Explain brachial plexus
Reading File
Finding Sources
Searching the Web
brachial plexus anatomy roots trunks divisions cords branches
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Let me compose it:
Brachial Plexus
The brachial plexus is a somatic nerve plexus that provides virtually all motor and sensory innervation to the upper limb. It originates in the neck, courses over the first rib, and enters the axilla.
1. Overview
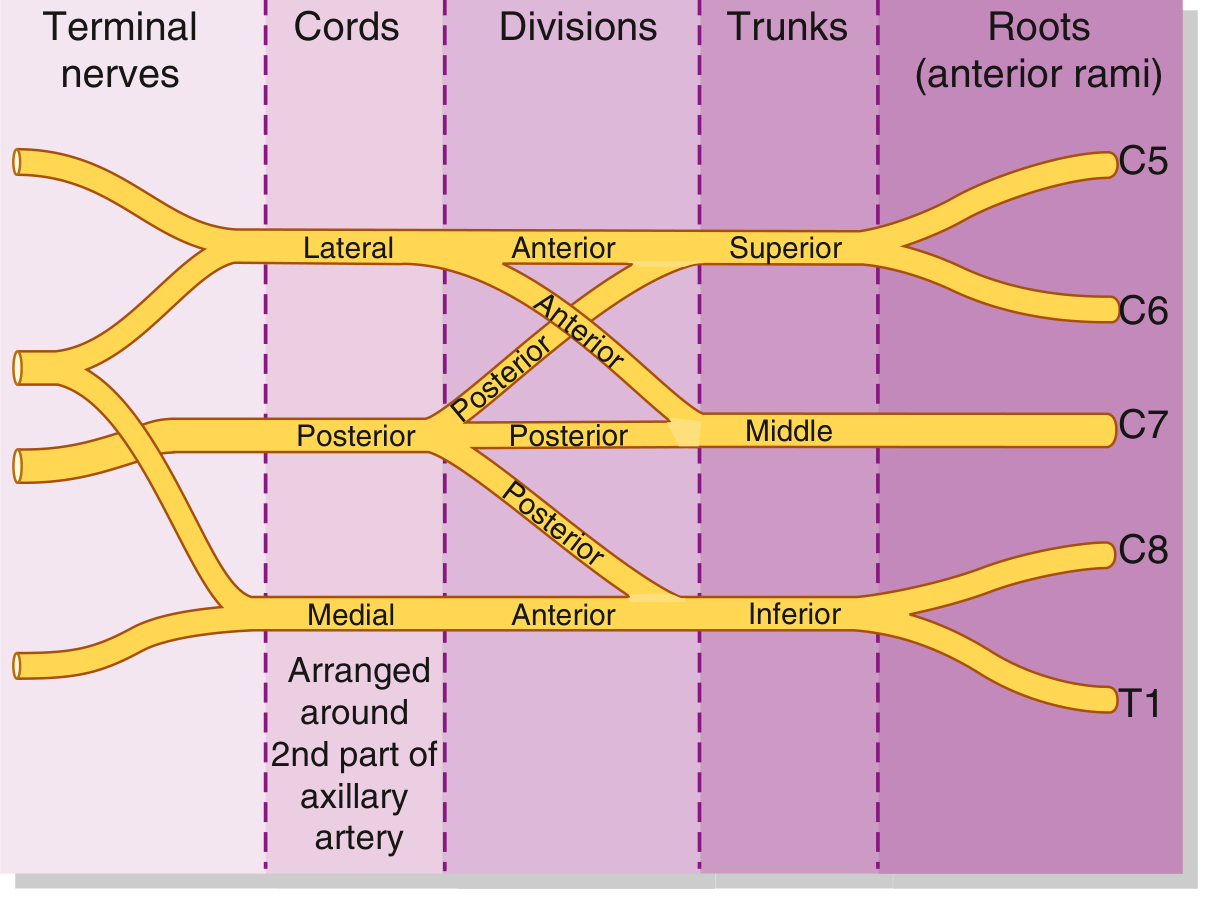
The plexus is formed by the anterior rami of C5, C6, C7, C8, and T1. Occasionally C4 contributes (prefixed plexus) or T2 contributes (postfixed plexus). The organization from proximal to distal follows a strict sequence: Roots → Trunks → Divisions → Cords → Branches.
