Give me detail notes on Neonatal seizures from basics to advance in easy language which covers every aspects of this topic from standard books for MBBS student
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive, rich content from the textbooks along with key diagrams. Let me now compile the detailed, well-structured notes.
Neonatal Seizures - Complete Notes for MBBS Students
Sources: Bradley and Daroff's Neurology in Clinical Practice, Adams and Victor's Principles of Neurology (12th Ed.), Tintinalli's Emergency Medicine, Rosen's Emergency Medicine
1. DEFINITION
A neonatal seizure is a paroxysmal alteration in any neurological function (motor, behavioral, or autonomic) that is accompanied by abnormal, synchronous electrical discharge on EEG, occurring in an infant within the first 28 days of life (or up to 44 weeks post-conceptional age in preterm infants).
Key features:
- Seizures in newborns are almost always acute symptomatic (caused by an underlying brain injury or metabolic problem) - unlike adults, where unprovoked/idiopathic epilepsy is common.
- They are more common in the first 28 days of life than at any other period.
- They represent one of the most common manifestations of neonatal brain injury.
- Many neonatal seizures are electrographic only (no visible clinical signs) - detected only on EEG.
Bradley and Daroff's Neurology in Clinical Practice, p. 2854
2. INCIDENCE
- Approximately 1-5 per 1000 live births in term neonates.
- Higher in preterm infants.
- More common in males.
3. WHY ARE NEONATAL SEIZURES SPECIAL? (Pathophysiology)
This is the core reason why neonatal seizures are unique and difficult to treat.
3a. GABA paradox (the key concept)
In adult neurons, GABA (the main inhibitory neurotransmitter) activates GABA-A receptors → chloride flows INTO the cell → membrane becomes more negative (hyperpolarization) → INHIBITION (no seizure).
In immature/neonatal neurons, there is a net chloride EFFLUX when GABA-A receptors are activated → membrane becomes more positive (depolarization) → EXCITATION (promotes seizures!).
Why? Two key chloride transporters control intracellular chloride:
- NKCC1 - pumps chloride INTO the cell (dominant in neonates = high intracellular Cl⁻)
- KCC2 - pumps chloride OUT of the cell (becomes dominant with maturation)
In neonates, NKCC1 dominates → high intracellular Cl⁻ → GABA opens Cl⁻ channels → Cl⁻ flows OUT → depolarization → GABA is EXCITATORY in neonates.
Clinical implication:
This explains why phenobarbital and benzodiazepines (GABA agonists) often work poorly in neonates - they are trying to use a system that is developmentally inverted.
Bradley and Daroff's Neurology in Clinical Practice, p. 2855
3b. Other factors promoting neonatal seizures:
- Immature synaptic connections → seizures remain focal (no generalized tonic-clonic)
- Incomplete myelination → poor bihemispheric spread
- Higher ratio of excitatory (NMDA, AMPA) to inhibitory receptors
- Energy metabolism vulnerability
3c. Why seizures are harmful:
Prolonged seizures cause neuronal injury via:
- Disturbances in cerebral energy metabolism
- Depletion of ATP and energy stores
- Excitotoxicity (glutamate overactivation)
- This informs why even subclinical (EEG-only) seizures must be treated aggressively.
4. ETIOLOGY (Causes) - By Day of Onset
The timing of seizure onset strongly suggests the underlying cause:
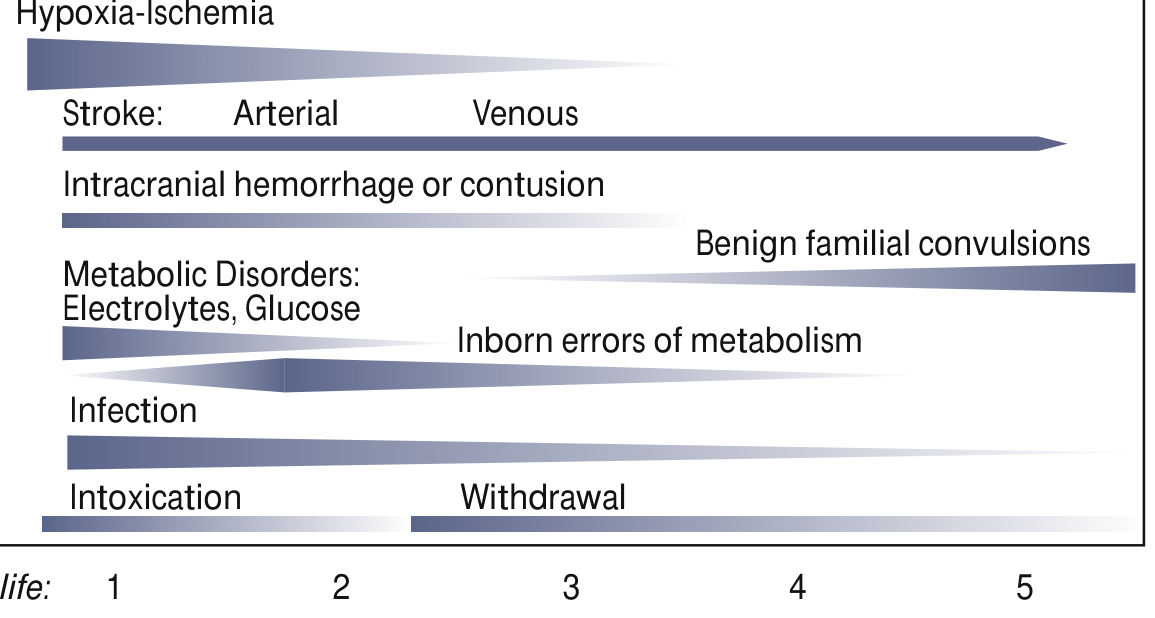
Day 1 (Birth to 24 hours) - Most serious
| Cause | Notes |
|---|---|
| Hypoxic-Ischemic Encephalopathy (HIE) | #1 cause (~50% of term seizures); perinatal asphyxia |
| Intracranial hemorrhage | Subdural, subarachnoid, IVH (especially preterm) |
| Direct drug toxicity | Local anesthetic injection (lidocaine) |
| Hypoglycemia | Especially in SGA, IDM (infant of diabetic mother) |
Day 1-3
| Cause | Notes |
|---|---|
| HIE (continues to predominate) | |
| Intracranial hemorrhage | |
| Hypoglycemia | Most common metabolic cause |
| Hypocalcemia (early) | Associated with prematurity, IDM, asphyxia |
| Pyridoxine deficiency | Rare but important treatable cause |
Day 3-7
| Cause | Notes |
|---|---|
| Meningitis / Sepsis | Group B Streptococcus, E. coli, Listeria, Herpes |
| Hypocalcemia (late) | Hyperphosphatemia (cow's milk feeds), hypomagnesemia |
| Inborn errors of metabolism | Maple syrup urine disease, non-ketotic hyperglycinemia |
| Benign neonatal seizures ("5th day fits") | Onset days 4-6, self-limiting |
| Drug withdrawal | Neonatal abstinence syndrome (opioids) |
After Day 7
| Cause | Notes |
|---|---|
| Herpes encephalitis | Can present up to weeks 2-3 |
| Inborn errors of metabolism | PKU, organic acidemias |
| Benign familial neonatal epilepsy | KCNQ2/KCNQ3 gene mutations, good prognosis |
