Tuberculosis epidemiology
Reading File
Finding Sources
Searching PubMed
"tuberculosis"[MeSH Terms] AND "epidemiology"[MeSH Terms]
Searching the Web
tuberculosis global epidemiology 2025 WHO report incidence prevalence
Reading File
Finding Sources
Searching PubMed
"tuberculosis" AND "global burden" AND "incidence"
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have rich material from multiple textbook sources. Let me compile the comprehensive answer.
Tuberculosis Epidemiology
Global Burden
Tuberculosis (TB) remains one of the most significant infectious disease burdens in the world. An estimated 1.7 billion people (roughly one-quarter of the global population) are infected with Mycobacterium tuberculosis, though the distribution is highly heterogeneous.
In 2018, there were approximately 10 million new TB cases globally. Of these, only 7.0 million were reported to national public health authorities, leaving an estimated 3 million unaccounted for - a major surveillance gap. In the same year, TB caused 1.2 million deaths, with a case fatality rate of approximately 15%. Despite a 9% decline in deaths between 2017 and 2018, the number of new cases did not decline, indicating insufficient progress toward global targets.
Source: Murray & Nadel's Textbook of Respiratory Medicine
Geographic Distribution
TB is not evenly distributed. In 2018, 86% of all cases were identified in three WHO regions:
| Region | Share of Cases | Incidence (per 100,000) |
|---|---|---|
| Southeast Asia | 44% | 220 |
| Africa | 24% | 231 |
| Western Pacific | 18% | 96 |
Most high-income countries have incidence rates below 10 per 100,000, where TB elimination is considered an achievable goal.
India bears the greatest single-country burden, accounting for 26% of global incident TB cases in 2019, with an estimated 2.64 million incident cases (rate: 193 per 100,000 population). Almost half of all rifampin-resistant/MDR-TB cases arose from just three countries: India (24%), China (13%), and Russia (10%).
Source: Park's Textbook of Preventive and Social Medicine; Murray & Nadel's Textbook of Respiratory Medicine
Age and Sex Distribution
In India and most high-burden countries, TB predominantly affects adolescents and young adults (15-30 years), indicating ongoing active transmission. In some southern Indian states (Kerala, Karnataka, Tamil Nadu, Andhra Pradesh), TB skews toward an older age group (50+ years), reflecting a different epidemiological pattern driven more by reactivation of latent infection.
Globally, about 1 million paediatric TB cases occur every year, with more than 100,000 deaths. Most childhood TB deaths result from meningitis or disseminated disease.
Transmission Dynamics
TB is an airborne infection. Infection is acquired by inhalation of M. tuberculosis in droplet nuclei (1-5 μm in diameter) that reach the alveoli and can remain suspended in air for several hours.
The determinants of transmission differ by setting:
- High-burden settings: Ongoing transmission with rapid progression (within 1-2 years) is the driving force
- Low-burden settings: TB more commonly results from reactivation of latent infection acquired earlier
Key factors determining infectiousness of a source case:
- Severity of coughing (aerosol generation)
- Bacillary load (bacillary population)
- Anti-tuberculosis therapy status (treated patients become non-infectious rapidly)
- Strain of M. tuberculosis
Major Risk Factors and Co-morbidities
HIV Co-infection
People living with HIV (PLHIV) are 20-30 times more likely to develop TB than HIV-negative individuals. In 2018, 8.6% of all TB cases had HIV co-infection. TB causes 1 in 3 HIV deaths. The burden is concentrated in Africa, where 70% of the 37 million PLHIV reside.
Diabetes Mellitus
Diabetes triples the risk for TB and worsens treatment outcomes. The prevalence of diabetes among TB patients worldwide is approximately 15.3% (range: 0.1% in Latvia to 45.2% in Marshall Islands). With diabetes projected to rise from 425 million (2017) to 629 million by 2045, predominantly in Africa and Asia, achieving global TB targets becomes increasingly difficult.
Poverty
Poverty is a powerful TB determinant. Crowded and poorly ventilated living conditions, malnutrition, and lack of health empowerment - all poverty-associated factors - drive transmission and disease.
Other Risk Factors
- Malnutrition and undernutrition
- Tobacco and alcohol use
- Indoor air pollution
- Overcrowding
- Increased human migration (mixing infected with uninfected communities)
Drug-Resistant TB
Drug-resistant TB is a major threat to global control:
- MDR-TB: Resistance to at least isoniazid and rifampin
- XDR-TB: MDR-TB plus resistance to at least one fluoroquinolone and one injectable second-line agent
In 2018, an estimated 500,000 people developed TB resistant to rifampicin, of whom 78% had MDR-TB. XDR-TB, first reported in 2006, had been documented in 131 WHO member states by end of 2018. Treatment outcomes for MDR-TB are far worse than drug-susceptible TB: cure rates of 56% vs. 85%, respectively.
Mathematical modeling predicts increasing drug resistance driven by transmission of resistant strains (rather than acquisition during treatment), reaching 32.5% among incident cases in Russia, 12.4% in India, 8.9% in the Philippines, and 4.7% in South Africa.
