Triple deformity of knee etiology pathology and signs and symptoms causes and mechanism investigation and treatment explain in detail with appropriate illustrative diagrams and images
triple deformity knee etiology pathology signs symptoms treatment orthopedics
https://www.relainstitute.com/articles/triple-deformity-of-t…
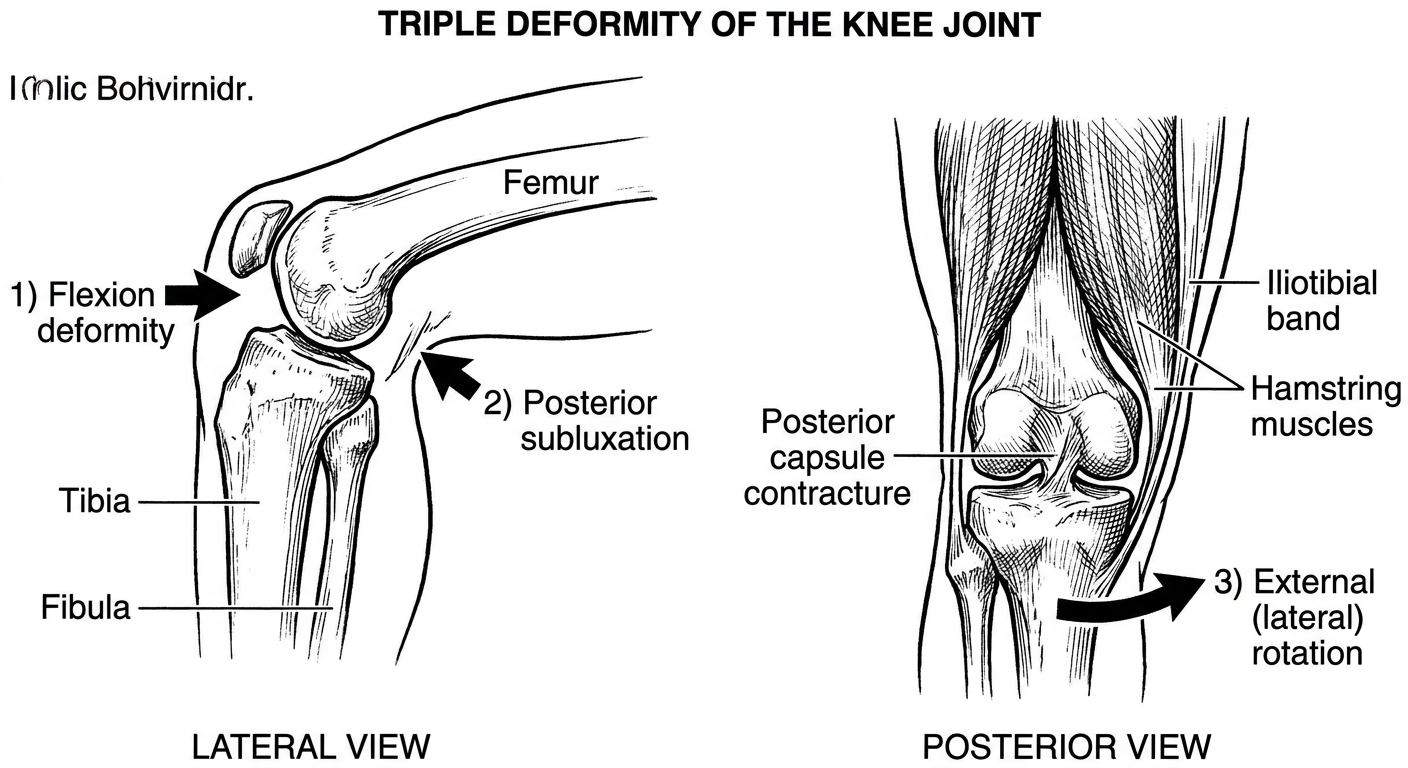
Medical diagram showing triple deformity of the knee joint - labeled anatomical illustration showing three components: 1) Flexion deformity of knee joint, 2) Posterior subluxation of tibia on femur, 3) External (lateral) rotation of tibia. Show the knee from lateral and posterior views with clear arrows indicating each deformity direction. Include annotation labels for femur, tibia, fibula, posterior capsule contracture, iliotibial band, and hamstring muscles. Educational medical textbook style, black and white with clear labels.