| Cerebral dysplasia | Cortical malformations |
| Kernicterus | Rare |
Summary mnemonic: "HI BEACH SWIM"
- HIE (hypoxic-ischemic encephalopathy)
- Infection (meningitis, herpes)
- Blood - intracranial hemorrhage
- Electrolytes (hypoCa, hypoNa, hypoMg)
- Antenatal drug exposure / withdrawal
- Cerebral malformation (dysplasia)
- Hypoglycemia
- Syndrome (genetic epilepsy - KCNQ2)
- Withdrawal (opioid, barbiturate)
- Inborn errors of metabolism
- Meningitis
Adams and Victor's Principles of Neurology, p. 352; Bradley and Daroff's, p. 2856
5. CLASSIFICATION OF NEONATAL SEIZURES (Volpe Classification)
Because the neonatal brain is immature, seizures are fragmented and focal - not the dramatic generalized convulsions seen in adults. Volpe classified them into 4 clinical types:
| Clinical Type | Manifestations | EEG Correlation | Notes |
|---|---|---|---|
| Subtle (most common, ~50%) | Eye deviation/blinking/fixed stare; lip smacking, chewing, tongue protrusions; apnea; bicycling of legs; swimming arm movements | Variable - may or may not have EEG correlate | Most common in both term and preterm; often missed |
| Clonic - Focal | Rhythmic, slow jerking of one limb or face (1-3 Hz) | Usually has EEG correlate | Suggests focal pathology (e.g., cerebral infarct) |
| Clonic - Multifocal | Clonic movements migrating randomly across body | Usually has EEG correlate | |
| Tonic - Focal | Sustained extension/flexion of one limb | May have EEG correlate | |
| Tonic - Generalized | Decorticate or decerebrate posturing | Usually NO EEG correlate - brainstem release phenomenon | Not a "true" seizure in EEG sense |
| Myoclonic - Focal/Multifocal | Rapid single or multiple jerks of a limb | Variable | |
| Myoclonic - Generalized | Rapid synchronous flexion jerks of entire body | Usually has EEG correlate | Ominous prognosis |
Key clinical facts:
- Subtle seizures are most common and most difficult to detect.
- Generalized tonic-clonic seizures do NOT occur in neonates due to immature synaptic connections and incomplete myelination.
- Focal clonic seizures most commonly = focal cerebral infarction.
- Generalized tonic = usually NOT a true seizure, represents brainstem release.
- Generalized myoclonic = ominous sign (early myoclonic encephalopathy).
Bradley and Daroff's Neurology in Clinical Practice, p. 2857 (Table 110.1)
6. DIFFERENTIAL DIAGNOSIS - What Mimics Seizures?
The hardest part is distinguishing seizures from normal neonatal movements.
Jitteriness vs. Clonic Seizures
| Feature | Jitteriness | Clonic Seizures |
|---|---|---|
| Stimulus sensitivity | YES - provoked by stimuli | NO |
| Suppressed by holding | YES - stops with passive flexion | NO |
| Eye movement | NO | YES (deviation/blinking) |
| Autonomic changes | NO | YES (tachycardia, apnea) |
| Movement type | Tremor - equal amplitude both ways | Fast and SLOW components |
| EEG | Normal | Abnormal seizure discharge |
Other mimics:
- Physiological myoclonus - evoked by stimuli (touch/sound), occurs in healthy newborns, no encephalopathy
- Hyperekplexia (startle disease) - exaggerated startle to auditory/visual/touch stimuli; due to glycine neurotransmission gene mutations; non-epileptic
- Normal newborn movements - stretching, yawning, random limb movements
Bradley and Daroff's Neurology in Clinical Practice, p. 2857
7. DIAGNOSIS
7a. EEG - The Gold Standard
- Continuous conventional EEG is the gold standard (American Clinical Neurophysiology Society recommendation).
- aEEG (amplitude-integrated EEG) is a simplified single/two-channel bedside monitor; less sensitive but easier to interpret at the bedside.
EEG criteria for a neonatal seizure:
- Sudden electrographic change
- Repetitive waveforms evolving in morphology, frequency, and/or location
- Amplitude ≥ 2 μV
- Duration ≥ 10 seconds
Why EEG is essential:
- Only 1/3 of EEG seizures have visible clinical signs
- Only 1/3 of those are recognized by experienced staff
- Only 1/4 of clinically suspected seizures have EEG confirmation
- → EEG prevents BOTH undertreating (missing subclinical seizures) AND overtreating (normal movements)
Important EEG terms:
- Electroclinical seizure - both clinical signs AND EEG discharge together
- Subclinical / electrographic-only seizure - EEG discharge without any clinical signs
- Clinical-only seizure - apparent clinical seizure with NO EEG discharge (brainstem release, or very deep seizure)
- Uncoupling - clinical signs stop but EEG seizure continues (common after giving AEDs)
- Burst suppression - alternating high-voltage bursts with long flat periods = ominous (Ohtahara syndrome)
- Trace alternant - normal pattern in quiet sleep of term infant (NOT burst suppression)
Bradley and Daroff's Neurology in Clinical Practice, p. 2857-2858
7b. Investigations - What to Order?
