Endocrine hypertension
Reading File
Finding Sources
Finding Sources
Searching PubMed
"endocrine hypertension" diagnosis management
Reading File
Reading File
Searching PubMed
"primary aldosteronism" OR "pheochromocytoma" OR "Cushing syndrome" hypertension
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from authoritative textbooks, two key diagnostic flowcharts, and recent PubMed guidelines. I have enough to write a thorough response.
Endocrine Hypertension
Endocrine causes make up over 20% of all secondary hypertension cases - yet they are frequently undiagnosed because many patients lack obvious signs or symptoms. Identifying them matters because the hypertension is often curable or substantially improved by treating the underlying endocrine disorder.
Overview & Classification
The main endocrine causes, in approximate order of prevalence:
| Cause | Prevalence Among Hypertensives | Key Mechanism |
|---|---|---|
| Primary aldosteronism | 5-20% of all hypertension | Autonomous aldosterone excess → Na retention, K+ wasting |
| Pheochromocytoma/Paraganglioma | 0.1-0.6% | Catecholamine excess → vasoconstriction, ↑CO |
| Cushing syndrome | 0.5-1% | Cortisol excess → ↑CO, ↑TPR, Na retention |
| Hypothyroidism | ~40% have diastolic HTN | ↑SVR, ↓compliance |
| Hyperthyroidism | Systolic dominant | ↑CO, wide pulse pressure |
| Primary hyperparathyroidism | Up to 70% | ↑cytosolic Ca²⁺ → ↑SVR, renal vasoconstriction |
| Acromegaly | Common | GH/IGF-1-mediated, usually mild |
| Renin-secreting tumor | Rare (<200 cases) | Autonomous renin → Ang II → secondary hyperaldosteronism |
| Obstructive sleep apnea | Very common; ~73% in resistant HTN | Sympathetic activation, nocturnal + diurnal BP elevation |
1. Primary Aldosteronism (PA)
The most common endocrine cause of hypertension - up to 1 in 5 patients investigated for hypertension. Twice as common in women.
Pathophysiology
Autonomous aldosterone secretion, independent of the renin-angiotensin axis. Aldosterone acts on the mineralocorticoid receptor (MR) in the collecting duct to retain sodium and excrete potassium, raising plasma volume and BP. Excess aldosterone also causes direct cardiovascular inflammation, fibrosis, and hypertrophy independent of BP.
Subtypes:
- Aldosterone-producing adenoma (APA / Conn adenoma) - unilateral, surgical cure possible
- Bilateral idiopathic adrenal hyperplasia (BAH) - medical management
- Unilateral adrenal hyperplasia, glucocorticoid-remediable aldosteronism (rare familial form)
Who to Screen
- Hypertension with spontaneous or easily provoked hypokalemia
- Resistant/refractory hypertension (not controlled on ≥3 agents)
- Early-onset hypertension
- Hypertension + atrial fibrillation
- Known adrenal adenoma + hypertension
- Family history of PA or early stroke
- Key point: absence of hypokalemia does NOT exclude PA - most patients are normokalemic
Screening Test: Aldosterone-Renin Ratio (ARR)
- Measured on a random morning sample (diurnal variation matters)
- ARR >20 with plasma aldosterone >15 ng/dL supports PA (some labs use ARR >200 ng/dL per ng/mL/h)
- Test is 70-90% sensitive and 70-100% specific
- Medications to consider holding: MR blockers (spironolactone, eplerenone), diuretics, beta-blockers, ACEi/ARBs - though this is complex (see below)
Confirmatory Testing
When ARR is borderline (25-50), confirmatory testing is required: oral sodium loading, saline infusion, fludrocortisone suppression test, or captopril challenge.
