Modified radical neck dissection I need in points for a 10 marks long answer from standard ent text books like Scott brown and Cummings It should include introduction to conclusion flow charts when needed diagrams In the last summarise key points This is needed for ent university knruhs exam for long easst 10 marks answer I don’t need tough sentences I want in easy understandable sentences
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have all the content needed for a comprehensive 10-mark answer. Let me compile it.
Modified Radical Neck Dissection (MRND)
For KNRUHS ENT University Exam - 10 Marks Long Answer
(Sources: Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head and Neck Surgery)
INTRODUCTION
- Neck dissection is a surgical procedure used to remove lymph nodes from the neck that may contain cancer cells spreading from a primary head and neck tumor.
- The Radical Neck Dissection (RND) was first described by Crile in 1906. It removed all lymph nodes (levels I-V) along with three important non-lymphatic structures: the Sternocleidomastoid muscle (SCM), Internal Jugular Vein (IJV), and Spinal Accessory Nerve (SAN).
- Over time, surgeons realized that removing these structures caused significant disability (especially shoulder problems). So the Modified Radical Neck Dissection (MRND) was developed - same lymph node clearance but one or more of those three structures is preserved.
CLASSIFICATION OF NECK DISSECTIONS
NECK DISSECTIONS
|
_____|______________________
| |
COMPREHENSIVE SELECTIVE
(Levels I-V) (Less than 5 levels)
|
|________________________
| |
Radical ND Modified Radical ND
(removes SAN, (preserves 1 or more of:
IJV, SCM) SAN / IJV / SCM)
Types of MRND (based on what is preserved):
| Type | What is Preserved |
|---|---|
| Type I (MRND-I) | Spinal Accessory Nerve (SAN) only |
| Type II (MRND-II) | SAN + Internal Jugular Vein |
| Type III (MRND-III) | SAN + IJV + SCM (also called "Functional Neck Dissection") |
Note: As long as at least ONE of the three structures is preserved, it is called MRND.
DEFINITION
- MRND is the en bloc removal of all lymph node-bearing tissue on one side of the neck, from levels I through V, while preserving one or more of the three non-lymphatic structures: SAN, IJV, and/or SCM.
BOUNDARIES OF DISSECTION
(Cummings, Fig. 118.6 - shown below)