Immediate (bedside):
- Blood glucose (treat immediately if <45 mg/dL)
- Electrolytes: Na, Ca, Mg, phosphate
- ABG
Blood tests:
- CBC, CRP, blood culture
- LFT, metabolic screen
- Lactate, ammonia
- Serum amino acids (if IEM suspected)
CSF (lumbar puncture):
- Routine: cells, protein, glucose, Gram stain, culture
- Viral PCR: HSV, CMV, enterovirus
- Urine organic acids (for IEM)
- Special: urine α-aminoadipic semialdehyde (AASA) + serum pipecolic acid (for pyridoxine-dependent seizures)
Neuroimaging:
- Cranial ultrasound - first-line (available at bedside, no radiation, detects IVH, periventricular leukomalacia)
- MRI brain - best for cortical injury, HIE, cortical malformations, stroke (preferred over CT when available)
- CT head - if non-accidental trauma, intracranial hemorrhage, or emergency
Genetics:
- Gene panel or whole exome sequencing when etiology unknown (KCNQ2, SCN2A, etc.)
8. NEONATAL EPILEPSY SYNDROMES
8a. Benign Familial Neonatal Epilepsy (BFNE)
- Autosomal dominant inheritance
- Genes: KCNQ2, KCNQ3 (voltage-gated K⁺ channels), SCN2A
- Onset: first week of life
- Clonic or apneic seizures; resolves within first year
- Normal neurodevelopment; good prognosis
- Treatment: Na⁺ channel blockers (phenytoin/carbamazepine) very effective
8b. Benign Neonatal Seizures ("Fifth-day fits")
- Non-familial
- Onset: Days 4-6 of life
- EEG: discontinuous theta activity
- Seizures may escalate to status epilepticus briefly
- Good prognosis; normal development; seldom recur
8c. Ohtahara Syndrome (Early Infantile Epileptic Encephalopathy)
- Intractable tonic seizures + burst suppression on EEG
- Caused by numerous genetic abnormalities
- Some families report rhythmic movements in utero
- Very poor prognosis; often evolves to West syndrome → Lennox-Gastaut syndrome
- Refractory to most medications
8d. Early Myoclonic Encephalopathy
- Erratic focal myoclonus shifting around the body asynchronously
- Burst suppression on EEG
- Also poor prognosis; often metabolic cause
Bradley and Daroff's Neurology in Clinical Practice, p. 2856
9. METABOLIC/TREATABLE CAUSES - High Yield
Always consider treatable causes when etiology is unknown:
| Condition | Treatment | Clue |
|---|---|---|
| Pyridoxine (B6) deficiency / ALDH7A1 deficiency | Pyridoxine 100 mg IV (may cause apnea - give with EEG + resuscitation ready) | Seizures in utero, refractory to AEDs; urine AASA elevated |
| Folinic acid-responsive seizures | Folinic acid (allelic to pyridoxine-dep seizures) | |
| Pyridoxal phosphate (PLP) oxidase deficiency | Pyridoxal phosphate | |
| Biotinidase deficiency | Biotin supplementation | Skin rash, alopecia |
| Hypoglycemia | Dextrose IV | IDM, SGA, post-asphyxia |
| Hypocalcemia | Calcium gluconate IV | Tetany-like, early/late neonatal |
| Hypomagnesemia | Magnesium sulfate IV | Often accompanies hypocalcemia |
| Non-ketotic hyperglycinemia | Sodium benzoate + dextromethorphan | Hiccups, lethargy |
| Maple syrup urine disease | Dietary restriction of BCAAs | Sweet-smelling urine |
Practical strategy: When etiology is unknown, give folinic acid 5 mg/kg/day PO + pyridoxal phosphate 10 mg/kg q8h PO for 3 days empirically - continue if improvement seen, pending genetic results.
Bradley and Daroff's Neurology in Clinical Practice, p. 2856; Adams & Victor's, p. 352
10. MANAGEMENT
10a. General Principles
- Ensure airway, breathing, circulation (ABC)
- Treat hypoglycemia immediately (dextrose 10% IV 2 mL/kg)
- Correct electrolyte abnormalities (Ca, Na, Mg)
- Confirm seizure with EEG/aEEG if available
- Begin sepsis workup and start empiric antibiotics + acyclovir (meningitis cannot be excluded)
10b. Antiepileptic Drug (AED) Stepwise Approach
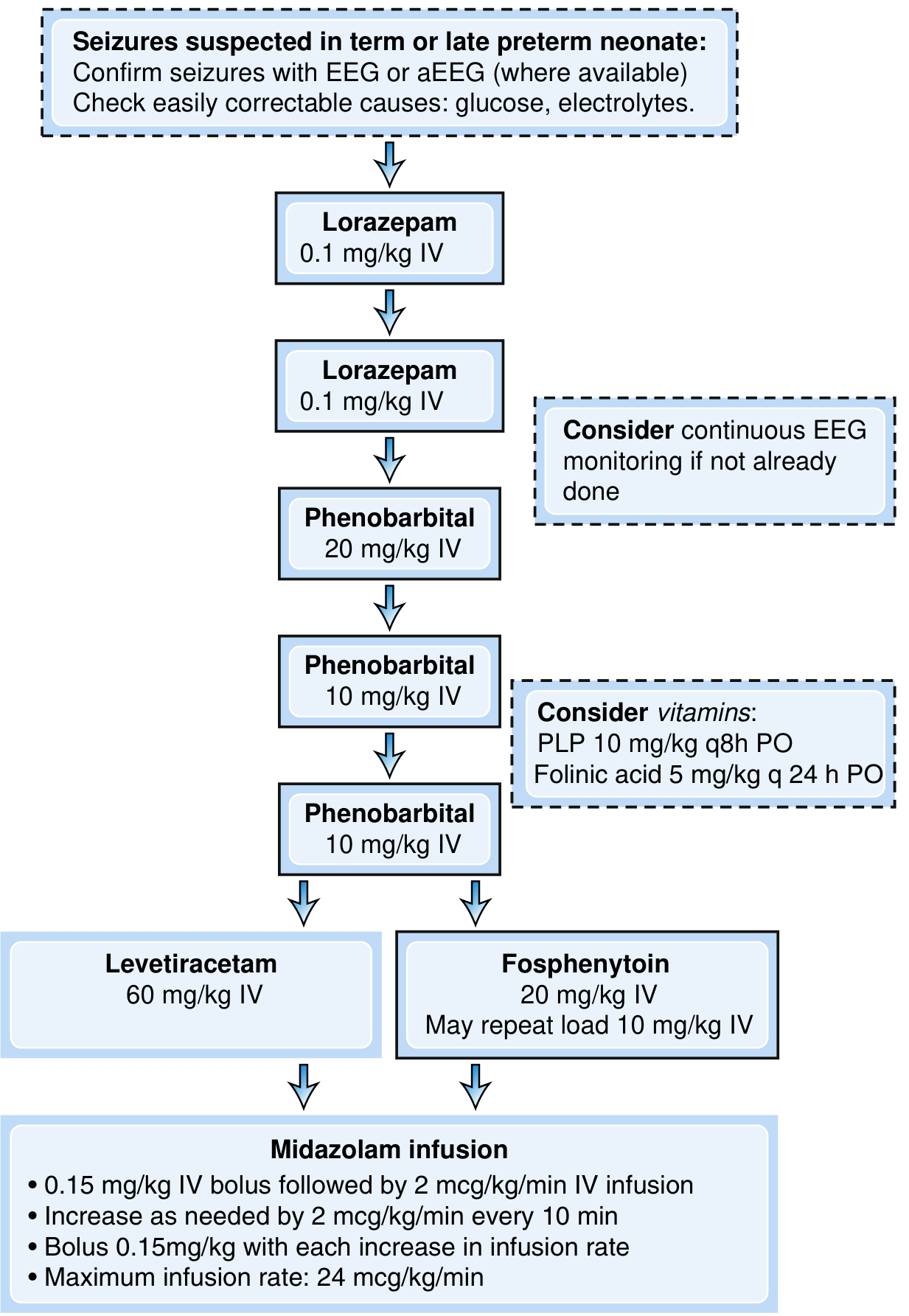
Step-by-step treatment:
Step 1 - First-line: Phenobarbital
- 20 mg/kg IV loading dose (WHO recommends phenobarbital as first-line)
- Controls ~50% of seizures
- Maintenance: 3-5 mg/kg/day (divided q12h)
- Side effects: respiratory depression, sedation
Step 2 - If seizures continue: Repeat doses or alternative