Triple Deformity of the Knee
Definition
- Flexion deformity of the knee joint
- Posterior subluxation of the tibia on the femur
- External (lateral) rotation of the tibia
Schematic Diagram of Triple Deformity
Etiology (Causes)
| Cause | Mechanism |
|---|---|
| Tuberculosis of the knee (most classic) | Hematogenous seeding - synovium or metaphysis/epiphysis; leads to pannus, cartilage destruction, and ligamentous laxity |
| Rheumatoid arthritis | Chronic synovitis, pannus formation, cartilage and bone erosion, capsular/ligamentous stretching |
| Poliomyelitis | Muscle paralysis (hamstrings, quadriceps imbalance) - gravity-assisted deformity |
| Iliotibial band contracture | The tight ITB acts as a bowstring producing flexion + external rotation |
| Septic (pyogenic) arthritis - late untreated | Joint destruction, fibrous ankylosis |
| Hemophilic arthropathy | Repeated hemarthrosis - low clotting capacity leads to synovial hypertrophy and joint destruction |
| Neuropathic (Charcot) joint | Loss of pain sensation - repeated undetected trauma leading to progressive destruction |
Pathology
Stages of Tuberculous Knee (the model disease for triple deformity)
- Mycobacterium tuberculosis seeds the synovial membrane via hematogenous spread
- Granuloma formation with epithelioid cells, Langhans giant cells, lymphocytes, and central caseation
- Synovial hypertrophy and effusion develop (boggy, doughy swelling - "white swelling" or "cold swelling")
- Pannus (vascular granulation tissue) forms and begins to creep over the articular cartilage
- Joint space is preserved or slightly widened (effusion)
- No articular cartilage destruction yet
- Pannus invades and erodes articular cartilage from the periphery inward
- "Kissing lesions" - cartilage destroyed from both surfaces simultaneously
- Marginal erosions appear; osteolytic foci develop in periarticular bone
- Joint space narrows progressively
- Night pain is characteristic at this stage
- Complete destruction of articular cartilage; bone exposed
- Severe periarticular muscle wasting (especially quadriceps)
- Ligamentous laxity and capsular fibrosis develop simultaneously
- Massive joint destruction with virtually no joint space
- Triple deformity becomes clinically evident:
- Flexion: posterior capsule and hamstring contracture
- Posterior subluxation: gravity + capsular destruction allows tibia to slip backward
- External rotation: contracture of the iliotibial band, which acts as a bowstring along the lateral aspect, pulling the tibia into external rotation
