Ecg in detail for easy explain
Reading File
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram waves P QRS T normal components labeled diagram
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Searching Images
12 lead ECG electrode placement positions chest precordial limb leads
Reading File
Loading Image
Searching Images
ECG ST segment elevation myocardial infarction STEMI abnormal changes
Reading File
Loading Image
I now have comprehensive content. Let me compile the complete ECG guide:
ECG (Electrocardiogram) — Complete Easy Guide
🫀 What Is an ECG?
An ECG (Electrocardiogram) records the electrical activity of the heart from electrodes placed on the skin. It translates the heart's electrical events into a waveform on paper, giving a window into rhythm, conduction, and muscle health — all in real time.
"Electrical events of the cardiac pacemaker and the specialized conduction system are represented by the ECG at the body surface." — Miller's Anesthesia
1. The ECG Paper
The graph paper is standardized so that time and voltage are always consistent:
| Measurement | Small box (1 mm) | Large box (5 mm) |
|---|---|---|
| Time (horizontal) | 0.04 sec (40 ms) | 0.20 sec (200 ms) |
| Voltage (vertical) | 0.1 mV | 0.5 mV |
- A standard ECG records 10 seconds of cardiac activity
- It usually records all 12 leads simultaneously — each group recorded for 2.5 seconds
2. The ECG Waveform — One Heartbeat
Every heartbeat produces this sequence of waves:
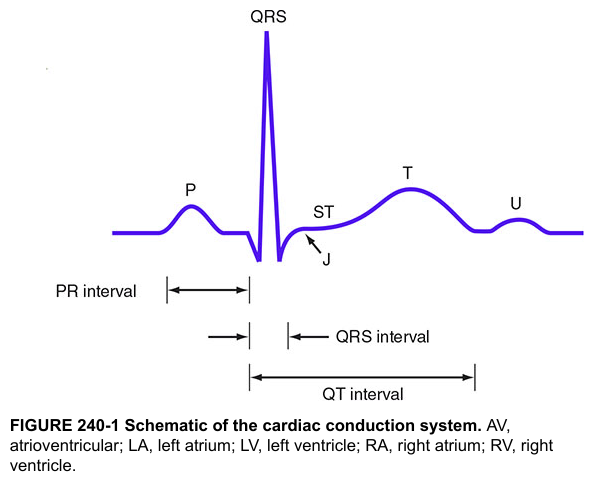
🔵 P Wave — Atrial Depolarization
- The SA node fires → electrical impulse spreads across both atria
- Atria contract (atrial systole = "atrial kick")
- On ECG: small rounded upward bump
- Normal duration: < 0.12 sec (120 ms)
- Broad P wave = atrial enlargement or conduction delay
🟡 PR Interval — AV Node Delay
- Measured from start of P wave → start of QRS
- Represents the pause at the AV node (gateway between atria and ventricles)
- This delay allows the ventricles to fill before contracting
- Normal: 0.09–0.20 sec (90–200 ms)
-
0.20 sec = 1st degree AV block (prolonged conduction)
- Short PR = Wolff-Parkinson-White (pre-excitation via accessory pathway)
🔴 QRS Complex — Ventricular Depolarization
- Impulse travels: His bundle → left & right bundle branches → Purkinje fibers → ventricular muscle
- Both ventricles depolarize and contract simultaneously
- On ECG: the tallest, sharpest deflection
- Normal duration: 0.075–0.11 sec (75–110 ms)
Understanding the letters:
| Letter | Meaning |
|---|---|
| Q | First negative deflection |
| R | Positive deflection |
| S | Negative deflection after R |
| Capital (Q, R, S) | Large amplitude (≥ 5 mm) |
| Lowercase (q, r, s) | Small amplitude (< 5 mm) |
Pathological Q waves (deep, wide) indicate prior myocardial infarction
🟢 ST Segment — Ventricular "Plateau"
- Flat line between the end of QRS (J-point) and start of T wave
- Represents early ventricular repolarization
- Normally isoelectric (flat)
- ST elevation = acute injury/infarction (STEMI)
- ST depression = ischemia or subendocardial infarction
🟠 T Wave — Ventricular Repolarization
- Ventricles reset electrically
- Normally upright (positive) in most leads
- Inverted T wave = ischemia, ventricular strain, or electrolyte abnormality
- Tall, peaked T waves = hyperkalemia or early MI (hyperacute T wave)
⚪ U Wave — Small wave after T
- Small, often invisible upward deflection after the T wave
- Represents late repolarization of Purkinje fibers
- Prominent U waves → hypokalemia
🔵 QT Interval — Full Ventricular Cycle
- Measured from start of QRS → end of T wave
- Includes both depolarization + repolarization