- Additional Phenobarbital: 10 mg/kg IV (can repeat once more: another 10 mg/kg)
- OR Phenytoin / Fosphenytoin 20 mg/kg IV (may repeat 10 mg/kg)
- Controls additional ~50% of remaining seizures
- Fosphenytoin preferred (less cardiac toxicity)
Benzodiazepines (Lorazepam 0.1 mg/kg IV or Midazolam):
- Useful when seizure is suspected clinically but unconfirmed by EEG
- Short half-life - less risk of prolonged sedation
- Also useful for acute breakthrough seizures
Step 3 - Refractory seizures:
- Levetiracetam 60 mg/kg IV - increasingly used; recent RCT shows it is LESS effective than phenobarbital
- Midazolam infusion - 0.15 mg/kg IV bolus, then 2 mcg/kg/min infusion; increase 2 mcg/kg/min every 10 min; max 24 mcg/kg/min
- Bumetanide (NKCC1 blocker) - experimental; targets the pathophysiological mechanism
Special notes on drug choice:
- Phenobarbital is first-line (WHO recommendation)
- Benzodiazepines are acceptable alternatives and good for acute/suspected seizures
- Levetiracetam has limited evidence; inferior to phenobarbital in RCT but widely used
- Na⁺ channel blockers (carbamazepine, phenytoin) especially effective for channelopathies (KCNQ2)
Bradley and Daroff's, p. 2858; Tintinalli's, p. (Ch. 138)
10c. Maintenance Therapy - After NICU Discharge
The decision to continue AEDs at discharge is individualized:
Risk factors for later epilepsy (consider continuing AEDs):
- Status epilepticus during neonatal period
- Severe HIE
- Required more than ONE AED to control seizures
Generally, most acute symptomatic seizures remit within a few days - seizures from HIE usually stop as the brain recovers; continuing long-term AEDs may not be necessary and has theoretical neurotoxicity concerns.
11. PROGNOSIS
The most important factor = the underlying etiology (not the seizure type or EEG pattern alone).
Risk of adverse neurodevelopmental outcome:
- 25%-70% of survivors will have neurodevelopmental impairment (cerebral palsy, intellectual disability, language/cognitive delays)
- Epilepsy after neonatal seizures: 10%-30%
- Infantile spasms (West syndrome) relatively common among neonatal seizure survivors
EEG background = most important prognostic EEG factor:
- Severe EEG background suppression → poor prognosis
- Burst-suppression pattern → very poor prognosis (Ohtahara syndrome)
- Background disturbance MORE predictive than specific interictal epileptiform discharges
Prognosis by etiology:
| Cause | Prognosis |
|---|---|
| Benign familial neonatal epilepsy | Excellent |
| Benign neonatal seizures ("5th day") | Excellent |
| Hypoglycemia (caught early) | Good if treated promptly |
| HIE (mild) | Moderate |
| HIE (severe) / Ohtahara | Poor |
| Cortical dysplasia | Poor (refractory seizures) |
| Early myoclonic encephalopathy | Poor |
Timing also matters:
- Seizures within 24-48 hours of a difficult birth = usually severe cerebral damage; ~50% of survivors severely disabled
- Seizures beginning several days to weeks after birth = more likely metabolic, more treatable, better prognosis
Bradley and Daroff's, p. 2858-2859; Adams & Victor's, p. 352
12. QUICK SUMMARY TABLE
| Feature | Detail |
|---|---|
| Definition | Paroxysmal neurological change + EEG discharge, first 28 days of life |
| Most common cause | HIE (~50% of term seizures) |
| Most common type | Subtle (50%) |
| Pathophysiology | GABA excitatory due to NKCC1/KCC2 imbalance → immature neurons depolarize with GABA |
| Gold standard diagnosis | Continuous EEG |
| First-line treatment | Phenobarbital 20 mg/kg IV |
| Why phenobarbital is partially ineffective | GABA excitatory in neonates |
| Key treatable cause | Pyridoxine deficiency (give 100 mg IV) |
| Prognosis determinant | Underlying etiology; EEG background activity |
| Risk of later epilepsy | 10-30% |
| Benign neonatal seizure gene | KCNQ2, KCNQ3 (BFNE) |
| Jitteriness vs. seizure key difference | Jitteriness - suppressed by holding, stimulus-sensitive, no EEG change |
13. KEY POINTS FOR EXAMS
- GABA is excitatory in neonates - key mechanism, explains why phenobarbital works poorly.
