse?)
- Q — Quality (burning? stabbing? aching?)
- R — Radiation/location
- S — Severity (0–10 NRS or Visual Analogue Scale; pain is the 5th vital sign)
- T — Temporal pattern (constant vs. breakthrough; incident vs. spontaneous)
- Functional impact — sleep, mobility, mood, daily activities
- Psychological/spiritual overlay — anxiety, depression, fear amplify pain threshold
"Pain threshold varies with mood and morale. Given the opportunity to express fears, the patient should experience less pain." — Swanson's Family Medicine Review
Baseline assessment also includes:
- Prior analgesic history and response
- Identifying the anatomic and pathologic diagnosis — never assume all pain is tumor-related (it could be treatment-related, infection, or unrelated comorbidity)
3. The WHO Analgesic Ladder
The World Health Organization's 3-step framework remains the cornerstone of cancer pain management worldwide.
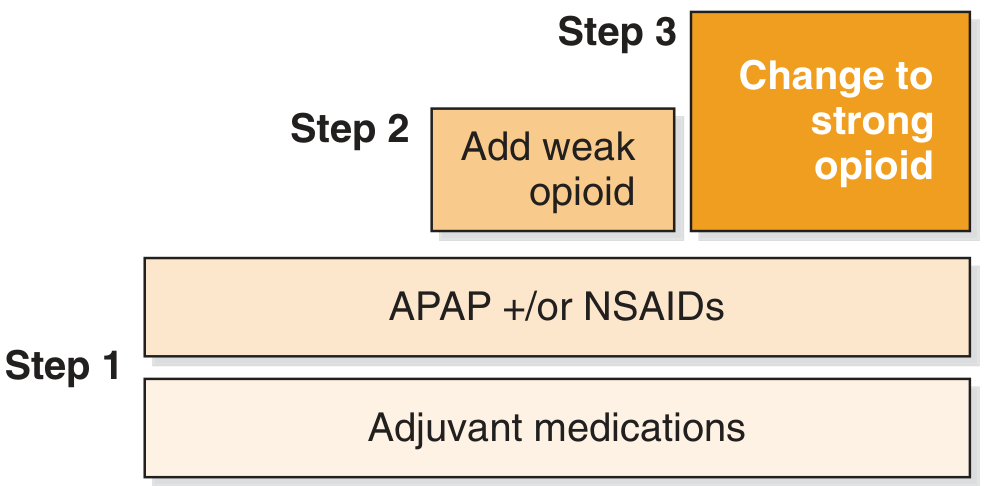
Fig. WHO Analgesic Ladder for Cancer Pain Management (Cummings Otolaryngology)
WHO's 5 Principles of Analgesic Administration
| Principle | Meaning |
|---|---|
| By mouth | Oral route preferred — effective, cheap, adjustable |
| By the clock | Fixed schedule (not PRN) — maintain constant analgesia |
| By the ladder | Match analgesic potency to pain severity |
| For the individual | Titrate to each patient — no standard "right dose" |
| Attention to detail | Continuously reassess efficacy AND side effects |
Never write PRN alone for cancer pain. Gaps in coverage cause return of pain and actually require more total medication compared to around-the-clock dosing. — Swanson's Family Medicine Review
4. Pharmacological Management by Ladder Step
Step 1 — Mild Pain: Non-Opioids
- Acetaminophen (APAP): Safe first-line; max 4 g/day (reduce in hepatic impairment); continue even when opioids are added
- NSAIDs (ibuprofen, naproxen, diclofenac): Especially effective for bone metastases (anti-inflammatory mechanism). Caution in elderly, renal impairment, GI risk, cardiovascular disease
Step 2 — Moderate Pain: Weak Opioids
- Tramadol, codeine (with APAP), hydrocodone
- Note: Codeine is a prodrug — poor metabolizers (CYP2D6) get no analgesia; ultra-rapid metabolizers get toxicity
- Tramadol: serotonin/norepinephrine reuptake inhibition + weak µ-agonist; ceiling effect limits utility in severe pain
Step 3 — Moderate-to-Severe Pain: Strong Opioids
Drug of choice: Morphine sulfate
| Opioid | Route | Notes |
|---|---|---|
| Morphine | PO, SC, IV, PR | Gold standard; active metabolite M6G accumulates in renal failure |
| Hydromorphone | PO, SC, IV | 5× potency of morphine; useful in renal impairment |
| Oxycodone | PO | ~1.5× morphine; less nausea than morphine in some |
| Fentanyl | Transdermal, buccal, IV | Transdermal patch: 72-hr release; analgesic persists 16–24h after removal; best for stable pain |
| Methadone | PO, IV | NMDA antagonist; excellent for neuropathic pain; long/unpredictable half-life — specialist use |
| Buprenorphine | Transdermal, SL | Partial agonist; ceiling on respiratory depression |
Do NOT use meperidine (pethidine) for chronic cancer pain — active metabolite normeperidine accumulates and causes CNS toxicity (seizures). — Swanson's