- Must be corrected for heart rate using Bazett's formula:
QTc = QT ÷ √(RR interval)
Normal QTc:
- Males: 390–450 ms
- Females: 390–460 ms
Prolonged QTc → risk of Torsades de Pointes (dangerous ventricular tachycardia)
3. Normal ECG Intervals at a Glance
| Parameter | Normal Value |
|---|---|
| Heart rate | 50–100 bpm |
| P wave duration | < 120 ms |
| PR interval | 90–200 ms |
| QRS duration | 75–110 ms |
| QTc (males) | 390–450 ms |
| QTc (females) | 390–460 ms |
| QRS axis | −30° to +90° |
(Goldman-Cecil Medicine)
4. Heart Rate Calculation
Method 1 (formula):
HR = 60,000 ÷ RR interval (in ms)
Method 2 (big boxes — for regular rhythm):
Count large boxes between two R waves:
| Boxes | Rate |
|---|---|
| 1 | 300 bpm |
| 2 | 150 bpm |
| 3 | 100 bpm |
| 4 | 75 bpm |
| 5 | 60 bpm |
| 6 | 50 bpm |
Method 3 (10-second strip): Count total QRS complexes × 6 = bpm
5. The 12 Leads — What They "See"
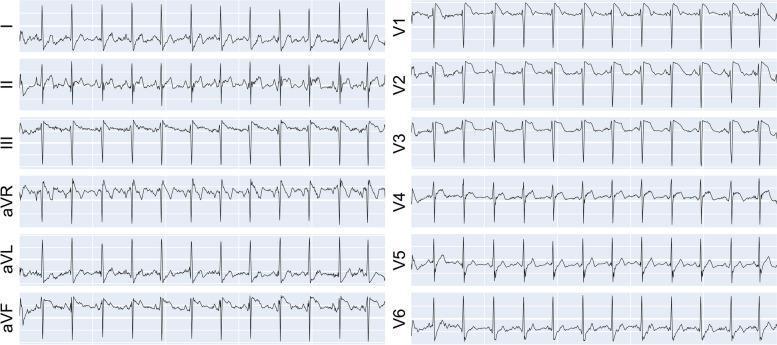
12 leads = 12 different "camera angles" of the heart's electricity
Limb Leads (Frontal Plane)
| Lead | View |
|---|---|
| I | Left side of heart (lateral) |
| II | Inferior (bottom) |
| III | Inferior |
| aVR | Right side (usually negative) |
| aVL | Lateral (high) |
| aVF | Inferior (feet direction) |
Precordial Leads (Horizontal Plane — chest)
| Lead | Anatomical Position | What It Views |
|---|---|---|
| V1 | 4th ICS, right sternal border | Septum / RV |
| V2 | 4th ICS, left sternal border | Septum / RV |
| V3 | Between V2 and V4 | Anterior wall |
| V4 | 5th ICS, midclavicular line | Anterior wall |
| V5 | Anterior axillary line | Lateral wall |
| V6 | Mid-axillary line | Lateral wall |
Reciprocal changes: When one area is injured (ST elevation), the opposite leads show ST depression — this is a clue for localizing an MI.
6. The Cardiac Conduction Pathway (Simplified)
SA Node → Atria (P wave)
↓
AV Node (PR interval delay)
↓
Bundle of His
↓
Right Bundle Branch Left Bundle Branch
↓ ↓
Purkinje Fibers → Ventricular Muscle (QRS complex)
↓
Ventricular Repolarization (T wave)
7. Key ECG Patterns to Recognize
✅ Normal Sinus Rhythm
- Regular P wave before every QRS
- Rate 60–100 bpm
- PR interval 120–200 ms
- QRS < 110 ms
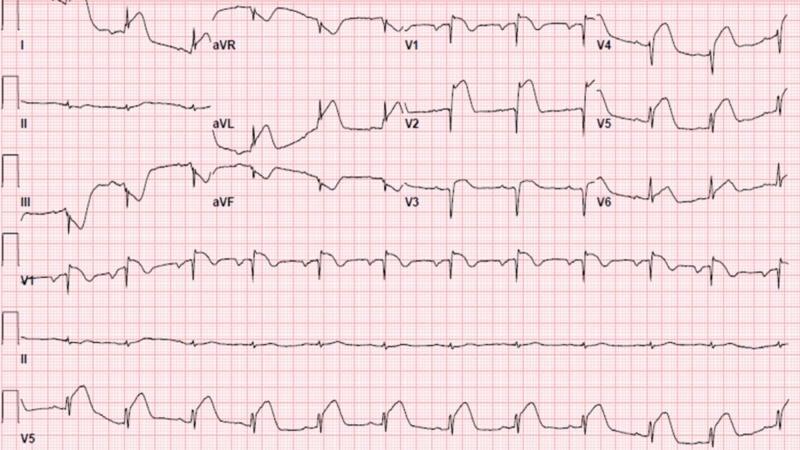
🔴 STEMI (Heart Attack — Acute MI)
- ST elevation ≥ 1 mm in ≥ 2 contiguous leads
- Tombstone morphology (ST merges with T wave)
- Pathological Q waves develop over hours
- Reciprocal ST depression in opposite leads
⚡ Ventricular Tachycardia (VT)
- Wide QRS complexes (> 120 ms)
- No visible P waves
- Rate > 100 bpm
- Life-threatening
💗 Atrial Fibrillation (AF)
- No P waves — replaced by chaotic fibrillatory baseline
- Irregularly irregular RR intervals
- Narrow QRS (unless aberrant conduction)
8. Systematic Approach to Reading Any ECG
Use this 7-step method every time:
- Rate — Count beats (fast/normal/slow?)
- Rhythm — Regular or irregular? P before every QRS?
- P wave — Present? Shape? Duration < 120 ms?
- PR interval — Normal 120–200 ms? Prolonged = AV block?
- QRS complex — Width < 110 ms? Pathological Q waves?
- ST segment — Elevation or depression?
- T wave — Upright or inverted? Peaked?
Quick Memory Trick for Waves
| Wave | Stands For |
|---|---|
| P | Pacemaker fires (SA node) → atrial activation |
| PR | Pause at the node (Relay station = AV node) |
| QRS | Quick Rapid Spike = ventricles fire |
| T | Tidy up (repolarization — heart resets) |
Sources: Goldman-Cecil Medicine (25th ed.) · Miller's Anesthesia (10th ed.) · Harrison's Principles of Internal Medicine (21st ed.) · Fuster and Hurst's The Heart (15th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.