- Cold abscess and sinuses may form; melon seed bodies (rice bodies) may be found in joint fluid
Mechanism of Formation
How Each Component Develops:
- Joint effusion causes reflex spasm of the hamstrings (flexors), holding the knee slightly flexed (the position of maximum joint volume - ~25° flexion)
- Prolonged flexion leads to shortening of the posterior capsule and hamstring tendons
- Quadriceps wasting removes the antagonist pull
- Result: fixed flexion contracture
- Articular destruction and ligamentous laxity (especially posterior cruciate ligament involvement)
- In the flexed position, gravity and body weight act on the tibia, pulling it posteriorly on the femoral condyles
- The flexed posture with weight bearing causes the tibia to progressively sublux backward
- On lateral X-ray: the tibia sits posterior to the normal alignment with the femoral condyles
- The iliotibial band (ITB) runs obliquely from the iliac crest to the lateral tibial condyle (Gerdy's tubercle)
- As the knee flexes and the posterior structures contract, the ITB - which cannot elongate - acts as a taut lateral bowstring
- It mechanically rotates the tibia externally relative to the femur
- This is further assisted by contracture of the biceps femoris (external rotator of the flexed knee)
Signs and Symptoms
Early Stage
- Limp - the first symptom noticed in children
- Aching pain around the knee, worse on activity
- Joint swelling - diffuse, boggy, doughy consistency ("white swelling" - no warmth or redness, unlike pyogenic)
- Slight flexion attitude - knee held in mild flexion
- Enlarged inguinal lymph nodes (popliteal nodes may also be enlarged but harder to palpate)
- Wasting of quadriceps - visible even early
Intermediate Stage
- Night pain - characteristic of tuberculosis (released muscle spasm during sleep causes sudden pain)
- Increasing stiffness of the joint
- Marked quadriceps wasting
- Effusion detectable on clinical examination (bulge sign, patellar tap)
- Restricted range of movements with pain on movement
Late Stage - Triple Deformity
- Visible deformity:
- Knee held in flexion
- Tibia pushed posteriorly
- Foot externally rotated
- Fixed flexion deformity - knee cannot be fully extended even passively
- Posterior fullness in the popliteal fossa (subluxed tibia)
- Severe quadriceps wasting - thigh appears grossly wasted
- Cold abscess - fluctuant, non-tender, non-warm swelling, may track along fascial planes
- Sinuses - discharging sinuses may develop in untreated cases