Mnemonic: Robert Taylor Drinks Cold Beer (Roots, Trunks, Divisions, Cords, Branches)
2. Schematic Diagram
From Gray's Anatomy for Students:
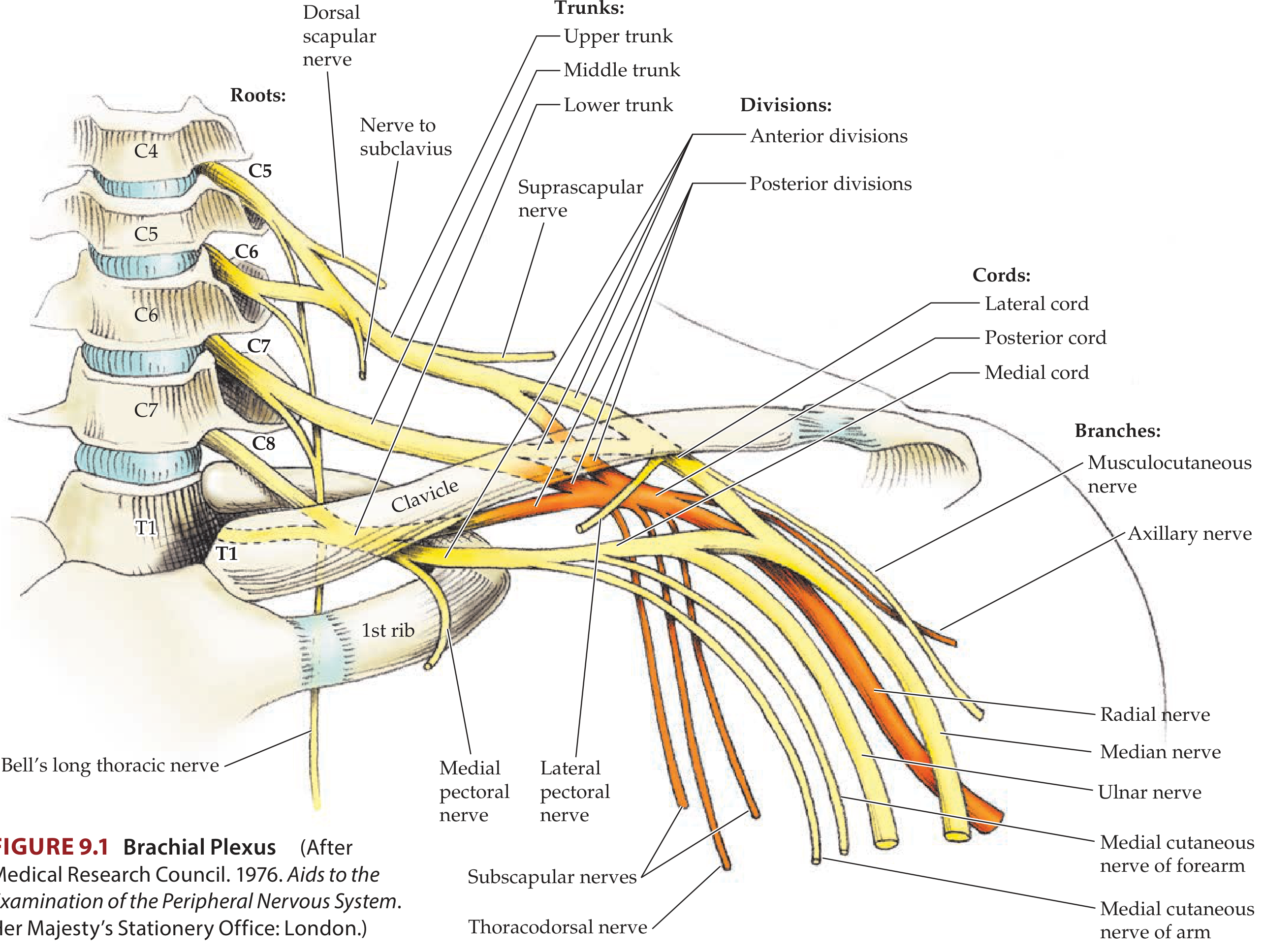
From Neuroanatomy through Clinical Cases (Fig. 9.1) — anatomical illustration with all branches labeled:
3. Components in Detail
A. Roots (C5–T1)
- The anterior rami of spinal nerves C5–T1 form the roots.
