Potts spine 10 marks ms ortho
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative textbook content from Campbell's Operative Orthopaedics, Harrison's Principles of Internal Medicine, Adams & Victor's Neurology, and Rheumatology (Elsevier). I have all the information needed for a complete 10-mark MS Ortho answer.
Pott's Spine (Tuberculous Spondylitis) - MS Ortho 10 Marks
Definition
Pott's disease (tuberculous spondylitis) is the most common form of skeletal tuberculosis, representing infection of the vertebral column by Mycobacterium tuberculosis. It was first described by Sir Percival Pott in 1779 in a patient with paraplegia due to spinal TB. TB-induced spondylitis is one of the oldest recognized human infections, found in Egyptian and Peruvian mummies more than 5,000 years ago.
Epidemiology & Pathogenesis
- The vertebral column is affected in 50% of all skeletal TB cases
- Among weight-bearing joints: spine (40%), hips (13%), knees (10%)
- Spread is hematogenous (from primary pulmonary, genitourinary, or lymph node foci) or lymphogenous (especially thoracolumbar lesions)
- Two vertebral bodies and the intervening disc are typically affected as one unit
- Bacilli settle preferentially at the anterior superior or inferior angle of the vertebral body (rich blood supply, high oxygen requirement)
- Contiguous progression occurs via subligamentous burrowing under the anterior longitudinal ligament, spreading to adjacent vertebrae
Sites affected:
- Upper thoracic spine - more common in children
- Lower thoracic and upper lumbar vertebrae - more common in adults
- Cervical and sacral involvement is less common
Pathology
The sequence of destruction:
