Sd curve for orbicularis occuli muscle praticle with application uses and doses and type of graph
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Searching PubMed
strength duration curve orbicularis oculi electrotherapy
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
strength duration curve rheobase chronaxie nerve muscle electrotherapy
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive data to provide a thorough answer. Let me compile the complete response.
Strength-Duration (SD) Curve — Orbicularis Oculi: Complete Guide
What is the SD Curve?
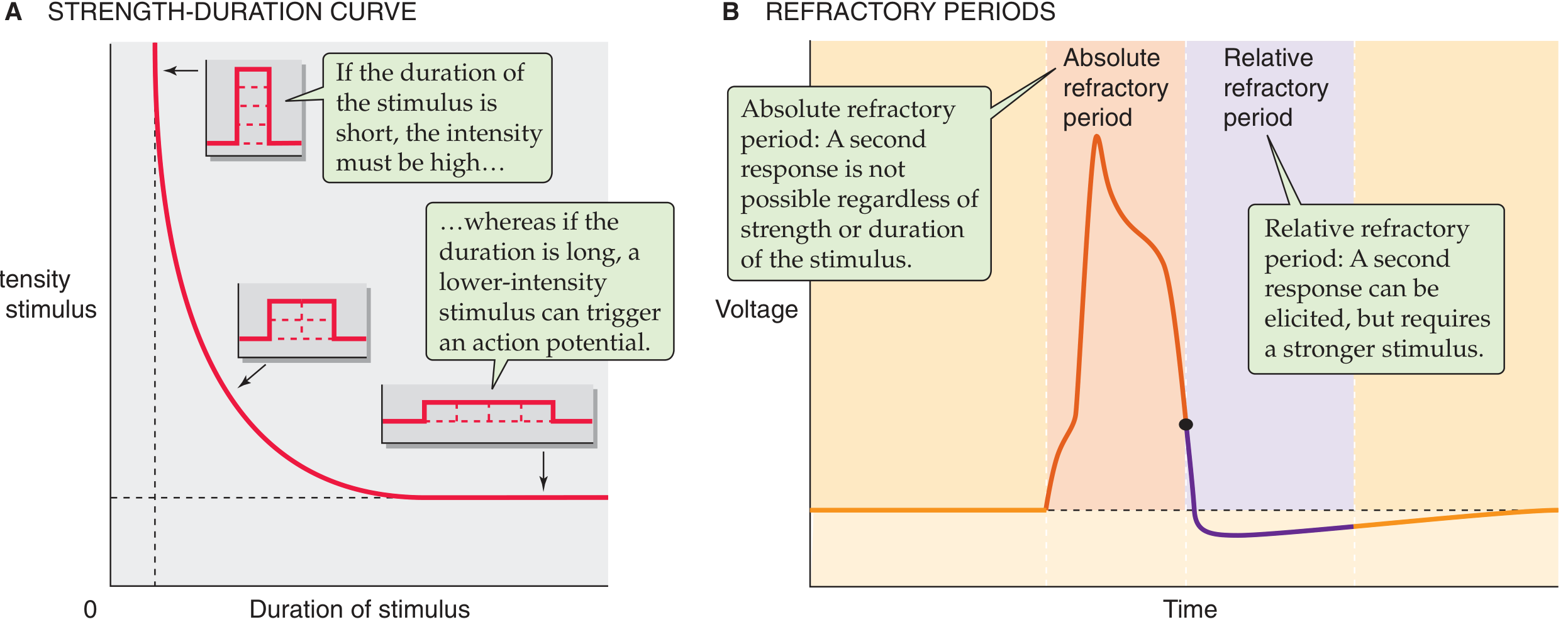
The Strength-Duration (SD) Curve is a graphical representation of the relationship between the intensity (strength) of an electrical stimulus and the minimum duration required to just excite a nerve or muscle (i.e., reach threshold and evoke an action potential).
"The minimal intensity of stimulating current needed to produce an action potential is called the threshold intensity; it varies with the stimulus duration. A weak stimulus needs a long duration, and a strong stimulus is sufficient at a short duration. The relation between the strength and the duration of a threshold stimulus is called the strength-duration curve." — Ganong's Review of Medical Physiology
Type of Graph
The SD curve is a rectangular hyperbola plotted on:
- X-axis: Duration of stimulus (milliseconds) — pulse width
- Y-axis: Intensity/Strength of stimulus (mA or volts) — threshold current
Key Features of the Graph
| Feature | Definition |
|---|---|
| Rheobase | Minimum stimulus intensity required to elicit an action potential at infinite (very long) duration — the horizontal asymptote of the curve |
| Chronaxie | Minimum stimulus duration required at twice the rheobase intensity — the most clinically useful parameter |
| Vertical asymptote | Below a minimum pulse width, no action potential is possible regardless of intensity |
| Horizontal asymptote | Below the rheobase intensity, no action potential is possible regardless of duration |
"The rheobase is the minimum intensity of stimulation required to generate an action potential when the stimulation is of infinite duration. When the stimulus intensity is twice the rheobase, the minimum duration required to achieve an action potential is the chronaxie." — Medical Physiology (Boron & Boulpaep)
Normal vs. Denervated Muscle — SD Curve Differences
| Parameter | Normal (Innervated) Muscle | Denervated Muscle |
|---|---|---|
| Curve shape | Steep hyperbola — shifts left | Flattened, shifted right |
| Chronaxie | Short (0.1–1 ms for nerve; ~1 ms for muscle) | Prolonged (10–100 ms) |
| Rheobase | Lower | Higher |
| Response | Sharp threshold (responds to short pulses) | Requires longer pulses |
| Accommodation | Normal | Absent — responds to slowly rising currents |
This shift to the right in the SD curve is the hallmark sign of denervation and is the basis for clinical testing of the orbicularis oculi in facial nerve palsy.