- They emerge between the anterior scalene and middle scalene muscles.
- Each root receives gray rami communicantes from the sympathetic trunk, carrying postganglionic sympathetic fibers to the periphery.
- The roots + trunks lie superior and posterior to the subclavian artery in the posterior triangle of the neck.
Branches from roots:
| Nerve | Root(s) | Supplies |
|---|---|---|
| Dorsal scapular nerve | C5 | Rhomboid major & minor |
| Long thoracic nerve | C5, C6, C7 | Serratus anterior |
| Contribution to phrenic nerve | C5 | Diaphragm (partial) |
B. Trunks
The three trunks cross the base of the posterior triangle over rib I:
| Trunk | Formed from |
|---|---|
| Superior (upper) trunk | C5 + C6 |
| Middle trunk | C7 alone |
| Inferior (lower) trunk | C8 + T1 |
Branches from trunks (only from the superior trunk):
- Suprascapular nerve (C5, C6) - innervates supraspinatus and infraspinatus
- Nerve to subclavius (C5, C6) - innervates the subclavius muscle
C. Divisions
Each trunk splits into an anterior and a posterior division behind the clavicle:
- Anterior divisions → supply flexor (anterior) compartments
- Posterior divisions → supply extensor (posterior) compartments
- No peripheral nerves originate directly from the divisions themselves.
D. Cords
The cords are named for their position relative to the 2nd part of the axillary artery:
| Cord | Formed from | Root levels | Position |
|---|---|---|---|
| Lateral cord | Anterior divisions of superior + middle trunks | C5, C6, C7 | Lateral to axillary artery |
| Medial cord | Anterior division of inferior trunk | C8, T1 | Medial to axillary artery |
| Posterior cord | All three posterior divisions | C5 → T1 (all levels) | Posterior to axillary artery |
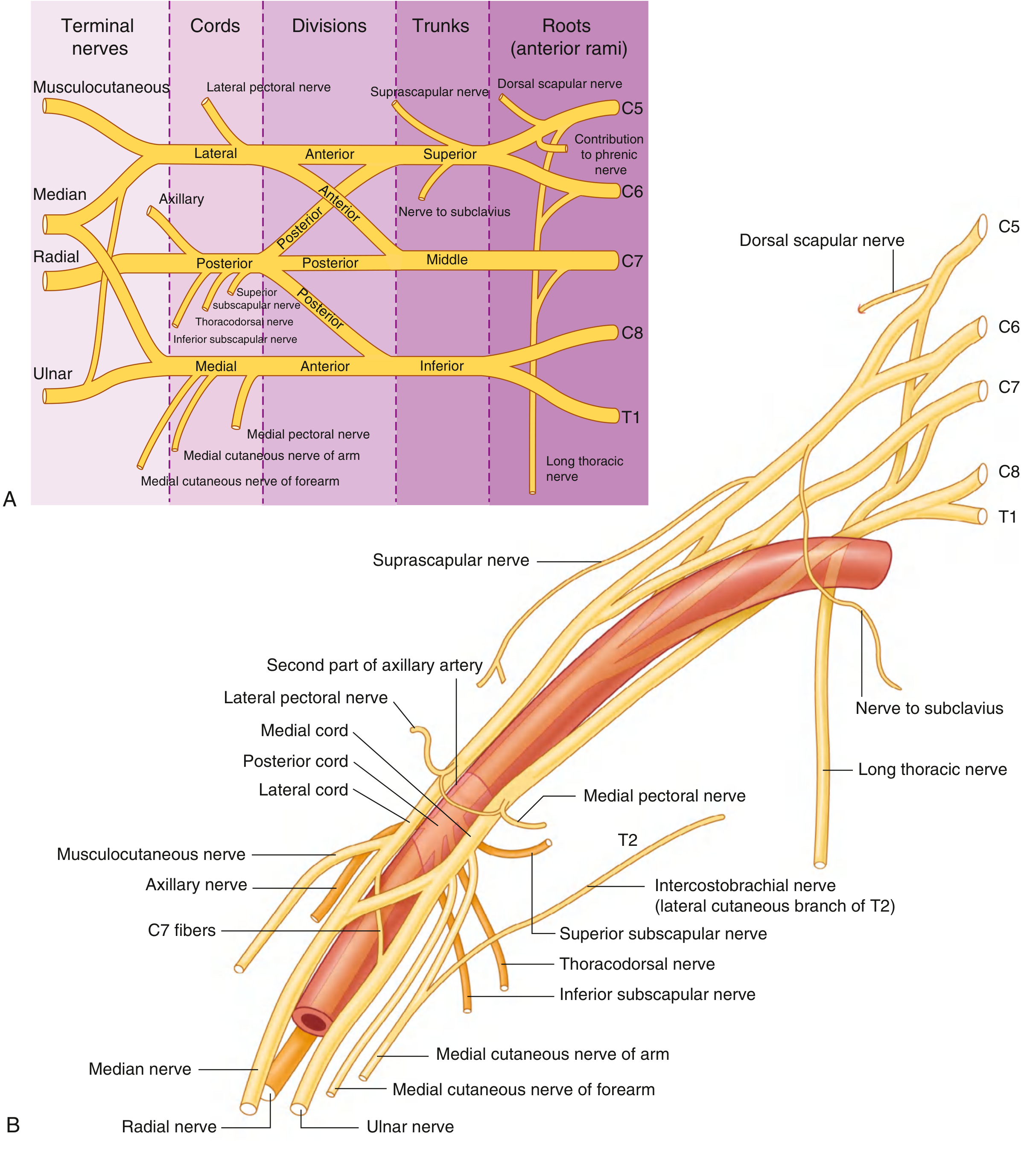