5. Initiating Opioid Therapy: Practical Steps
- Start with short-acting oral morphine (5–10 mg q4h); daily starting dose 30–60 mg/day
- After 1 week of stable dosing → convert to long-acting morphine (same total daily dose) + keep short-acting for breakthrough
- Breakthrough dose = 10–15% of the total 24-hour opioid dose, available q1–2h PRN
- If breakthrough doses are needed ≥3×/day → uptitrate the basal long-acting dose
- Titrate to effect — there is no ceiling dose for pure agonists in cancer pain
Converting Opioids (Rotation)
When switching opioids (inadequate analgesia, intolerable side effects):
- Calculate the equianalgesic dose of the new drug
- Start at ≤75–80% of the equianalgesic dose (incomplete cross-tolerance; different receptor profiles)
- Titrate from there
When dose requirements escalate rapidly (e.g., 3× the previous dose in 1 week), this most likely reflects tumor progression rather than tolerance. Reassess the anatomic cause. — Swanson's
6. Adjuvant (Co-analgesic) Drugs
These enhance opioid efficacy, treat neuropathic components, or address co-symptoms:
Anticonvulsants (for neuropathic Type I — shooting, burning pain)
- Gabapentin: Start 100–300 mg TID → titrate to 900–3600 mg/day; renal dose adjustment needed; SE: sedation, dizziness, peripheral edema
- Pregabalin: Similar mechanism, faster titration; better bioavailability
- Carbamazepine / Oxcarbazepine: Second-line for lancinating pain (e.g., trigeminal distribution)
Tricyclic Antidepressants (for neuropathic Type II — dull aching pain)
- Amitriptyline / Nortriptyline / Desipramine: Lower doses for pain than depression; once-nightly dosing capitalizes on sedative effect to improve sleep; QTc monitoring required; avoid in elderly/cardiac patients
SNRIs
- Duloxetine: Growing evidence in chemotherapy-induced peripheral neuropathy (CIPN); well tolerated
Corticosteroids (for visceral/bone/cerebral edema pain)
- Dexamethasone 4–8 mg/day: Reduces perineural/perivascular edema; boosts appetite; mood elevation; useful for visceral capsule pain, spinal cord compression, raised ICP
Bisphosphonates / Denosumab
- Zoledronic acid / Denosumab: For bone metastases — reduce skeletal-related events and bone pain; not immediate analgesics but reduce long-term bone pain burden
Ketamine (NMDA antagonist)
- Sub-anesthetic doses reduce opioid-refractory pain and opioid tolerance; typically specialist-initiated
7. Routes of Administration
| Route | When to Use |
|---|---|
| Oral | First choice — most patients; effective, cheap |
| Transdermal | Stable pain; unable to swallow; fentanyl patch |
| Sublingual/Buccal | Dysphagia; rapid breakthrough (fentanyl lollipop/buccal film) |
| Rectal | Cannot swallow; morphine, oxymorphone, hydromorphone suppositories |
| Subcutaneous infusion | Nausea/vomiting; bowel obstruction; end-of-life syringe driver |
| IV/PCA | Rapid titration; hospitalized patients |
| Epidural/Intrathecal | Refractory pain; opioid-sparing; specialist-placed pumps |
| Topical morphine gel | Malignant ulcers/wounds |
8. Managing Opioid Side Effects
Always start prophylactic bowel regimen when starting opioids — constipation does NOT resolve with tolerance.