- Caseation and necrosis of vertebral body (anterior column first)
- Destruction of intervertebral disc (relatively late - unlike pyogenic osteomyelitis)
- Collapse and anterior wedging of vertebral body
- Gibbus deformity (sharp angular kyphosis) - the hallmark
- Cold abscess formation - pus without signs of acute inflammation
Cold abscess tracking:
| Level | Abscess track |
|---|---|
| Cervical | Retropharyngeal - presents as neck swelling or dysphagia |
| Upper thoracic | Paravertebral - tracks to chest wall as soft tissue mass |
| Lower thoracic | Along psoas sheath - presents as psoas abscess |
| Lumbar | Reaches inguinal ligament or popliteal fossa |
Clinical Features
Constitutional symptoms:
- Insidious onset of low-grade fever, night sweats, malaise, weight loss
- Usually affects young adults and children from endemic regions
Local symptoms:
- Localized back pain (thoracic or lumbar) - most common presenting complaint
- Point tenderness over spinous processes
- Spasm of paravertebral muscles - rigid "poker" spine
- Deformity: progressive kyphosis (gibbus) - late finding
Neurological features (Pott's paraplegia):
- Occurs in 4-30% of cases
- Sensory deficits precede motor deficits
- Kyphosis + scoliosis = gibbous deformity
- Compressive myelopathy from:
- Epidural abscess (most common cause)
- Angulated kyphotic deformity
- Granulomatous tissue/pannus
MRI of Pott's Spine (Sagittal T2-weighted)
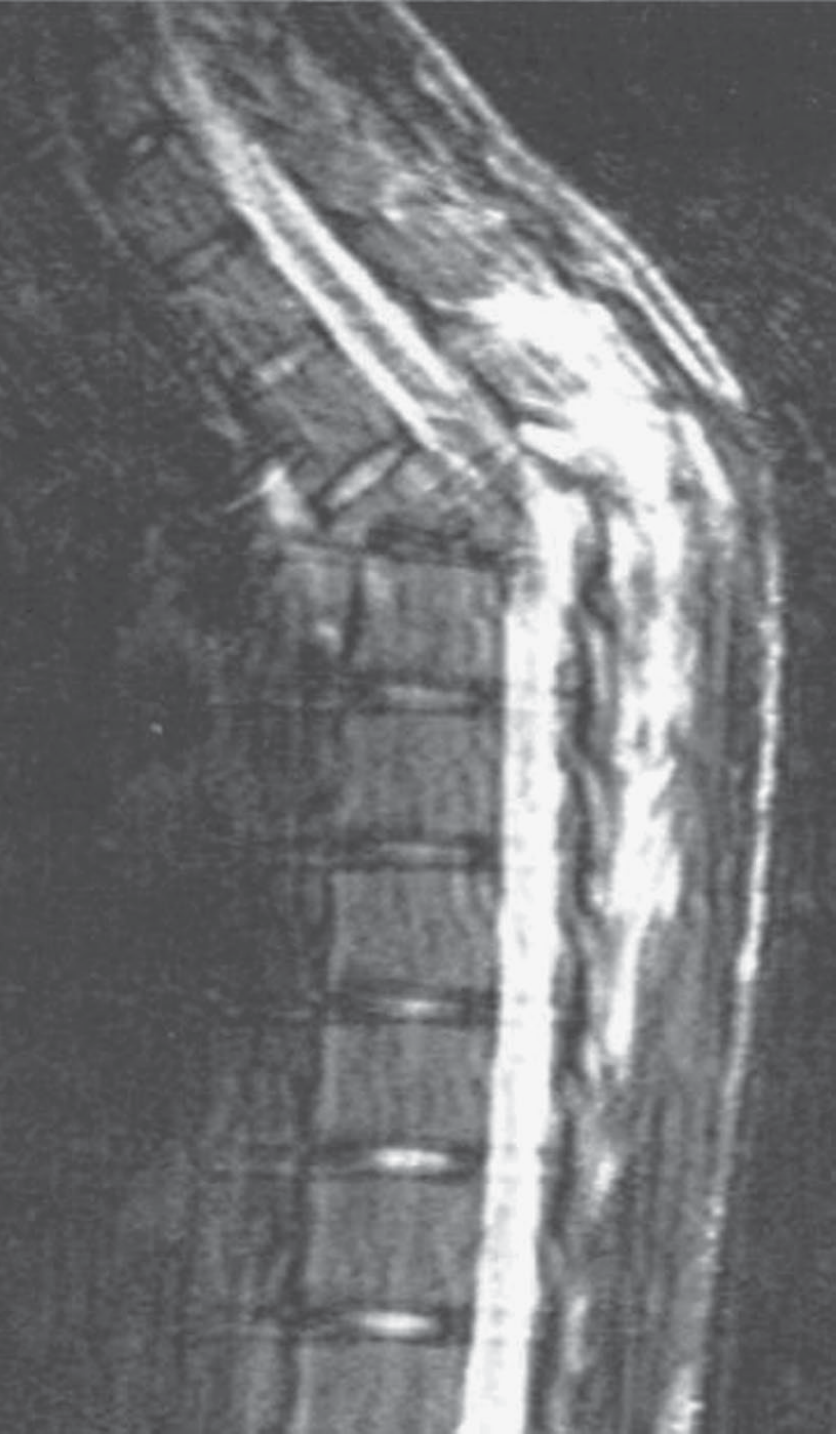
Sagittal T2-weighted MRI showing the angulated kyphotic deformity of the thoracic spine - highly characteristic of Pott's tuberculous spine disease. (Adams & Victor's Principles of Neurology, 12th Ed.)