- Shortening of the limb - due to flexion deformity
- Positive four-finger test - examiner can place four fingers in the popliteal fossa due to posterior tibial shift
- General signs of tuberculosis: evening rise of temperature, night sweats, weight loss, anorexia, pallor
X-Ray Findings (Investigations)
Radiological Progression
- Generalized or localized decalcification (osteoporosis) around the joint
- Increased joint space (effusion)
- Periarticular soft tissue swelling
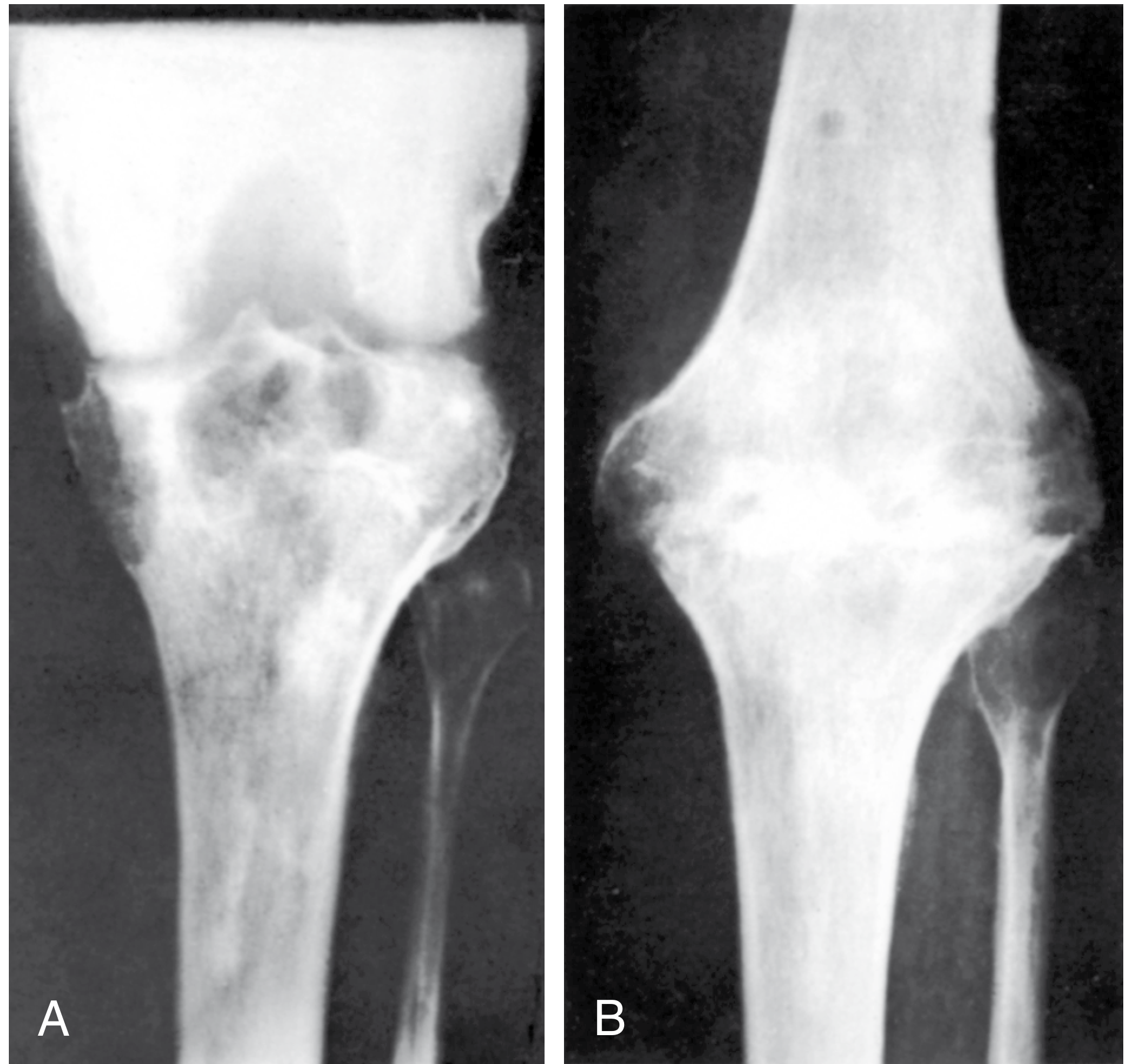
- Diminished joint space (cartilage destruction)
- Irregular joint line ("moth-eaten" appearance)
- Marginal erosions and periarticular bony foci
- Practically no joint space remaining
- Posterior subluxation of tibia visible on lateral view (posterior tibial shift - confirmed by drawing dotted line along posterior surface of femoral condyles)
- External rotation of tibia visible on AP view
- Flexion deformity visible clinically and on lateral view
- Generalized severe osteoporosis
- Possible collapse/destruction of femoral condyles or tibial plateau
X-Ray - Triple Deformity (S Das, 13th Ed.)
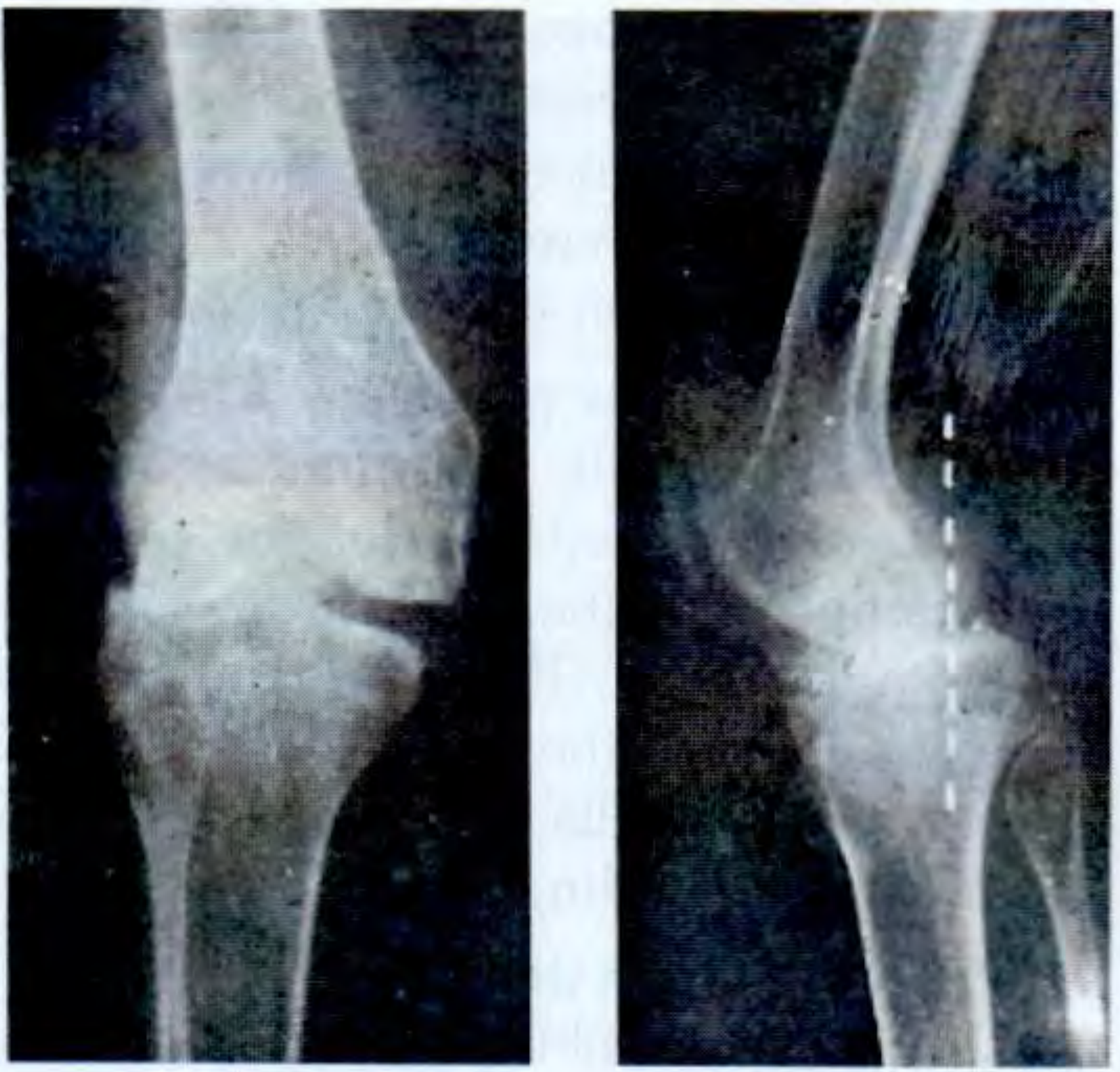
X-Ray - TB Knee Before and After Arthrodesis (Campbell's Operative Orthopaedics, 15th Ed.)
Other Investigations
| Investigation | Findings in TB Knee |
|---|---|
| Blood | ESR elevated, CRP raised, mild anaemia, lymphocytosis |
| Mantoux (tuberculin) test | Positive (>10 mm induration); note: may be negative in immunocompromised |
| IGRA (Interferon Gamma Release Assay) | More specific than Mantoux |
| Joint aspiration (synovial fluid) | Straw-colored fluid, low glucose, high protein, high WBC (lymphocyte predominant), AFB smear/culture |
| Synovial biopsy | Most definitive - shows epithelioid granulomas with Langhans giant cells and caseation necrosis |
| X-ray (AP + lateral) | As described above |
| MRI | Best for early disease - shows synovial thickening, effusion, marrow edema, cartilage loss, soft tissue involvement |
| CT scan | Better for bony erosions, sequestrum detection |
| Chest X-ray | To detect pulmonary TB (primary focus) |
| Sputum AFB / CBNAAT (GeneXpert) | To confirm TB elsewhere |
| Arthrography | Contrast medium (Conray/Urografin) or air - helpful for internal derangement assessment |
| Arthroscopy | Direct visualization + biopsy; allows arthroscopic synovectomy |
Treatment
I. Medical (Antitubercular Therapy - ATT)
| Phase | Drugs | Duration |
|---|---|---|
| Intensive phase | Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) | 2 months |