E. Terminal Branches (from Cords)
Full branches diagram from Gray's Anatomy for Students:
From the Lateral Cord:
| Branch | Function |
|---|---|
| Lateral pectoral nerve | Pectoralis major (and minor via communicating loop) |
| Musculocutaneous nerve | Biceps brachii, brachialis, coracobrachialis; terminates as lateral cutaneous nerve of forearm |
| Lateral root of median nerve | Contributes to median nerve |
Mnemonic for musculocutaneous targets: BBC - Biceps, Brachialis, Coracobrachialis
From the Medial Cord:
| Branch | Function |
|---|---|
| Medial pectoral nerve | Pectoralis minor and major |
| Medial cutaneous nerve of arm | Skin, medial distal arm |
| Medial cutaneous nerve of forearm | Skin, medial forearm to wrist |
| Medial root of median nerve | Contributes to median nerve |
| Ulnar nerve | All intrinsic hand muscles (except 3 thenar + 2 lateral lumbricals); flexor carpi ulnaris; medial half of FDP; medial hand/finger skin |
From the Posterior Cord:
| Branch | Function |
|---|---|
| Upper subscapular nerve | Subscapularis (upper part) |
| Thoracodorsal nerve | Latissimus dorsi |
| Lower subscapular nerve | Subscapularis (lower part) + teres major |
| Axillary nerve | Deltoid, teres minor; lateral cutaneous nerve of arm |
| Radial nerve | All posterior compartment muscles of arm and forearm; skin of posterior arm, forearm, and dorsum of hand |
Mnemonic for posterior cord branches: STAR (or ARTS) - Subscapular (upper & lower), Thoracodorsal, Axillary, Radial
The Median Nerve (special case):
Forms anterior to the 3rd part of the axillary artery from the lateral root (lateral cord) + medial root (medial cord), creating the characteristic "M or W shape" with the musculocutaneous nerve, lateral cord, median nerve, medial cord, and ulnar nerve in the axilla.
