Common peroneal nerve pg answer using structure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have all the information needed for a comprehensive, well-structured answer. Here it is:
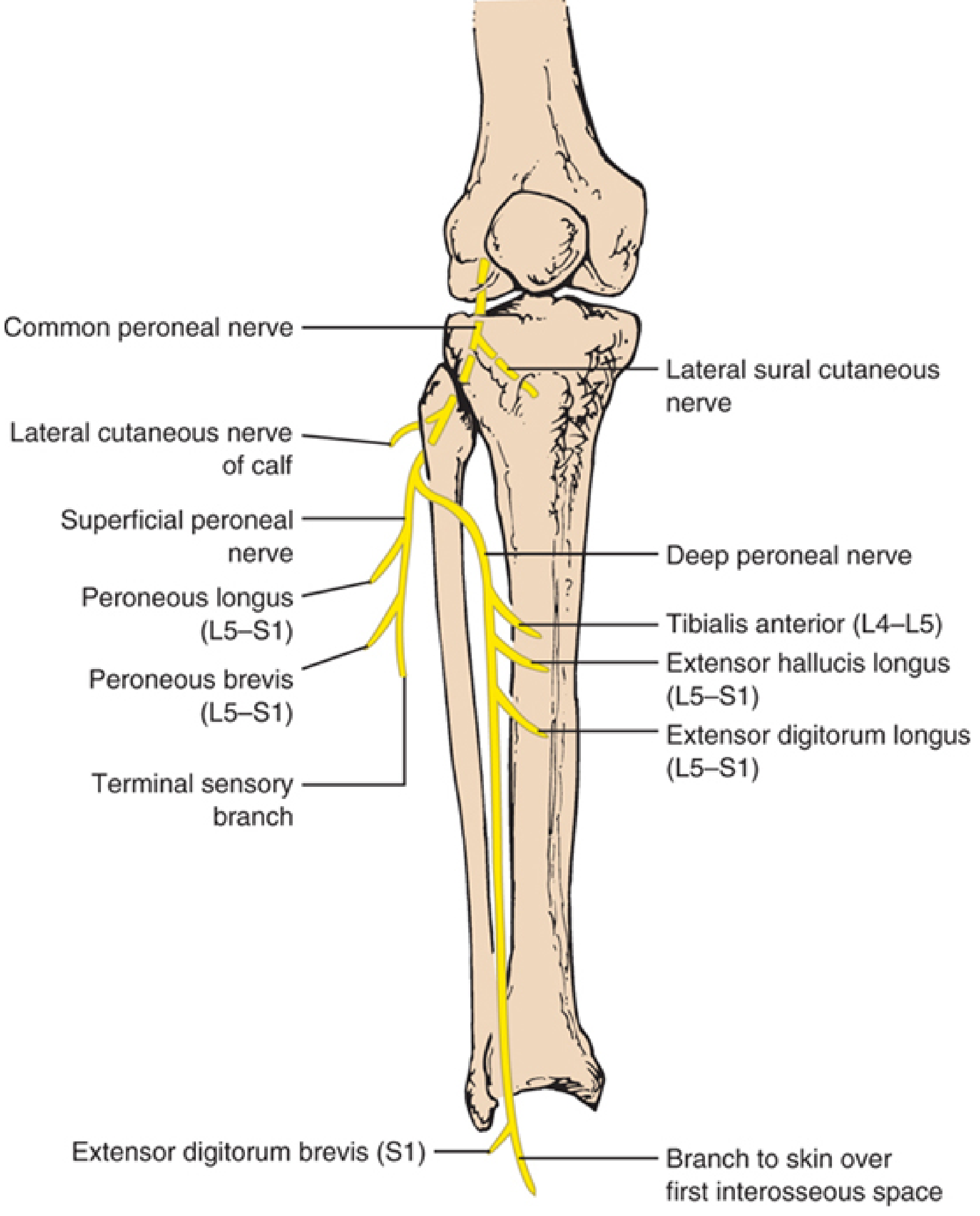
Common Peroneal Nerve
1. Origin & Root Values
- The common peroneal nerve (also called the common fibular nerve) is the lateral division of the sciatic nerve
- Root values: L4, L5, S1, S2
- It separates from the sciatic nerve just proximal to the popliteal fossa
2. Course
| Segment | Detail |
|---|---|
| Popliteal fossa | Travels along the medial border of the biceps femoris tendon in the fat plane lateral to the fossa |
| Around fibular head | Winds around the neck of the fibula - most vulnerable point |
| Fibular tunnel | Enters the substance of the peroneus longus muscle (fibular tunnel) |
| Terminal division | Divides into deep and superficial peroneal nerves at the fibular neck |
3. Branches
In the Popliteal Fossa (before division)
- Lateral sural cutaneous nerve - joins the medial sural cutaneous nerve (from tibial nerve) to form the sural nerve
- Lateral cutaneous nerve of the calf - descends along lateral head of gastrocnemius; supplies skin on the lateral aspect of the leg below the knee
Deep Peroneal Nerve (anterior tibial nerve)
Supplies the anterior compartment muscles:
| Muscle | Root | Action | Test |
|---|---|---|---|
| Tibialis anterior | L4-L5 | Dorsiflexion + inversion of foot | Walk on heels / dorsiflex against resistance |
| Extensor hallucis longus | L5-S1 | Extension of great toe + dorsiflexion | Dorsiflex distal phalanx of big toe against resistance |
| Extensor digitorum longus | L5-S1 | Extension of 4 lateral toes + dorsiflexion | Dorsiflex toes against resistance |
| Extensor digitorum brevis | L5-S1 (S1) | Extension of large toe + 3 medial toes | Dorsiflex proximal phalanges against resistance |
Sensory: Terminal branch to the skin of the first interosseous space (web between 1st and 2nd toes)
Superficial Peroneal Nerve
Supplies the lateral compartment muscles:
| Muscle | Root | Action |
|---|---|---|
| Peroneus longus | L5-S1 | Plantar flexion + eversion of foot |
| Peroneus brevis | L5-S1 | Plantar flexion + eversion of foot |
Sensory: Skin of the lateral distal lower leg and dorsum of the foot and toes (except first interosseous space)
Note: An accessory deep peroneal nerve (variant of the superficial peroneal nerve) is present in 20-28% of individuals - it supplies the lateral part of extensor digitorum brevis by winding around the lateral malleolus.