Localization
- CT adrenal (thin 1 mm slices) - first step after biochemical confirmation
- Adrenal vein sampling (AVS) - the definitive test for lateralization (unilateral vs bilateral); technically demanding, should be done at specialized centers
- Selectivity index confirms successful cannulation (>2 unstimulated, >5 stimulated)
- Lateralization index (LI) determines unilateral vs bilateral disease
Treatment
- Unilateral disease (APA): laparoscopic adrenalectomy - cures hypertension in many patients
- Bilateral disease (BAH): MR antagonists - spironolactone (first-line) or eplerenone (fewer anti-androgenic side effects)
Diagnostic algorithm:
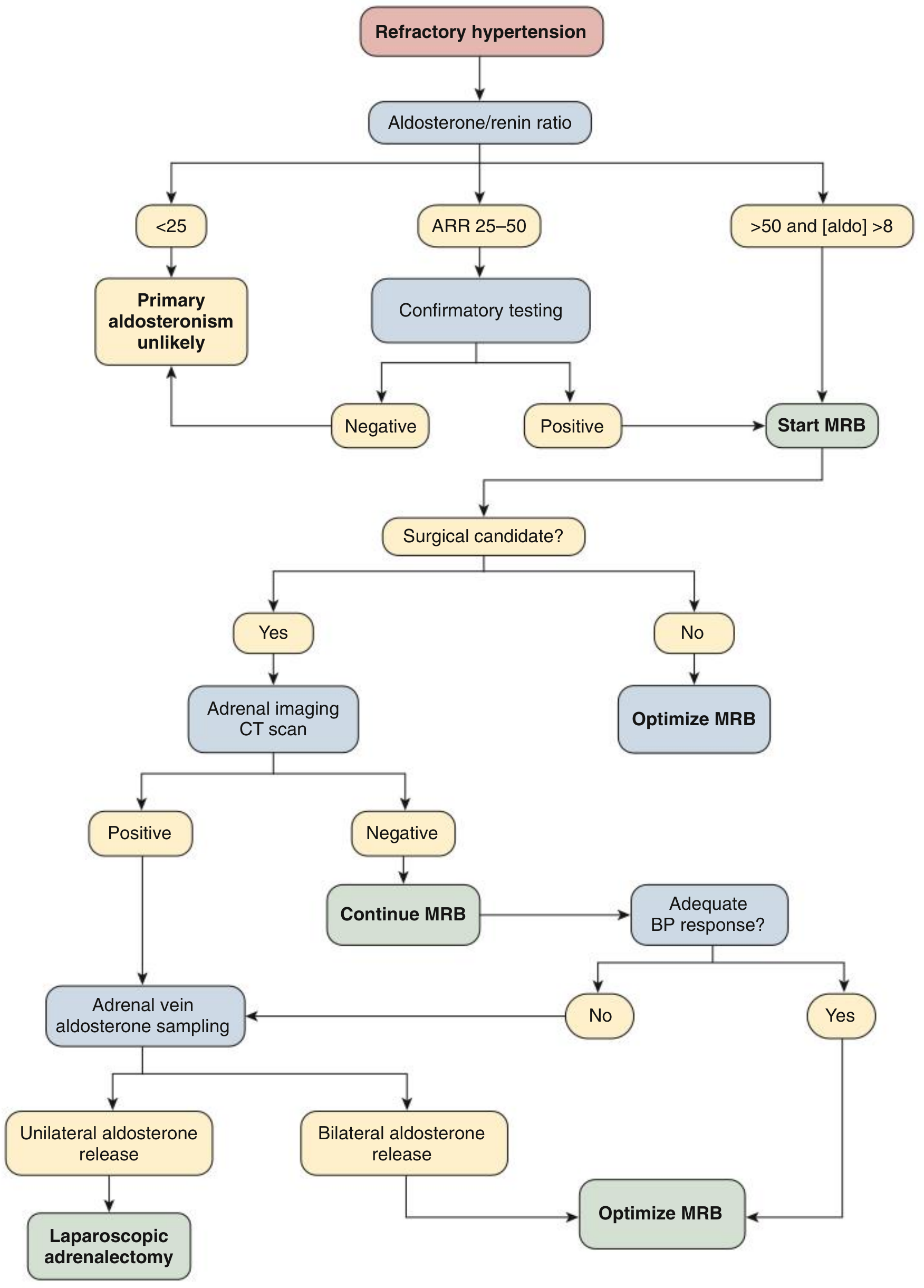
Fig. 39.6 - Comprehensive Clinical Nephrology, 7th Edition
2025 Update: The Endocrine Society issued an updated Clinical Practice Guideline on Primary Aldosteronism (PMID 40658480) and a supporting systematic review (PMID 40658500) in August 2025.