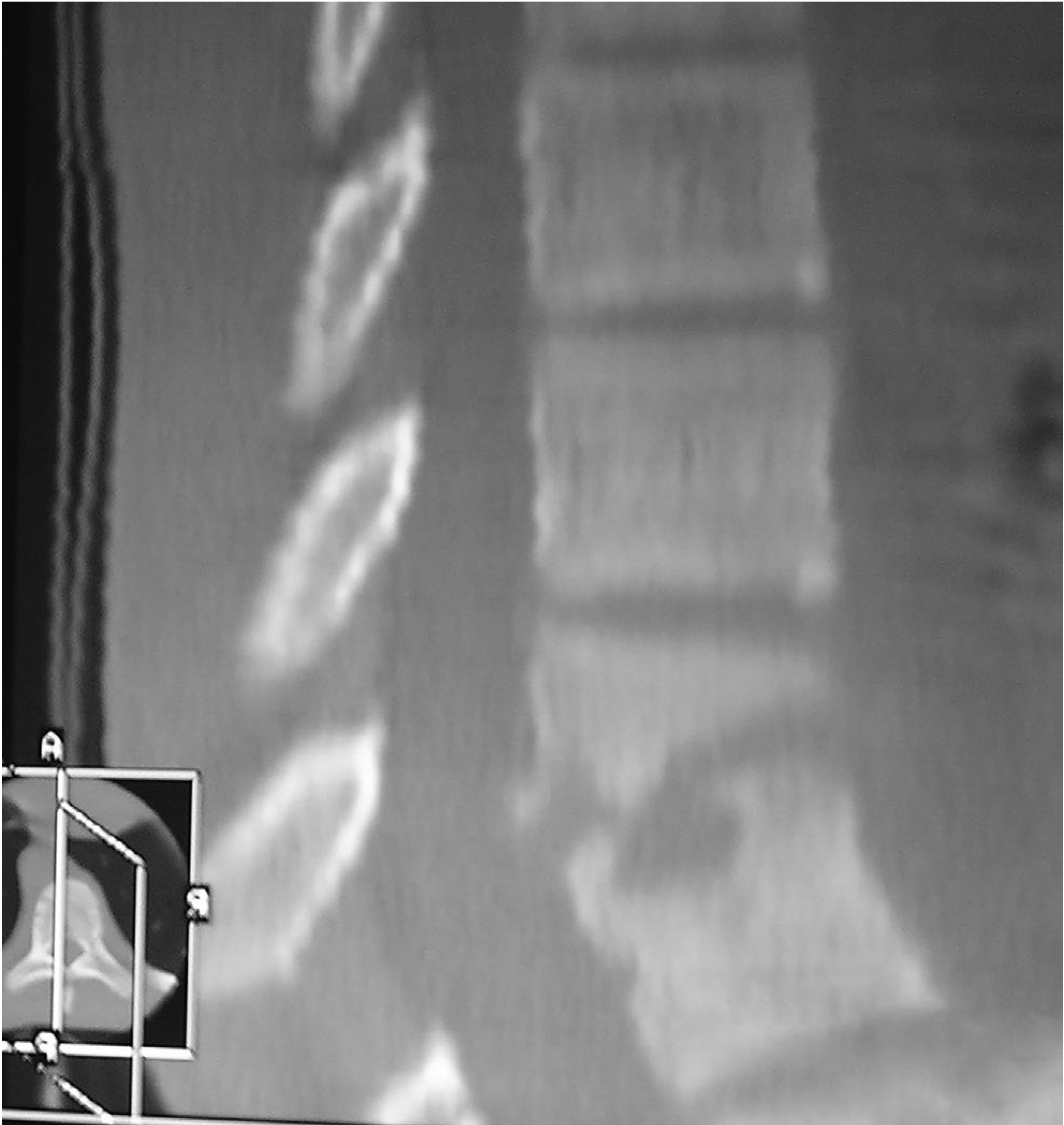
CT sagittal reconstruction showing vertebral collapse and kyphosis in Pott's disease. (Campbell's Operative Orthopaedics, 15th Ed., Fig. 25.2)
Investigations
Radiological:
- X-ray - late finding; loss of disc space, anterior wedging, paravertebral soft tissue shadow, calcified psoas abscess
- Note: disc space is preserved early (unlike pyogenic osteomyelitis where disc is involved early)
- CT scan - shows extent of bone destruction, pedicular erosion (classic: CT of T10 showing pedicle destruction)
- MRI - investigation of choice; shows:
- Vertebral body and disc signal changes
- Extent of cord compression
- Epidural collection
- Characteristic angulated kyphosis
- Paravertebral abscess
Laboratory:
- ESR invariably elevated (degree may be slight)
- Mantoux test / IGRA positive
- AFB culture - synovial fluid, abscess aspirate positive in high percentage
- Synovial fluid: thick, high protein, variable cell count (lymphocytic predominance)
Biopsy:
- Bone biopsy / aspiration of abscess - confirms diagnosis
- Histology: caseating granulomas with Langhans' giant cells
Differential diagnosis:
- Pyogenic osteomyelitis (disc involved early, rapid sclerosis)
- Metastatic deposits (posterior elements often spared in TB)
- Brucellosis (25% skeletal involvement)
- Primary bone tumors
Treatment
Conservative (Medical)
The cornerstone of treatment is anti-tuberculous therapy (ATT). Remarkable results can be obtained with external stabilization + long-term ATT even without surgery.