| Side Effect | Management |
|---|---|
| Constipation | Stimulant laxative (senna 2–8 tabs BD) + stool softener (docusate); osmotic agents (lactulose 15–30 mL q4–8h); methylnaltrexone for refractory opioid-induced constipation |
| Nausea/Vomiting | Metoclopramide, prochlorperazine, ondansetron; usually resolves in 1–2 weeks; switch opioid if persistent |
| Sedation | Usually transient; reduce dose; methylphenidate for persistent sedation |
| Respiratory depression | Rare at analgesic doses; treat with naloxone 0.04 mg IV titrated slowly |
| Pruritus | Antihistamines; opioid rotation |
| Urinary retention | Catheterization; opioid rotation |
| Delirium | Consider opioid-induced hyperalgesia; rotate opioid; haloperidol for delirium |
If nausea is refractory on triple antiemetic therapy, switch to a different opioid rather than adding a 4th antiemetic. — Swanson's
9. Conversational / Psychosocial Factors in Oncology Pain
These are the most commonly underestimated components:
Psychological Factors
- Anxiety and fear lower the pain threshold significantly — address fear of death, treatment, and disability directly
- Depression: Co-exists in >25% of cancer patients; TCAs/SNRIs serve dual analgesic + antidepressant purpose
- Catastrophizing: Amplifies pain perception — cognitive behavioral therapy (CBT) restructures maladaptive pain cognitions
- "Total Pain" (Dame Cicely Saunders): Pain has physical, psychological, social, and spiritual dimensions — all must be addressed
Communication Strategies
- Use open-ended questions: "Tell me about your pain — what does it feel like?"
- Normalize reporting: "Many patients with your condition experience pain — it's important you tell me so I can treat it"
- Address opiophobia (patient and family): Clarify that opioids for cancer pain ≠ addiction; respiratory depression is rare at analgesic doses
- Discuss goals of pain control: Complete relief vs. functional improvement vs. acceptable level
Social Factors
- Caregiver burden and family dynamics affect pain reporting and adherence
- Financial stress (drug costs) → medication non-adherence → poor pain control
- Isolation and loneliness worsen pain — family support programs reduce total opioid requirement
Spiritual/Existential Factors
- Fear of death, loss of meaning, unfinished business amplify the pain experience
- Chaplaincy services, psycho-oncology referrals, and dignity therapy address these dimensions
10. Special Oncology Pain Situations
Bone Pain (Most Common)
- NSAIDs + opioids are synergistic
- Local radiotherapy is first choice for focal bone metastases (e.g., single vertebral level) — effective, reduces opioid requirement
- Bisphosphonates for diffuse skeletal disease
- Strontium-89 / Radium-223 for widespread blastic bone disease
Neuropathic Chemotherapy-Induced Peripheral Neuropathy (CIPN)
- Duloxetine has best evidence (Level A)
- Gabapentin/pregabalin for burning dysesthesias
- Topical treatments (lidocaine gel, capsaicin) for focal areas
Spinal Cord Compression (Oncological Emergency)
- High-dose dexamethasone immediately (16 mg/day)
- Urgent radiotherapy or surgical decompression
- Do not delay pain treatment while awaiting imaging
End-of-Life / Refractory Pain
- Palliative sedation for intractable, refractory suffering
- Continuous subcutaneous opioid infusion (syringe driver)
- Intrathecal drug delivery systems for those requiring high doses
11. The "Ten Commandments" of Cancer Pain Management
(Swanson's Family Medicine Review)
- Do not assume all pain is tumor-related — make a specific anatomic/pathologic diagnosis
- Consider the patient's feelings — emotional expression reduces pain threshold
- Never use PRN alone — around-the-clock dosing prevents pain recurrence