4. Sites & Causes of Injury
Most Common Site: Fibular Head/Neck
The nerve is superficial and unprotected here - this is the most common compressive neuropathy in the lower extremity.
Causes at fibular head:
- Compression - habitual leg crossing (most common in thin/emaciated patients), casts, orthoses, pneumatic compression stockings, operative positioning (lateral decubitus, lithotomy)
- Stretch injury - acute forceful foot inversion, prolonged squatting (strawberry pickers' palsy), yoga (yoga foot drop)
- Trauma - laceration, fibular fracture, knee dislocation, gunshot wounds
- Iatrogenic - total knee arthroplasty, hip arthroplasty (lithotomy position), arthroscopic knee surgery
- Intraneural ganglia - from disruption of superior tibiofibular joint capsule (underappreciated; presents with pain, fluctuating weakness, palpable mass)
- Postpartum - stirrup compression or bilateral "pushing palsy" during labor
- Bilateral - weight loss/emaciation, bedridden state, vasculitis
5. Clinical Features of Common Peroneal Palsy
| Feature | Detail |
|---|---|
| Motor | Foot drop (weakness of dorsiflexion + toe extension); weakness of foot eversion |
| Gait | Steppage gait (high stepping to clear the dropped foot) |
| Sensory | Loss over lateral lower two-thirds of leg + dorsum of foot |
| Spared | Foot inversion (tibial nerve + L5 root via tibialis posterior) |
| Pain | Usually absent - significant pain suggests intraneural ganglion |
The deep branch is more commonly affected than the whole nerve. Eversion may be relatively spared when the lesion is selective to the deep peroneal nerve (except for first web space sensation).
6. Localized Syndromes
A. Deep (Anterior Tibial) Peroneal Nerve Syndrome
- Motor deficit: paresis/paralysis of toe and foot dorsiflexion
- Sensory: limited to web of skin between 1st and 2nd toes
- Distal compression at ankle = Anterior Tarsal Tunnel Syndrome (beneath crural cruciate ligament) - causes isolated extensor digitorum brevis paresis/atrophy ± sensory loss in first web space
B. Superficial Peroneal Nerve Syndrome
- Paresis of peronei (foot eversion) + sensory loss over lateral distal leg and dorsum
- First web space is spared
- Purely sensory form: compression at fascial exit point (high lace boots, skates)
C. Lateral Cutaneous Nerve of Calf Neuropathy
- Numbness/pain over posterolateral leg from knee to lower third
- Rare; seen in diabetics or with peripopliteal cystic bursitis
7. Differential Diagnosis of Foot Drop
| Condition | Key Distinguishing Feature |
|---|---|
| Common peroneal neuropathy | Eversion + dorsiflexion weak; inversion spared; sensory loss dorsum of foot |
| L5 radiculopathy | Inversion also weak (tibialis posterior); hip abduction may be weak; back pain; EMG shows paraspinal involvement |
| Sciatic nerve lesion | Hamstrings affected; whole leg involved |
| Tibialis anterior tendon (TAT) rupture | Normal EMG; palpable tendon defect on dorsum of ankle; toe extensors/eversion preserved |
| Lumbosacral plexopathy | Multiple root distributions affected |
Key distinguishing point: foot inversion is preserved in peroneal palsy (inversion = tibialis posterior via tibial nerve / tibialis anterior via deep peroneal - the posterior tibial component is spared).
8. Investigations
- EMG/NCS - confirms axonal vs. demyelinating injury; identifies fascicular patterns; assesses prognosis
- MRI nerve/popliteal fossa - detects intraneural ganglia, masses, Baker cyst
- If intraneural ganglion suspected: look for articular branch connection to superior tibiofibular joint
9. Prognosis & Management
- Prognosis is generally good in partial paralysis from compressive causes
- Remove/correct precipitating cause
- Intraneural ganglia: surgical decompression with disconnection of articular branch
- Foot-drop splint/AFO during recovery
- Nerve repair for complete lacerations
Sources: Localization in Clinical Neurology 8e; Bradley and Daroff's Neurology in Clinical Practice; Adams and Victor's Principles of Neurology 12e; Imaging Anatomy Text and Atlas Vol. 3
This is a shared conversation. Sign in to Orris to start your own chat.