TB in the United States
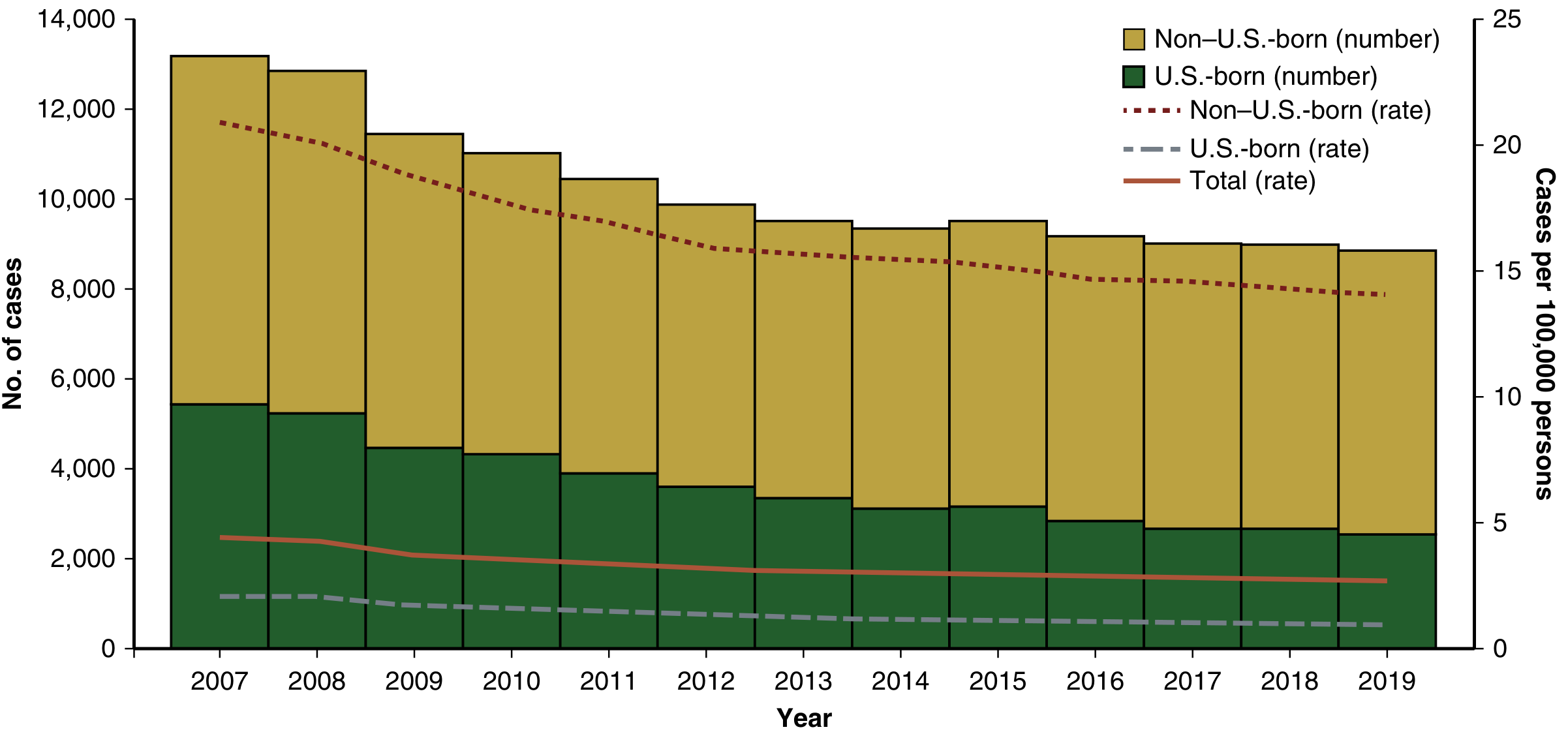
Figure: TB case counts and rates by U.S.-born vs. non-U.S.-born persons, 2007-2019 (Source: Murray & Nadel's Textbook of Respiratory Medicine)
In the United States, TB incidence declined dramatically following the introduction of effective chemotherapy, but progress has slowed to ~1.5% per year. In 2019, 8,920 cases (2.7 per 100,000) were reported - the lowest number since systematic national reporting began in 1953. Critically, 71% of cases were among non-U.S.-born persons. From 1993 to 2019, the overall incidence fell 71%, but the reduction was disproportionate: 86% among U.S.-born vs. only 57% among non-U.S.-born persons.
Global Control Strategies
| Strategy | Period | Focus |
|---|---|---|
| DOTS | Mid-1990s - 2005 | Directly Observed Treatment, Short-course |
| Stop TB Strategy | 2006-2015 | Five key indicators: detection, treatment success, incidence, prevalence, death |
| End TB Strategy | 2015-2030 | 90% reduction in deaths, 80% reduction in incidence vs. 2015 baseline; SDG alignment |
| WHO 2035 Target | - | 95% reduction in deaths, 90% reduction in incidence |
The 2018 UN General Assembly high-level meeting on TB set new global commitments:
- Treat 40 million people (including 3.5 million children and 1.5 million with drug-resistant TB) by 2022
- Provide TB preventive treatment to 30 million (including 6 million PLHIV and 4 million children under 5)
- Mobilize at least $13 billion/year for universal TB prevention, diagnosis, and treatment
- Allocate at least $2 billion/year for TB research
The COVID-19 pandemic threatened to reverse recent progress, with estimates suggesting global TB deaths could increase by 0.2-0.4 million in 2020 alone if health services were disrupted.
Sources:
- Murray & Nadel's Textbook of Respiratory Medicine - Chapter 51: Tuberculosis Epidemiology & Transmission
- Park's Textbook of Preventive and Social Medicine - TB Epidemiology in India; End TB Strategy
This is a shared conversation. Sign in to Orris to start your own chat.