- Prescribe adequate doses — the right dose is what relieves pain, not what a textbook says
- Try non-narcotics first for mild–moderate pain, unless clearly severe
- Do not be afraid of opioids — when non-narcotics fail, escalate promptly
- Use non-drug therapies: hypnosis, imagery, biofeedback, physiotherapy, CBT
- Seek colleagues' advice when your interventions are insufficient
- Support the entire family — treat anticipatory grief; prevent isolation
- Maintain quiet confidence and cautious optimism — set small achievable goals to build trust
12. Multidisciplinary Team Approach
Optimal oncology pain management involves:
| Specialist | Role |
|---|---|
| Oncologist | Disease-directed therapy (chemo, radio, surgery) that reduces tumor burden |
| Palliative care physician | Symptom management, goals of care |
| Pain specialist / Anesthesiologist | Interventional procedures, opioid rotation |
| Pharmacist | Dosing, interactions, compounding |
| Psycho-oncologist / Psychiatrist | Depression, anxiety, CBT |
| Social worker | Financial support, family coping, discharge planning |
| Physiotherapist | Deconditioning, TENS, mobility |
| Chaplain/Spiritual care | Existential suffering |
| Nursing | Daily assessment, medication adherence, education |
Summary: Daily Clinical Checklist for Oncology Pain
✅ Assess pain score at every visit (0–10 NRS)
✅ Characterize type (somatic/neuropathic/visceral) — different drugs for different types
✅ Check breakthrough analgesic use — if >3 doses/day, uptitrate basal opioid
✅ Ask about functional impact: sleep, mobility, mood
✅ Screen for opioid side effects: constipation, nausea, sedation
✅ Reassess psychological and spiritual distress
✅ Review bowel regimen — every patient on opioids needs one
✅ Ask about adherence and access to medications
✅ Consider if disease-directed therapy could reduce pain burden
✅ Involve family in the conversation
Key References:
- Cummings Otolaryngology Head and Neck Surgery — Medication Management, Chapter 14
- Swanson's Family Medicine Review — Chapter 66, Cancer Pain Management
- Harrison's Principles of Internal Medicine 22E — Chapter 13, Palliative Care
- Recent meta-analysis: Imkamp et al., J Pain Symptom Manage 2024 — network meta-analysis questioning opioid-first approaches in cancer pain management highlights the growing role of multimodal strategies (PMID: 38838946)
Soo, tremadol total dose is 400mg per day right? But if we add paracetamol we have to calculate combined dose. How to calculate combined dose and what is the max combined dose
Finding Sources
Searching the Web
tramadol paracetamol combination maximum daily dose calculation 37.5mg 325mg
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the information needed. Here's a clear, clinically practical answer:
Tramadol + Paracetamol: Dose Calculation & Maximum Combined Dose
First, the Individual Drug Limits
| Drug | Max Daily Dose |
|---|---|
| Tramadol | 400 mg/day (ceiling dose — beyond this, no extra analgesia, only more toxicity: seizures, serotonin syndrome) |
| Paracetamol (Acetaminophen) | 4000 mg/day under medical supervision; 3000–3250 mg/day OTC/general use; ≤2000 mg/day in frail/elderly/liver-risk patients |
— Goldman-Cecil Medicine; Katzung's Basic & Clinical Pharmacology 16e
The Fixed-Dose Combination (FDC) Tablets
The most commonly available formulations are:
| Formulation | Tramadol per tab | Paracetamol per tab |
|---|---|---|
| Ultracet / Tramacet | 37.5 mg | 325 mg |
| Tramazac-P (generic) | 37.5 mg | 325 mg |
| Some regional brands | 50 mg | 325 mg |
| Some regional brands | 50 mg | 500 mg |
How to Calculate the Combined Maximum Dose
The limiting factor is whichever drug hits its ceiling first. You calculate both, then stop at the lower number.