2. Pheochromocytoma & Paraganglioma (PPGL)
Rare but potentially lethal if missed. Pheochromocytomas arise from the adrenal medulla; paragangliomas from extra-adrenal chromaffin tissue (most commonly in the retroperitoneum).
Clinical Features
The classic triad:
- Headache (often severe, pounding)
- Sweating (profuse, diaphoretic)
- Palpitations / tachycardia
Hypertension may be:
- Paroxysmal (classic) - episodic crises lasting 15 min to hours
- Sustained (in ~50%)
- Orthostatic (paradoxically, due to volume contraction)
Unexpected intraoperative hypertension during abdominal surgery is an important clue to undiagnosed pheo.
Who to Screen
- Classic triad (headache, sweating, palpitations) ± hypertension
- Adrenal incidentaloma on imaging
- Family history / known mutation (VHL, RET, NF1, SDH genes)
- Resistant hypertension with paroxysmal features
Biochemical Diagnosis
- First-line: plasma-free metanephrines (highest sensitivity ~97%)
- Alternative: 24-hour urine fractionated metanephrines and catecholamines
- Sample ideally drawn supine for ≥20 minutes (reduces false positives)
- Advanced CKD raises metanephrine levels - adjust interpretation accordingly
- Interfering medications to be aware of: acetaminophen, levodopa, MAO inhibitors, SSRIs, tricyclics, sympathomimetics, some beta-blockers, cocaine
Imaging (after biochemical confirmation)
- CT or MRI abdomen/pelvis - first-line (most PPGLs are adrenal or para-aortic)
- CT/MRI chest, neck, head if abdominal imaging negative
- ¹²³I-MIBG scan - reserved for negative cross-sectional imaging despite markedly elevated biochemistry, or metastatic disease staging
- ⁶⁸Ga-DOTATATE PET - superior for paragangliomas; increasingly preferred
Workup Flowchart
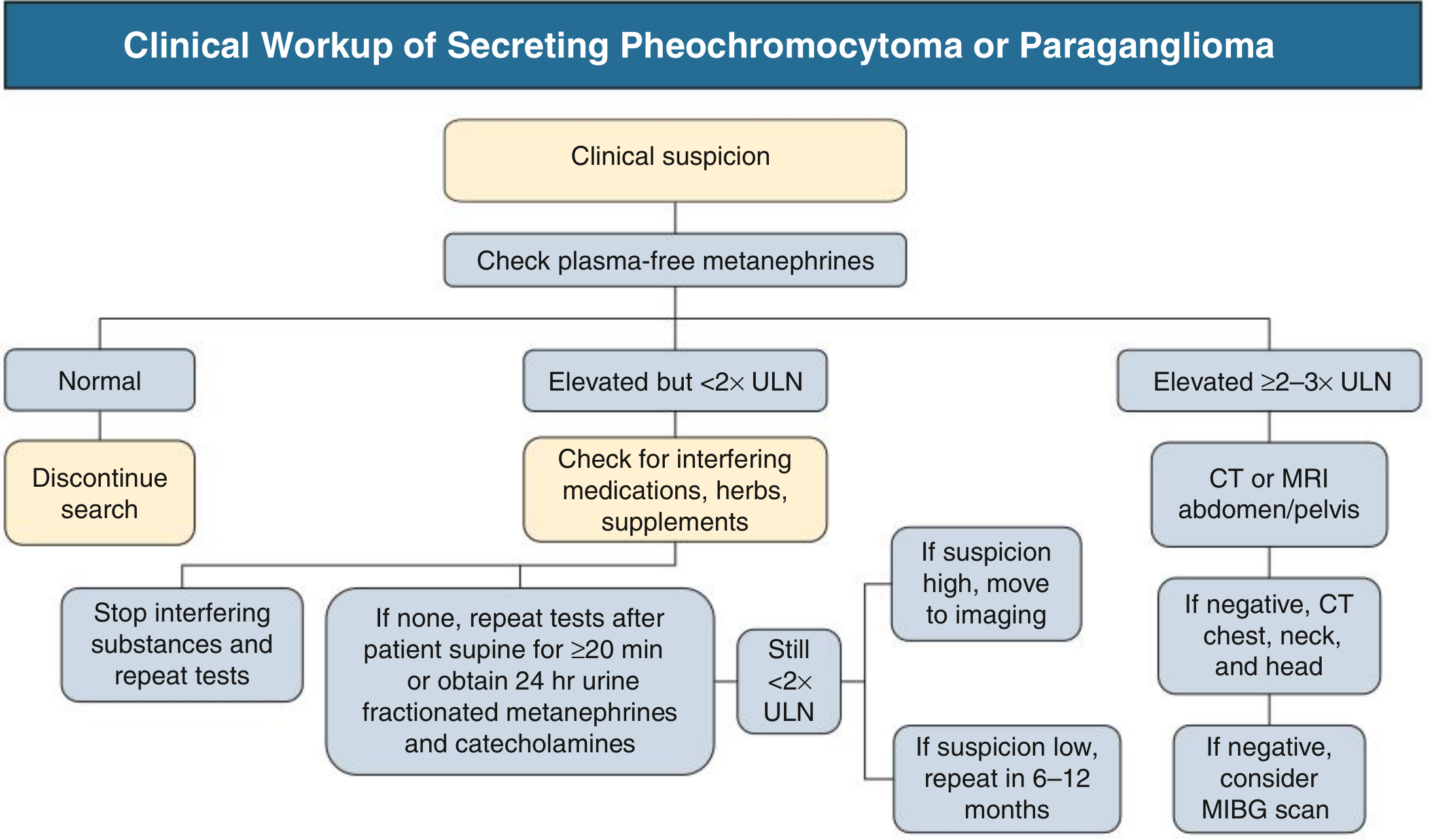
Fig. 40.5 - Comprehensive Clinical Nephrology, 7th Edition
Treatment
- Surgical excision after preoperative alpha-blockade (phenoxybenzamine or selective α₁-blockers)
- Beta-blockers added ONLY after alpha-blockade is established (adding beta-blocker first risks paradoxical hypertensive crisis by leaving alpha receptors unopposed)