4. Relations and Course
| Region | Relation |
|---|---|
| Between scalenes (neck) | Roots pass between anterior and middle scalene muscles |
| Posterior triangle | Trunks cross; suprascapular nerve and long thoracic nerve visible |
| Behind clavicle | Divisions pass posterior to clavicle |
| Axilla | Cords surround the 2nd part of axillary artery |
| Lateral border of pectoralis minor | Cords divide into terminal branches |
5. Clinical Injuries
Erb-Duchenne Palsy (Upper Brachial Plexus Palsy)
- Roots involved: C5 and C6
- Mechanism: Excessive lateral flexion of the neck away from the shoulder (downward force on shoulder) - occurs in difficult delivery (shoulder dystocia), motorcycle accidents, or falls
- Muscles paralyzed: Deltoid, biceps, brachialis, brachioradialis, supinator
- Posture: Arm hangs internally rotated, elbow extended, forearm pronated - classic "waiter's tip" or "policeman taking a tip" position
- Sensory loss: Lateral arm and upper forearm (C5, C6 dermatomes)
- Prognosis: Best among partial lesions - most common type
Klumpke's Palsy (Lower Brachial Plexus Palsy)
- Roots involved: C8 and T1 (T1 more commonly)
- Mechanism: Forceful hyperabduction of the arm - breech delivery with arms above head, grabbing overhead support during a fall
- Muscles paralyzed: All intrinsic hand muscles (combined median + ulnar pattern) → claw hand
- Sensory loss: Medial forearm, hand, and medial 1½ fingers
- Horner's syndrome: Associated ptosis, miosis (pupil constriction), enophthalmos, and anhidrosis on the affected face - due to disruption of preganglionic sympathetic fibers from T1
- Prognosis: Poor
Total Brachial Plexus Palsy (C5–T1)
- Mechanism: Severe trauma (high-speed accidents)
- Result: Complete flaccid paralysis and anesthesia of the entire upper limb (except upper medial arm - intercostobrachial nerve from T2 is spared)
- Prognosis: Worst
Supraclavicular vs. Infraclavicular Injuries
- Supraclavicular (roots and trunks) - more severe, worse prognosis, often avulsion injuries
- Infraclavicular (cords and terminal nerves) - better prognosis, more amenable to surgical repair
6. Summary Table
| Level | Components | Key Branches |
|---|---|---|
| Roots | C5, C6, C7, C8, T1 | Dorsal scapular, long thoracic, phrenic contribution |
| Trunks | Superior (C5,6), Middle (C7), Inferior (C8,T1) | Suprascapular, nerve to subclavius |
| Divisions | Anterior × 3, Posterior × 3 | None directly |
| Cords | Lateral, Medial, Posterior | All terminal nerves |
| Branches | 5 terminal nerves | Musculocutaneous, Axillary, Radial, Median, Ulnar |
Sources: Gray's Anatomy for Students (Fig. 7.52, 7.53, 7.55); Neuroanatomy through Clinical Cases 3rd Ed. (Fig. 9.1); S Das Manual on Clinical Surgery 13th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.