Formula:
Max tablets/day = Lower of (Max tramadol dose ÷ tramadol per tab) OR (Max paracetamol dose ÷ paracetamol per tab)
Example 1: Tramadol 37.5 mg + Paracetamol 325 mg (Ultracet)
| Calculation | Tablets | |
|---|---|---|
| Tramadol limit: 400 ÷ 37.5 | = 10.6 | → max 10 tabs |
| Paracetamol limit: 4000 ÷ 325 | = 12.3 | → max 12 tabs |
→ Limiting drug = Tramadol
Maximum = 8 tablets/day (commonly recommended; giving 300 mg tramadol + 2600 mg paracetamol — keeps a safety buffer)
Absolute maximum = 10 tablets/day (375 mg tramadol + 3250 mg paracetamol)
Standard dosing: 2 tablets every 6 hours = 8 tabs/day = 300 mg tramadol + 2600 mg paracetamol
Example 2: Tramadol 50 mg + Paracetamol 325 mg
| Calculation | Tablets | |
|---|---|---|
| Tramadol limit: 400 ÷ 50 | = 8 tabs | → max 8 tabs |
| Paracetamol limit: 4000 ÷ 325 | = 12.3 tabs | → max 12 tabs |
→ Limiting drug = Tramadol
Maximum = 8 tablets/day = 400 mg tramadol + 2600 mg paracetamol
Standard dose: 1–2 tabs every 6–8 hours
Example 3: Tramadol 50 mg + Paracetamol 500 mg
| Calculation | Tablets | |
|---|---|---|
| Tramadol limit: 400 ÷ 50 | = 8 tabs | → max 8 tabs |
| Paracetamol limit: 4000 ÷ 500 | = 8 tabs | → max 8 tabs |
→ Both hit ceiling at 8 tabs simultaneously
Maximum = 8 tablets/day = 400 mg tramadol + 4000 mg paracetamol
Critical Point: When Paracetamol Becomes the Limiting Drug
If your patient is taking additional paracetamol from other sources (common in oncology — cold remedies, other combination tablets, syrups), you must account for total daily paracetamol from ALL sources.
Total paracetamol = (tabs × paracetamol per tab) + any standalone paracetamol
This must stay under 4000 mg/day (or 2000 mg/day in liver disease, alcoholism, malnutrition, elderly)
Special Considerations in Oncology Patients
| Situation | Adjustment |
|---|---|
| Hepatic metastases / liver impairment | Reduce paracetamol to 2000 mg/day max; some guidelines say avoid entirely in Child-Pugh C |
| Elderly (>65 years) | Cap paracetamol at 2000–3000 mg/day |
| Renal impairment (CrCl <30 mL/min) | Tramadol: increase dosing interval to q12h; max 200 mg/day |
| Seizure history / epilepsy | Tramadol lowers seizure threshold — use with extreme caution |
| On SSRIs/SNRIs/TCAs | Tramadol + serotonergic drugs → Serotonin syndrome risk — serious in onco patients on antidepressants |
| On MAO inhibitors | Absolute contraindication |
Quick Reference Card
Most common FDC: Tramadol 37.5 mg + Paracetamol 325 mg
Standard dose: 2 tabs × 4 times daily = 8 tabs/day
→ Tramadol: 300 mg/day ✓ (safe, under 400 mg ceiling)
→ Paracetamol: 2600 mg/day ✓ (well under 4000 mg ceiling)
Absolute max: 10 tabs/day (limited by tramadol)
→ Tramadol: 375 mg/day
→ Paracetamol: 3250 mg/day
Bottom line: In the standard 37.5/325 FDC, tramadol is always the limiting drug — you hit its 400 mg ceiling before paracetamol reaches its 4000 mg ceiling. The practical safe ceiling is 8 tablets/day (2 tabs QID). Always check for hidden paracetamol in other concurrent medications your oncology patients are receiving.