- Neonatal seizures are almost always acute symptomatic - find the cause.
- HIE = #1 cause in term neonates; intracranial hemorrhage + HIE together in preterm.
- Subtle seizures = most common type (lip-smacking, bicycling, eye deviation).
- Generalized tonic-clonic seizures DO NOT occur in neonates.
- EEG is mandatory - only 1/3 of EEG seizures have clinical signs.
- Jitteriness is NOT a seizure - it is stimulus-sensitive, suppressible, no EEG change.
- Pyridoxine deficiency = rare but completely treatable - always consider.
- Phenobarbital 20 mg/kg IV = first-line treatment.
- KCNQ2/KCNQ3 mutations = benign familial neonatal epilepsy - good prognosis.
- Burst suppression on EEG = Ohtahara syndrome = poor prognosis.
- Prognosis mainly determined by underlying etiology and EEG background quality.
- "5th day fits" (benign neonatal seizures) - onset days 4-6, self-limiting, good prognosis.
- Neonatal seizures may become uncoupled after AEDs - clinical signs stop but EEG seizure continues.
Sources: Bradley and Daroff's Neurology in Clinical Practice (9th ed.); Adams and Victor's Principles of Neurology (12th ed.); Tintinalli's Emergency Medicine; Rosen's Emergency Medicine
Give me 30 best MCQ quiz test on topic Perinatal hypoxia and Neonatal Seizures which covers all concept for MBBS student
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I now have rich content from multiple textbooks on both topics. I have comprehensive knowledge from the previous session's notes plus the additional HIE content just gathered. Let me now craft all 30 high-quality MCQs.
🧠 30 Best MCQ Quiz: Perinatal Hypoxia & Neonatal Seizures
For MBBS Students - Covers all core concepts from standard textbooks
SECTION A: PERINATAL HYPOXIA / HIE (Q1-Q12)
Q1. Which of the following is the MOST common cause of neonatal seizures in a term newborn?
- A) Hypoglycemia
- B) Intracranial hemorrhage
- C) Hypoxic-Ischemic Encephalopathy (HIE)
- D) Meningitis
✅ Answer: C - HIE
Explanation: HIE accounts for approximately 50% of neonatal seizures in term newborns. It is the single most common cause and should always be the first consideration after a difficult delivery. (Bradley & Daroff's, p. 2856)
Q2. The incidence of neonatal encephalopathy following perinatal asphyxia is approximately:
- A) 0.1-0.5 per 1000 live births
- B) 1-6 per 1000 live births
- C) 10-15 per 1000 live births
- D) 20-30 per 1000 live births
✅ Answer: B - 1-6 per 1000 live births
Explanation: Neonatal encephalopathy is estimated to occur in 1-6 per 1000 live births, with a mortality rate of ~20% in the newborn period and ~25% neurodevelopmental disability in survivors. (Adams & Victor's, p. 1038)
Q3. In a neonate with severe HIE, which of the following clinical findings is expected on examination within the first 12 hours?
- A) Hyperalertness and brisk reflexes
- B) Lethargy, hypotonia, and normal EEG
- C) Stupor or coma, irregular breathing, hypotonia, and seizures
- D) Normal tone with ankle clonus and soft fontanel
✅ Answer: C
Explanation: In severe HIE (Grade 3), stupor/coma is present from birth, respirations are irregular requiring ventilation, limbs are hypotonic and motionless, and convulsions usually begin within the first 12 hours. (Adams & Victor's, p. 1039)
Q4. A neonate is lethargic, obtunded, and hypotonic 24 hours after a difficult delivery. After 72 hours, the baby develops seizures, and the EEG shows epileptiform activity. This best corresponds to which grade of HIE (Sarnat/Fenichel classification)?
- A) Grade 1 (Mild)
- B) Grade 2 (Moderate)
- C) Grade 3 (Severe)
- D) Grade 0 (Normal)
✅ Answer: B - Grade 2 (Moderate)
Explanation: Moderate HIE presents with lethargy, obtundation, and hypotonia. After 48-72 hours, the baby may worsen with seizures, cerebral edema, and EEG abnormalities. A jittery hyperactive phase may precede deterioration. EEG shows epileptiform activity = unfavorable sign. (Adams & Victor's, p. 1039)
Q5. A term neonate born after complicated delivery has a cord blood gas pH of 6.95 and base deficit of 18 mEq/L. He requires ventilation at birth. Therapeutic hypothermia should ideally be initiated within:
- A) 1 hour of delivery
- B) 3 hours of delivery
- C) 6 hours of delivery
- D) 12 hours of delivery
✅ Answer: C - 6 hours of delivery
Explanation: Therapeutic hypothermia (target temperature 33-34°C) must be initiated within 6 hours of delivery for maximum neuroprotective benefit. It is indicated in infants ≥35 weeks with evidence of moderate-severe HIE. Criteria include: cord pH <7.0 OR base deficit >16, with evidence of encephalopathy. (Harriet Lane Handbook, p. 660)
Q6. Which of the following pH values on cord blood gas (or first-hour blood gas) meets criteria for therapeutic hypothermia (with additional clinical criteria)?
- A) pH 7.20 with base deficit 8
- B) pH 7.30 with base deficit 5
- C) pH 7.05 with base deficit 12 (borderline zone: 7.01-7.15, base deficit 10-15.9)
- D) pH 7.40 with base deficit 3
✅ Answer: C
Explanation: Criteria for hypothermia: pH <7.0 OR base deficit >16 = definite indication. For the borderline zone (pH 7.01-7.15, base deficit 10-15.9), ADDITIONAL criteria must be met (e.g., 10-min APGAR ≤5, need for ventilation ≥10 min, or clinical encephalopathy). (Harriet Lane Handbook, p. 660)
Q7. In mild HIE (Grade 1), which of the following findings is MOST characteristic?