Anatomy of Orbicularis Oculi (Relevant to SD Testing)
The orbicularis oculi is a sphincter muscle surrounding the orbit with three functional portions:
- Orbital part — forceful voluntary closure
- Pretarsal/palpebral part — involuntary blinking, involved in the blink reflex
- Lacrimal part — lacrimal pump
It is innervated by the facial nerve (CN VII) — zygomatic and temporal branches. The blink reflex (orbicularis oculi reflex) is mediated partly by trigeminal pathways.
Practical Application of SD Curve to Orbicularis Oculi
1. Diagnosis of Facial Nerve (CN VII) Palsy / Denervation
- The SD curve is used to assess the degree of denervation of the orbicularis oculi in Bell's palsy, trauma, or surgical injury to CN VII
- A right-shifted curve with prolonged chronaxie indicates partial or complete denervation
- Helps distinguish neuropraxia (intact axon — normal/near-normal curve) from axonotmesis/neurotmesis (denervated curve)
- Serial SD testing tracks reinnervation progress — as the curve shifts back toward normal, reinnervation is occurring
2. Electrotherapy / Neuromuscular Electrical Stimulation (NMES)
- In denervated orbicularis oculi, the pulse duration must be set longer (based on the SD curve) to achieve muscle contraction without stimulating intact nearby nerves
- Typical denervated muscle stimulation: pulse widths of 10–300 ms (vs. 0.1–1 ms for normal nerve)
- The SD curve guides selection of pulse width and intensity for therapeutic electrical stimulation to:
- Maintain muscle bulk during denervation
- Prevent fibrosis
- Aid recovery after facial nerve palsy
3. Blepharospasm Assessment
- SD testing can map the excitability of orbicularis oculi in blepharospasm (involuntary bilateral spasm)
- Helps guide the appropriate site and extent of botulinum toxin injection
4. Monitoring After Surgery
- Used intraoperatively and postoperatively to monitor facial nerve function during parotidectomy, acoustic neuroma surgery, and other skull base procedures
- A 5-channel facial nerve recording montage with electrodes placed in frontalis, orbicularis oculi, nasalis, orbicularis oris, and mentalis muscles is standard — Cummings Otolaryngology
Botulinum Toxin (BoNT-A) Applications & Doses for Orbicularis Oculi
The SD curve assessment informs whether electrotherapy or BoNT-A is appropriate. Botulinum toxin is used when the orbicularis oculi is overactive (blepharospasm, crow's feet, hypertrophy):
| Indication | Injection Sites | Dose (onabotulinumtoxinA) |
|---|---|---|
| Crow's feet (lateral canthal rhytides) | 2–4 sites lateral to orbital rim | 12–15 U/side |
| Blepharospasm | 3–4 periocular subcutaneous sites | 2.5–5 U per site (~10–20 U total per eye) |
| Hypertrophic orbicularis oculi | Subcutaneous, midpupillary line, 3 mm below ciliary margin | 2–4 U |
| Hemifacial spasm | Periocular sites (same as blepharospasm) | Similar to blepharospasm |
"Botulinum toxin injection (e.g. 2.5–5 units injected subcutaneously at 3–4 periocular sites) affords relief in most (95%) patients by temporary paralysis of the injected muscles; typically, repeat injections are required every 3 months." — Kanski's Clinical Ophthalmology
Key precautions for orbicularis oculi BoNT-A:
- Higher doses → risk of ptosis, lagophthalmos, dry eye, diplopia
- Inject lateral to the orbital rim for crow's feet — medial injections risk lower eyelid droop
- Keratoconjunctivitis sicca (dry eye) risk with pretarsal doses >4 U
- Inject when patient is not smiling to avoid affecting the zygomaticus complex (upper lip ptosis risk)
Summary: SD Curve Parameters in Practice
| Parameter | Innervated Orbicularis | Denervated Orbicularis | Clinical Use |
|---|---|---|---|
| Rheobase | ~1–2 mA | Higher | Baseline excitability |
| Chronaxie | ~0.7–1 ms | >10 ms (up to 100 ms) | Degree of denervation |
| Curve position | Left (steep) | Right (flattened) | Serial monitoring |
| Therapeutic pulse width | 0.1–1 ms | 10–300 ms | NMES parameter setting |
References:
- Medical Physiology (Boron & Boulpaep), p. 276–277
- Ganong's Review of Medical Physiology, 26th Ed., p. 101
- Dermatology 5e (Bolonia et al.), p. 3192–3194
- Kanski's Clinical Ophthalmology, 10th Ed., p. 854
- Cummings Otolaryngology – Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.