Standard ATT regimen:
| Phase | Duration | Drugs |
|---|---|---|
| Intensive | 2 months | HRZE (Isoniazid + Rifampicin + Pyrazinamide + Ethambutol) |
| Continuation | 10 months (total 12 months for bone TB) | HR (Isoniazid + Rifampicin) |
Note: Some guidelines recommend 12-18 months total for spinal TB.
Supportive measures:
- Bed rest with spine immobilization (orthosis/plaster jacket)
- Nutritional support
- Treatment of active pulmonary focus if present
Surgical Indications
Surgery is required in:
- Severe spinal deformity (gibbus)
- Compressive myelopathy / Pott's paraplegia
- Large abscess causing cord compression (medical emergency - requires rapid drainage)
- Instability of the spine
- Failure of medical treatment
- Diagnostic uncertainty (biopsy needed)
Surgical Options
| Procedure | Indication |
|---|---|
| Anterior decompression + fusion (Hodgson's Hong Kong operation) | Gold standard for cord compression; radical debridement + bone grafting |
| Posterior instrumented fusion | Stabilization, correction of kyphosis |
| Combined anterior-posterior | Severe deformity, multilevel disease |
| Abscess drainage (percutaneous or open) | Large psoas / paravertebral abscess |
| Laminectomy | Rarely used alone (unstable) |
The Hong Kong operation (anterior radical debridement + strut graft fusion) remains the classic surgical approach for Pott's paraplegia.
Complications
- Pott's paraplegia (most feared) - early: abscess compression; late: fibrous/bony compression
- Gibbus deformity - cosmetic and functional
- Sinus tract formation - abscess tracking to skin
- Secondary amyloidosis (chronic untreated disease)
- Bladder/bowel dysfunction (in severe myelopathy)
- Drug resistance - MDR-TB spinal disease is increasingly reported
Key Differentiating Features: TB vs Pyogenic Spondylitis
| Feature | TB Spondylitis | Pyogenic Osteomyelitis |
|---|---|---|
| Onset | Insidious | Acute |
| Disc space | Preserved early | Involved early |
| Sclerosis | Absent/late | Rapid |
| Cold abscess | Characteristic | Rare |
| Levels | Multiple contiguous | Usually single |
| Neurological | 4-30% | Less common |
Summary Box (Exam Quick Recall)
- Definition: TB of vertebral column; Percival Pott 1779
- Commonest site: Lower thoracic/upper lumbar (adults); upper thoracic (children)
- Hallmark: Gibbus deformity (angular kyphosis)
- Unique feature: Cold abscess; disc space preserved early
- Investigation of choice: MRI spine
- Treatment: ATT (12 months) ± surgery
- Surgery of choice: Hong Kong operation (anterior debridement + strut graft)
- Complication: Pott's paraplegia (4-30%)
Sources: Campbell's Operative Orthopaedics 15th Ed (2026); Harrison's Principles of Internal Medicine 22E (2025); Adams & Victor's Principles of Neurology 12th Ed; Rheumatology 2-Volume Set (Elsevier, 2022)
Radial club hand and keinbocks disease
Reading File
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.