- Biochemical follow-up at 6 months then annually; imaging annually for high-risk patients (large tumors, multifocal paragangliomas)
2026 Guideline: Japan Endocrine Society Clinical Practice Guideline for PPGL 2025 (PMID 41083371) - published Jan 2026.
3. Cushing Syndrome
Glucocorticoid excess from any source. Hypertension is present in ~80% of patients.
Causes
| Cause | Details |
|---|---|
| Cushing disease (pituitary adenoma secreting ACTH) | Most common endogenous cause; 4x more common in women |
| Adrenal adenoma / nodular hyperplasia / carcinoma | ACTH-independent |
| Ectopic ACTH | From neuroendocrine tumors (small cell lung Ca, bronchial/thymic carcinoids); tends to cause most severe HTN and hypokalemia |
| Exogenous steroids | Most common cause overall; HTN less prominent than endogenous |
Mechanisms of Hypertension
- Cortisol raises both cardiac output and total peripheral resistance
- At very high cortisol levels (especially ectopic ACTH), 11β-HSD2 is overwhelmed → cortisol binds mineralocorticoid receptors → pseudohyperaldosteronism → volume expansion and hypokalemia
- Cortisol inhibits vasodilatory nitric oxide
- Enhanced pressor responsiveness to catecholamines and angiotensin II
- Activation of cardiac and vascular MR → inflammatory, hypertrophic, and fibrotic changes
- Left ventricular hypertrophy disproportionate to BP level
Clinical Clues
Central adiposity, moon facies, buffalo hump, purple striae (≥1 cm wide, often abdominal), easy bruising, proximal myopathy, osteoporosis, glucose intolerance, hirsutism/acne. Ectopic ACTH: marked hyperpigmentation + severe hypokalemia + wasting disease.
Pearl: In a hypertensive patient with low aldosterone AND suppressed plasma renin activity, always consider glucocorticoid excess.
Diagnosis
Three first-line tests (any one or more):
- 24-hour urinary free cortisol (UFC) - elevated (>3-4x ULN is highly specific)
- Late-night salivary cortisol (×2) - loss of normal circadian nadir
- Overnight 1 mg dexamethasone suppression test - morning cortisol >1.8 mcg/dL is abnormal
Once hypercortisolism is confirmed, distinguish ACTH-dependent vs independent → plasma ACTH → pituitary MRI vs adrenal CT.