Soo, tremadol total dose is 400mg per day right? But if we add paracetamol we have to calculate combined dose. How to calculate combined dose and what is the max combined dose
This was answered in full just above — no need to re-research. Here's the complete answer again:
Tramadol + Paracetamol: Combined Dose Calculation
Individual Drug Ceilings First
| Drug | Max Daily Dose |
|---|---|
| Tramadol | 400 mg/day (hard ceiling — beyond this: seizures, serotonin syndrome, no added analgesia) |
| Paracetamol | 4000 mg/day under medical supervision; 2000 mg/day in elderly, liver disease, malnutrition |
The Core Principle
The limiting drug = whichever hits its ceiling first. Calculate both limits → stop at the lower number.
Formula:
Max tabs/day = Lower of:
- Max tramadol dose ÷ tramadol per tablet
- Max paracetamol dose ÷ paracetamol per tablet
Worked Out for Each Common Formulation
Formulation 1: Tramadol 37.5 mg + Paracetamol 325 mg (Ultracet / Tramacet — most common)
| Drug | Max dose ÷ per-tab dose | = Max tabs |
|---|---|---|
| Tramadol | 400 ÷ 37.5 | = 10.6 → 10 tabs |
| Paracetamol | 4000 ÷ 325 | = 12.3 → 12 tabs |
Limiting drug = Tramadol
| Dosing | Tabs/day | Tramadol | Paracetamol |
|---|---|---|---|
| Standard (2 tabs QID) | 8 tabs | 300 mg ✅ | 2600 mg ✅ |
| Absolute maximum | 10 tabs | 375 mg ✅ | 3250 mg ✅ |
Practical recommendation: 2 tabs every 6 hours = 8 tabs/day — keeps a safety buffer on tramadol and well under paracetamol ceiling.
Formulation 2: Tramadol 50 mg + Paracetamol 325 mg
| Drug | Calculation | Max tabs |
|---|---|---|
| Tramadol | 400 ÷ 50 | = 8 tabs |
| Paracetamol | 4000 ÷ 325 | = 12 tabs |
Maximum = 8 tabs/day = 400 mg tramadol + 2600 mg paracetamol
Formulation 3: Tramadol 50 mg + Paracetamol 500 mg
| Drug | Calculation | Max tabs |
|---|---|---|
| Tramadol | 400 ÷ 50 | = 8 tabs |
| Paracetamol | 4000 ÷ 500 | = 8 tabs |
Maximum = 8 tabs/day = 400 mg tramadol + 4000 mg paracetamol
(Both ceilings hit simultaneously — no room for extra standalone paracetamol)
Watch Out: Hidden Paracetamol Sources
In oncology patients, always audit ALL concurrent medications for paracetamol content — cough syrups, cold tablets, antipyretics, other combination analgesics.
Total paracetamol = FDC tabs × 325/500 mg + any standalone paracetamol ≤ 4000 mg/day
Dose Reduction in Special Populations
| Patient | Adjust to |
|---|---|
| Hepatic metastases / liver impairment | Paracetamol ≤ 2000 mg/day (or avoid in Child-Pugh C) |
| Elderly >65 years | Paracetamol ≤ 2000–3000 mg/day |
| Renal impairment (CrCl <30 mL/min) | Tramadol: extend interval to q12h, max 200 mg/day |
| Epilepsy | Tramadol lowers seizure threshold — use with caution |
| On SSRIs / TCAs / SNRIs | Risk of serotonin syndrome — very relevant in onco patients |
Quick Summary
Standard FDC (37.5/325):
Safe daily max → 8 tablets (300 mg tramadol + 2600 mg paracetamol)
Absolute max → 10 tablets (375 mg tramadol + 3250 mg paracetamol)
Rule of thumb: Tramadol is ALWAYS the limiting drug in 37.5/325 and 50/325 FDCs.
Paracetamol only becomes limiting if the patient is also taking paracetamol from other sources.
This is a shared conversation. Sign in to Orris to start your own chat.