- A) Burst-suppression on EEG
- B) Stupor, coma, and absent Moro reflex
- C) Hyperalertness, tremulousness, brisk reflexes, and NORMAL EEG
- D) Seizures within 12 hours of birth
✅ Answer: C
Explanation: Mild HIE features: hyperalertness, tremulousness of limbs and jaw ("jittery baby"), low-threshold Moro reflex, brisk reflexes, possible ankle clonus, soft fontanel, and normal EEG. Recovery is usually complete with low risk of handicap. (Adams & Victor's, p. 1039)
Q8. Which of the following is the MOST important imaging modality for identifying the pattern and extent of neonatal encephalopathy and predicting neurodevelopmental outcome?
- A) CT head
- B) Cranial ultrasound
- C) MRI brain
- D) PET scan
✅ Answer: C - MRI brain
Explanation: MRI is the modality of choice - it best delineates cortical injury, HIE pattern (basal ganglia injury, watershed injury), cortical malformations, and stroke. It also identifies if damage is antenatal vs. intrapartum in origin. Cranial ultrasound is first-line at the bedside but less sensitive. (Adams & Victor's, p. 1039-1040)
Q9. The MOST common MRI abnormality in children with cerebral palsy following perinatal injury is:
- A) Cortical-subcortical lesions
- B) Focal infarcts
- C) Periventricular leukomalacia (PVL)
- D) Basal ganglionic damage
✅ Answer: C - Periventricular leukomalacia
Explanation: PVL of prematurity was found in 42% of infants with cerebral palsy in MRI-clinical correlative studies, making it the most common finding. Basal ganglia damage follows at 13%, cortical-subcortical lesions at 9%. (Adams & Victor's, p. 1040)
Q10. Which of the following prenatal risk factors is associated with perinatal hypoxic-ischemic injury?
- A) Maternal diabetes with good glycemic control
- B) Toxemia of pregnancy (preeclampsia)
- C) Advanced maternal age
- D) Maternal obesity
✅ Answer: B - Toxemia of pregnancy
Explanation: Recognized prenatal risk factors include: toxemia of pregnancy, antepartum uterine hemorrhage, maternal hypotension, hypothyroidism, fertility treatment, and small-for-date fetuses. Freud famously noted that the birth process abnormality may itself be the consequence of pre-existing prenatal pathology. (Adams & Victor's, p. 1039)
Q11. Which of the following statements about cerebral palsy and perinatal asphyxia is CORRECT?
- A) Cerebral palsy incidence has decreased significantly with fetal monitoring and C-sections
- B) Intrapartum factors alone account for the majority of neonatal encephalopathy cases
- C) Intrapartum factors alone are identified as the cause in only about 5% of neonatal encephalopathy cases
- D) All infants with neonatal encephalopathy develop cerebral palsy
✅ Answer: C
Explanation: A large Western Australian study found neonatal encephalopathy in 3.8/1000 live term births, but causative intrapartum factors alone were identified in only 5%. Only ~10% of all infants with neonatal encephalopathy developed spastic quadriplegia. The incidence of cerebral palsy has NOT changed despite widespread fetal monitoring and C-sections. (Adams & Victor's, p. 1040)
Q12. Which of the following is an ABNORMAL EEG finding (as opposed to a normal variant) in a term newborn?
- A) Trace alternant pattern during quiet sleep
- B) Delta brushes in a preterm infant
- C) Burst-suppression pattern with long voltage-suppressed periods between high-voltage bursts
- D) Sleep state cycling
✅ Answer: C - Burst-suppression
Explanation: The trace alternant pattern (normal low-amplitude activity preserved between bursts) is a normal quiet sleep pattern in term infants. In contrast, burst suppression (long periods of complete voltage suppression between bursts of high-voltage spikes) is pathological and associated with severe encephalopathy such as Ohtahara syndrome. (Bradley & Daroff's, p. 2858)
SECTION B: NEONATAL SEIZURES - BASICS (Q13-Q20)
Q13. A medical student observes a newborn with lip-smacking movements, intermittent apnea, and bicycling movements of the legs. The staff initially dismiss these as "normal." This is MOST consistent with which type of neonatal seizure?
- A) Focal clonic
- B) Generalized tonic
- C) Subtle
- D) Myoclonic
✅ Answer: C - Subtle
Explanation: Subtle seizures are the MOST COMMON type (~50%) and include: eye deviation/blinking/fixed stare, repetitive mouth and tongue movements (lip-smacking, chewing), apnea, autonomic changes, and bicycling/swimming movements. They are most often missed by clinical staff. (Bradley & Daroff's, Table 110.1)
Q14. Why do neonates NOT exhibit generalized tonic-clonic seizures?
- A) GABA is more active in neonates
- B) Neonatal brain has excessive inhibition
- C) Immature synaptic connections and incomplete corticocortical myelination prevent organized, generalized seizure patterns
- D) Neonates have lower excitatory neurotransmitter levels
✅ Answer: C
Explanation: The immaturity of the neonatal cerebrum prevents fully organized seizure patterns, and incomplete corticocortical myelination prevents bihemispheric spread. This is why seizures remain fragmentary and focal in neonates. (Adams & Victor's, p. 352; Bradley & Daroff's, p. 2857)
Q15. The KEY pathophysiological reason why phenobarbital is often ineffective in treating neonatal seizures is:
- A) Phenobarbital does not cross the blood-brain barrier in neonates
- B) GABA acts as an EXCITATORY neurotransmitter in immature neurons due to high NKCC1 activity
- C) Neonates have excessive KCC2 activity
- D) Phenobarbital is metabolized too rapidly in neonates
✅ Answer: B
Explanation: In immature neurons, NKCC1 dominates → high intracellular Cl⁻ → when GABA-A receptors activate, Cl⁻ flows OUT → depolarization (excitatory). Phenobarbital is a GABA agonist - it enhances a paradoxically excitatory system. KCC2 (chloride extrusion) becomes dominant only with maturity. (Bradley & Daroff's, p. 2855)
Q16. A term neonate develops rhythmic clonic jerking of the right arm on day 3 of life. EEG shows focal left hemispheric discharge. The MOST likely underlying etiology is:
- A) HIE
- B) Focal cerebral infarction (neonatal stroke)
- C) Meningitis
- D) Hypocalcemia
✅ Answer: B - Focal cerebral infarction
Explanation: Focal clonic seizures in the term newborn are MOST commonly associated with focal cerebral infarction (neonatal arterial ischemic stroke). They represent a localized cortical discharge with an EEG correlate and indicate focal pathology. (Bradley & Daroff's, p. 2857)
Q17. What is the minimum duration of electrographic change required to diagnose a neonatal EEG seizure?