| Continuation phase | Isoniazid (H) + Rifampicin (R) | 4-7 months (total 6-9 months for bone/joint TB) |
II. Conservative / Non-Surgical
- Rest and immobilization - posterior splint or POP cast to rest the joint in functional position
- A knee with a normal-appearing radiograph or mildly confined osteomyelitic changes frequently responds to multidrug chemotherapy; these patients may tolerate early range-of-motion and mobilization procedures - Campbell's, p.8029
- Physiotherapy - quadriceps strengthening, gentle ROM exercises once inflammation subsides
- Traction - skin or skeletal traction to correct early flexion deformity and relieve muscle spasm
- Serial plastering - gradual correction of deformity by progressive plaster casts
III. Surgical Treatment
- Repeated aspiration of joint fluid relieves tension pain
- Abscess: drained; localized bone lesion: curetted - Campbell's, p.8026
- Indicated in persistent synovitis not responding to chemotherapy
- Can be done open or arthroscopically (less morbidity)
- Removes the infected pannus and granulation tissue
- Best results in stage 1 (pre-arthritic stage)
- Partial synovectomy described by Wilkinson (1962) for TB knee - Campbell's, p.9277
- For localized bone lesions with sequestrum
- Curettage of adjacent bone lesion if distal femur or proximal tibia involved
- Gradual correction: Serial plasters / traction + ATT (for mild-moderate fixed flexion)
- Posterior capsulotomy: Release of tight posterior capsule for flexion contracture
- Hamstring lengthening: Surgical lengthening (recession or tenotomy) to correct flexion
- Iliotibial band release: Division/lengthening of ITB to correct external rotation component
- Pre-arthroplasty: reduction of subluxation is always attempted before any arthroplasty
- Indicated for severe joint destruction with significant degenerative changes when a more aggressive open approach is needed - Campbell's, p.8051
- Provides a pain-free, stable, weight-bearing limb (though with no movement)
- Preferred in young patients with single-joint disease where arthroplasty is inappropriate
- Immobilization in a long-leg cast post-operatively
- Results in solid fusion typically within months (see X-ray above: Figure 25.11)
- Considered in older patients with end-stage disease
- Technically challenging due to posterior subluxation in triple deformity; subluxation must be reduced before arthroplasty can be performed
- Limited success described; risk of reactivation of quiescent TB process is a concern