Treatment
- Cushing disease: transsphenoidal pituitary surgery
- Adrenal adenoma: laparoscopic adrenalectomy
- Ectopic ACTH: treat primary tumor ± bilateral adrenalectomy
- Successful treatment usually reduces BP, though hypertension may persist in some patients
4. Thyroid Disease
Hypothyroidism (~40% have hypertension)
- Predominantly diastolic HTN
- Mechanism: ↑systemic vascular resistance, ↓arterial compliance
- Narrow pulse pressure despite stiff vessels (low cardiac output)
- Subclinical hypothyroidism also associated with HTN
- Treatment of thyroid disease normalizes BP in most patients
Hyperthyroidism
- Predominantly systolic HTN
- Wide pulse pressure (↑CO + ↓SVR)
- Can mimic pheochromocytoma with paroxysmal features, flushing, palpitations
- Specific antithyroid treatment normalizes BP in most cases
5. Primary Hyperparathyroidism
- Up to 70% of patients with parathyroid adenoma have hypertension
- Mechanisms: ↑cytosolic calcium → ↑vascular resistance and ↑CO; hypercalcemia-induced renal vasoconstriction; kidney damage from hypercalciuria
- No direct correlation between serum Ca or PTH levels and BP
- Parathyroid adenoma resection cures or improves BP in most patients with new-onset HTN
6. Acromegaly
- Hypertension is common, though prevalence partly explained by age and sex
- GH and IGF-1 are implicated (BP decreases after successful treatment in many)
- BP elevations are seldom severe
7. Renin-Secreting Tumors
- Rare (<200 reported cases); most are benign renal juxtaglomerular cell tumors (2-4 cm)
- Classic presentation: young woman (<30 y), severe hypertension (~206/131 mmHg), hypokalemia (<3 mmol/L in 70%), proteinuria, occasionally hyponatremia
- Mechanism: autonomous renin → ↑Ang II → secondary hyperaldosteronism + direct vasoconstriction
- Diagnosis: elevated plasma renin/prorenin that normalizes after tumor removal, renin demonstrated within tumor
- Treatment: surgical resection
Adrenal Incidentaloma: The Triple Screen
Any adrenal incidentaloma in a hypertensive patient should be evaluated for:
- Pheochromocytoma - plasma-free metanephrines or 24-hr urine fractionated metanephrines
- Glucocorticoid excess - morning cortisol after 1 mg overnight dexamethasone
- Primary aldosteronism - plasma aldosterone and renin
- Malignancy risk - if non-contrast HU >10, >4-6 cm, or growing → surgical resection
Clinical Features Suggesting Endocrine Hypertension
| Feature | Think of... |
|---|---|
| Hypokalemia, low renin, high aldosterone | Primary aldosteronism |
| Paroxysmal HTN + headache + sweating + palpitations | Pheochromocytoma |
| Central obesity, purple striae, proximal myopathy | Cushing syndrome |
| Low aldosterone + suppressed renin | Cushing syndrome (cortisol activating MR) |
| Diastolic HTN, narrow pulse pressure, bradycardia | Hypothyroidism |
| Systolic HTN, wide pulse pressure, tremor, tachycardia | Hyperthyroidism |
| Hypercalcemia, kidney stones, bone pain | Primary hyperparathyroidism |
| Young woman with severe refractory HTN + hypokalemia | Renin-secreting tumor |
| Coarse facial features, large hands, macroglossia | Acromegaly |
| Resistant HTN + obesity + snoring | Obstructive sleep apnea |
Sources: Comprehensive Clinical Nephrology, 7th Edition (Ch. 39-40); National Kidney Foundation Primer on Kidney Diseases, 8e; Braunwald's Heart Disease; Robbins Pathologic Basis of Disease. Recent guidelines: Endocrine Society PA Guideline 2025 (PMID 40658480); Japan Endocrine Society PPGL Guideline 2025 (PMID 41083371).
This is a shared conversation. Sign in to Orris to start your own chat.