- A) 2 seconds
- B) 5 seconds
- C) 10 seconds
- D) 30 seconds
✅ Answer: C - 10 seconds
Explanation: EEG criteria for neonatal seizure: sudden electrographic change, repetitive waveforms evolving in morphology/frequency/location, amplitude ≥2 µV, and duration ≥10 seconds. (Bradley & Daroff's, p. 2858)
Q18. A nurse suspects a neonate is having seizures and documents 4 events in 1 hour. EEG monitoring is applied. It shows electrographic seizures occurring WITHOUT any visible clinical manifestations between nurse-documented events. These are termed:
- A) Electroclinical seizures
- B) Clinical-only seizures
- C) Subclinical (electrographic-only) seizures
- D) Pseudoseizures
✅ Answer: C - Subclinical seizures
Explanation: Subclinical seizures = EEG seizure discharge WITHOUT clinical signs. Studies show only 1/3 of neonatal EEG seizures have clinical manifestations - meaning the majority are subclinical and can only be detected with EEG monitoring. (Bradley & Daroff's, p. 2857)
Q19. A neonate is shaking after birth. The intern notes the movements STOP when the right arm is passively flexed and the movements occur only when the baby is startled by a loud noise. There are no eye movements and no change in heart rate. This is MOST consistent with:
- A) Clonic seizure
- B) Subtle seizure
- C) Jitteriness
- D) Myoclonic seizure
✅ Answer: C - Jitteriness
Explanation: Jitteriness is distinguished from seizures by: stimulus-sensitive, suppressible by passive flexion, no abnormal eye movements, no autonomic changes (tachycardia, apnea), and movement is a tremor (equal amplitude both ways). In contrast, clonic seizures have a fast AND slow component, are not suppressed by holding, and have EEG changes. (Bradley & Daroff's, p. 2857)
Q20. "Fifth-day fits" (benign neonatal seizures) are characterized by ALL of the following EXCEPT:
- A) Onset on days 4-6 of life
- B) May progress to brief status epilepticus
- C) Discontinuous theta activity on EEG
- D) Poor prognosis with high risk of recurrent epilepsy
✅ Answer: D - Poor prognosis is INCORRECT
Explanation: "Fifth-day fits" have good prognosis - normal development and seizures seldom recur. They begin on days 4-6, are non-familial, may include partial seizures that briefly escalate, with discontinuous theta on EEG. The outlook is excellent. (Adams & Victor's, p. 352)
SECTION C: ETIOLOGY, DIAGNOSIS & TREATMENT (Q21-Q30)
Q21. A newborn presents with seizures within the first hour of life after a very difficult delivery with prolonged cord prolapse. Seizures on Day 1 are MOST likely due to:
- A) Group B streptococcal meningitis
- B) Hyponatremia
- C) Hypoxic-ischemic encephalopathy
- D) Inborn error of metabolism
✅ Answer: C - HIE
Explanation: Seizures occurring within the first 24 hours (especially first 12 hours) after a complicated delivery are characteristic of HIE. HIE and intracranial hemorrhage dominate in the first 1-2 days. Infection and metabolic disorders typically present later. (Adams & Victor's, p. 352)
Q22. A 5-day-old infant develops refractory seizures unresponsive to phenobarbital and phenytoin. There is history of similar movements in utero. Alpha-aminoadipic semialdehyde (AASA) is elevated in the urine. The MOST appropriate treatment is:
- A) Levetiracetam 60 mg/kg IV
- B) Midazolam infusion
- C) Pyridoxine (Vitamin B6) 100 mg IV
- D) Magnesium sulfate IV
✅ Answer: C - Pyridoxine 100 mg IV
Explanation: Pyridoxine-dependent epilepsy (ALDH7A1/antiquitin deficiency) presents with refractory neonatal seizures, may cause seizures IN UTERO, and is characterized by elevated urine AASA and serum pipecolic acid. Treatment: 100 mg IV pyridoxine (give with EEG monitoring as it may cause apnea). Classically shows dramatic response. (Bradley & Daroff's, p. 2856; Adams & Victor's, p. 352)
Q23. The World Health Organization (WHO) recommends which drug as FIRST-LINE treatment for neonatal seizures?
- A) Levetiracetam
- B) Lorazepam
- C) Midazolam
- D) Phenobarbital
✅ Answer: D - Phenobarbital
Explanation: Phenobarbital 20 mg/kg IV is the WHO-recommended first-line agent for neonatal seizures. It controls ~50% of seizures. Despite its paradoxical mechanism (GABA excitatory in neonates), it remains the standard of care. A recent RCT confirmed levetiracetam is LESS effective than phenobarbital. (Bradley & Daroff's, p. 2858)
Q24. After giving phenobarbital 20 mg/kg IV, a neonate continues to have electrographic seizures. The clinical shaking movements have stopped. This phenomenon is termed:
- A) Electroclinical dissociation
- B) Uncoupling
- C) Pseudoseizure
- D) Subclinical seizure
✅ Answer: B - Uncoupling
Explanation: Uncoupling is the phenomenon where clinical manifestations stop but EEG seizures persist after administration of anticonvulsants. It is common in neonates after AEDs and is why continuous EEG monitoring is essential - clinical resolution does NOT mean seizure control. (Bradley & Daroff's, p. 2858)
Q25. Which gene mutation is responsible for Benign Familial Neonatal Epilepsy (BFNE), and what is the inheritance pattern?