- Must be preceded by at least 6 months of ATT; some recommend 1-2 years of disease quiescence
- Gaining knee flexion is considered the main goal of rehabilitation following surgery - Relainstitute
Treatment Summary Flowchart:
Triple Deformity of Knee
|
v
Start ATT (all stages)
|
+---> Early disease (Stage 1-2, no/mild deformity)
| -> Rest + Immobilization + Physiotherapy
| -> Arthroscopic/open synovectomy if no ATT response
|
+---> Moderate disease (Stage 2, early deformity)
| -> Serial plaster + traction to correct deformity
| -> Posterior capsulotomy + hamstring release
| -> Synovectomy + sequestrectomy
|
+---> Advanced disease (Stage 3, full triple deformity)
-> Correction of deformity (ITB release, capsulotomy)
-> Young patient: Arthrodesis (fusion)
-> Older patient: TKR (after subluxation reduction)
Differential Diagnosis
- Acute pyogenic arthritis - warm, red, tender, rapid onset; high fever; synovial fluid shows neutrophilia
- Osteoarthritis - disease of old age; bony swelling; osteophytes on X-ray; no lymphadenopathy
- Rheumatoid arthritis - bilateral, morning stiffness, RF positive; pannus formation; can also cause triple deformity in late stage
- Charcot (neuropathic) joint - associated with diabetes, tabes dorsalis; marked hypermobility; bizarre X-ray destruction
- Haemophilic arthropathy - young males; history of bleeding disorder; episodic hemarthrosis
- Gout/pseudogout - acute attacks; crystal analysis of synovial fluid diagnostic
Key Clinical Pearls
- Triple deformity = flexion + posterior subluxation + external rotation - all three must be present
- It is a late/end-stage sign, classically of tuberculosis of the knee
- The iliotibial band is the key structure responsible for the external rotation component (acts as a lateral bowstring)
- The "four-finger test" (palpation of posteriorly subluxed tibia) is a bedside sign
- "Night pain" is a hallmark of stage 2 (arthritic) TB knee - pain on movement diminishes at rest, but released muscle spasm during sleep wakes the patient
- X-ray: Always draw a line along the posterior femoral condyles on the lateral view to demonstrate posterior tibial subluxation
- ATT is the backbone of treatment - surgery is adjunctive
- TKR is technically difficult because of the subluxation and must be planned carefully
- S Das, A Manual on Clinical Surgery, 13th Edition, pp. 257-258
- Campbell's Operative Orthopaedics, 15th Ed. 2026, pp. 8026-8058
- Rela Institute, Triple Deformity of the Knee: Treatment and Prevention