- A) SCN1A; X-linked
- B) MECP2; autosomal recessive
- C) KCNQ2 / KCNQ3; autosomal dominant
- D) TSC1; autosomal recessive
✅ Answer: C - KCNQ2/KCNQ3, autosomal dominant
Explanation: BFNE is caused by mutations in KCNQ2 or KCNQ3 (voltage-gated potassium channel genes), inherited in an autosomal dominant pattern. SCN2A is also implicated. Seizures onset in the first week, remit within the first year, and prognosis is excellent with normal neurodevelopment. (Bradley & Daroff's, p. 2856)
Q26. A neonate born at 28 weeks gestation develops seizures on day 2 of life. Cranial ultrasound shows intraventricular blood. Which TWO etiologies should be considered as MOST likely in this preterm neonate?
- A) HIE and meningitis
- B) HIE and intracranial hemorrhage (IVH)
- C) Hypoglycemia and hypocalcemia
- D) KCNQ2 mutation and hypocalcemia
✅ Answer: B - HIE and IVH
Explanation: In preterm newborns, HIE and intracranial hemorrhage (IVH) each account for approximately one-third of seizures (unlike term neonates where HIE dominates). IVH occurs in 30-40% of infants <1500g and 50-60% of infants <1000g, with 90% of cases occurring within the first 96 hours. (Bradley & Daroff's, p. 2856; Harriet Lane, p. 661)
Q27. A neonate with seizures has a normal MRI, no metabolic abnormality, normal septic workup, and an EEG showing burst-suppression pattern. Seizures are intractable tonic seizures from the first days of life. Genetic testing reveals a pathogenic variant in STXBP1. This presentation is MOST consistent with:
- A) Benign familial neonatal epilepsy
- B) Pyridoxine-dependent epilepsy
- C) Early infantile epileptic encephalopathy (Ohtahara syndrome)
- D) Fifth-day fits
✅ Answer: C - Ohtahara syndrome
Explanation: Ohtahara syndrome (early infantile epileptic encephalopathy) is characterized by: intractable tonic seizures, burst-suppression on EEG from the first days/weeks of life, caused by genetic abnormalities (STXBP1, SCN2A, KCNQ2 among others), and has a very poor prognosis - often evolving to West syndrome and then Lennox-Gastaut syndrome. (Bradley & Daroff's, p. 2856)
Q28. What is the MOST important determinant of prognosis following neonatal seizures?
- A) Number of seizures in the first 24 hours
- B) Type of seizure (clonic vs. subtle)
- C) The underlying etiology
- D) The age at seizure onset
✅ Answer: C - Underlying etiology
Explanation: The underlying etiology is the major determinant of prognosis. The EEG background activity (severity of suppression) is the most important EEG prognostic marker. 25-70% of survivors have neurodevelopmental impairment; 10-30% develop epilepsy. Benign etiologies (BFNE) → excellent prognosis. HIE/cortical dysplasia → poor prognosis. (Bradley & Daroff's, p. 2858-2859)
Q29. A neonate with late-onset seizures (day 5-7) is found to have hypocalcemia with serum calcium of 6.2 mg/dL. The mother is exclusively formula-feeding with cow's milk-based formula. What is the MOST likely mechanism of hypocalcemia in this case?
- A) Maternal hypoparathyroidism
- B) Vitamin D deficiency from sunlight deprivation
- C) High phosphate load from cow's milk causing hyperphosphatemia → hypocalcemia
- D) Prematurity-related hypocalcemia
✅ Answer: C - Hyperphosphatemia from cow's milk
Explanation: Late neonatal hypocalcemia (days 5-10) is classically caused by high phosphate load from cow's milk formula, leading to hyperphosphatemia which suppresses calcium. This is also associated with hypomagnesemia. Early neonatal hypocalcemia (days 1-3) is associated with prematurity, IDM, and asphyxia. (Adams & Victor's, p. 352; standard pediatric textbook knowledge)
Q30. In management of refractory neonatal seizures unresponsive to phenobarbital, phenytoin, AND levetiracetam, the NEXT most appropriate agent is:
- A) Valproate 20 mg/kg IV
- B) Carbamazepine oral
- C) Diazepam rectal
- D) Midazolam IV infusion (0.15 mg/kg bolus then 2 mcg/kg/min infusion)
✅ Answer: D - Midazolam infusion
Explanation: For refractory seizures not controlled by standard medications, midazolam infusion is indicated: bolus 0.15 mg/kg IV, followed by infusion starting at 2 mcg/kg/min, increasing by 2 mcg/kg/min every 10 min as needed; maximum rate is 24 mcg/kg/min. Midazolam is preferred over diazepam due to its shorter half-life and titratable infusion. (Bradley & Daroff's, p. 2858 - Fig. 110.5)
📊 Quick Score Card
| Marks | Interpretation |
|---|---|
| 27-30 / 30 | Excellent - exam-ready |
| 22-26 / 30 | Good - revise weak areas |
| 16-21 / 30 | Fair - review pathophysiology & management |
| <16 / 30 | Needs revision - re-read the notes |
🔑 High-Yield Recap (Most Tested Points)
- HIE = #1 cause of neonatal seizures in term neonates (~50%)
- GABA is excitatory in neonates (NKCC1 dominant) → phenobarbital works poorly
- Subtle seizures = most common type (lip-smacking, bicycling, apnea)
- No GTCs in neonates - due to immature myelination
- EEG = gold standard - only 1/3 of EEG seizures have clinical signs
- Uncoupling = clinical stops but EEG seizure persists after AED
- Jitteriness = stimulus-sensitive, suppressible, NO EEG change
- Phenobarbital 20 mg/kg IV = first-line (WHO)
- Therapeutic hypothermia within 6 hours for moderate/severe HIE
- KCNQ2/KCNQ3 = BFNE = autosomal dominant = GOOD prognosis
- Burst-suppression = Ohtahara syndrome = POOR prognosis
- Pyridoxine 100 mg IV = pyridoxine-dependent epilepsy = TREATABLE
- Focal clonic = focal cerebral infarction
- Prognosis = determined by underlying etiology, not seizure type
Sources: Bradley and Daroff's Neurology in Clinical Practice | Adams and Victor's Principles of Neurology (12th Ed.) | Tintinalli's Emergency Medicine | Harriet Lane Handbook (23rd Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.