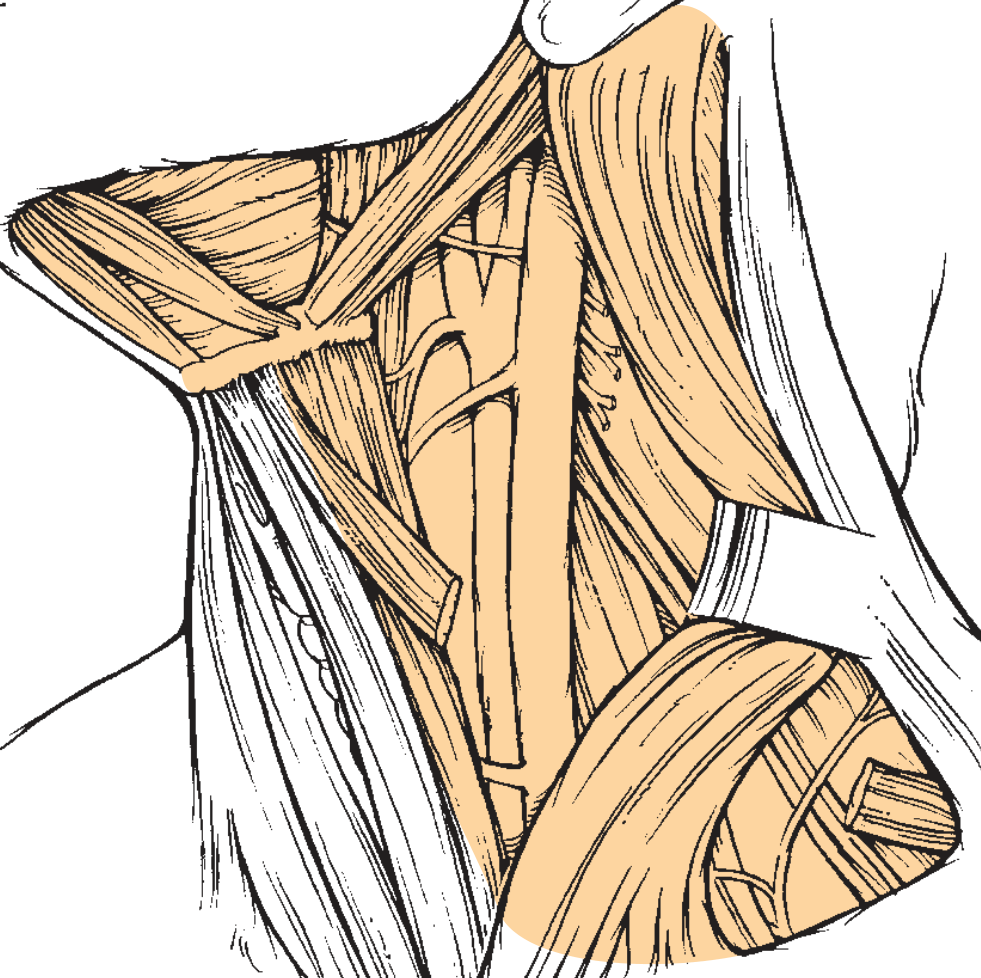
Fig. 118.6 from Cummings: Boundaries of MRND with SAN, IJV, and SCM preserved
| Border | Landmark |
|---|---|
| Superior | Inferior border of mandible |
| Inferior | Clavicle |
| Medial | Contralateral anterior belly of digastric + lateral border of strap muscles |
| Lateral | Anterior border of trapezius muscle |
LYMPH NODE LEVELS REMOVED
All 5 levels are cleared in MRND:
| Level | Location | Key Nodes |
|---|---|---|
| I | Submental (Ia) + Submandibular (Ib) | Drain oral cavity |
| II | Upper jugular group | Drain oropharynx, parotid |
| III | Mid jugular group | Drain larynx, pharynx |
| IV | Lower jugular group | Drain thyroid, esophagus |
| V | Posterior triangle | Drain scalp, posterior neck |
INDICATIONS
- The main use of MRND is when there is grossly visible lymph node disease in the neck (nodal metastasis), but the cancer is not directly fixed to or growing into the SAN, IJV, or SCM.
- If multiple neck levels are involved with mobile nodes, MRND is preferred over RND because it reduces morbidity.
- It is hard to justify removing the SAN if it is not directly involved by tumor - because other nerves (vagus, hypoglossal) lying equally close to nodes are routinely spared.
- MRND is especially important when bilateral neck dissection is needed: sacrificing both IJVs simultaneously can cause severe facial swelling and raised intracranial pressure.
Common primary sites requiring MRND:
- Oral cavity cancers
- Laryngeal cancers
- Oropharyngeal cancers
- Thyroid cancers (with lateral neck nodes)
SURGICAL ANATOMY - KEY STRUCTURES TO KNOW
Spinal Accessory Nerve (SAN) - Most Important to Preserve
- Below the jugular foramen, the SAN runs deep to digastric and stylohyoid muscles
- It lies lateral or just behind the IJV
- Then runs down and back to enter the SCM at the junction of upper and middle thirds
- Exits the SCM at the Erb's point (junction of upper and middle thirds of posterior border of SCM)
- Crosses the posterior triangle and enters trapezius muscle at the junction of its middle and lower thirds
Why preserve SAN? - If cut, the trapezius muscle becomes paralyzed causing severe shoulder drop, pain, and inability to abduct arm above 90 degrees.
SURGICAL TECHNIQUE (Step by Step)
(Cummings, Fig. 118.7 - shown below)
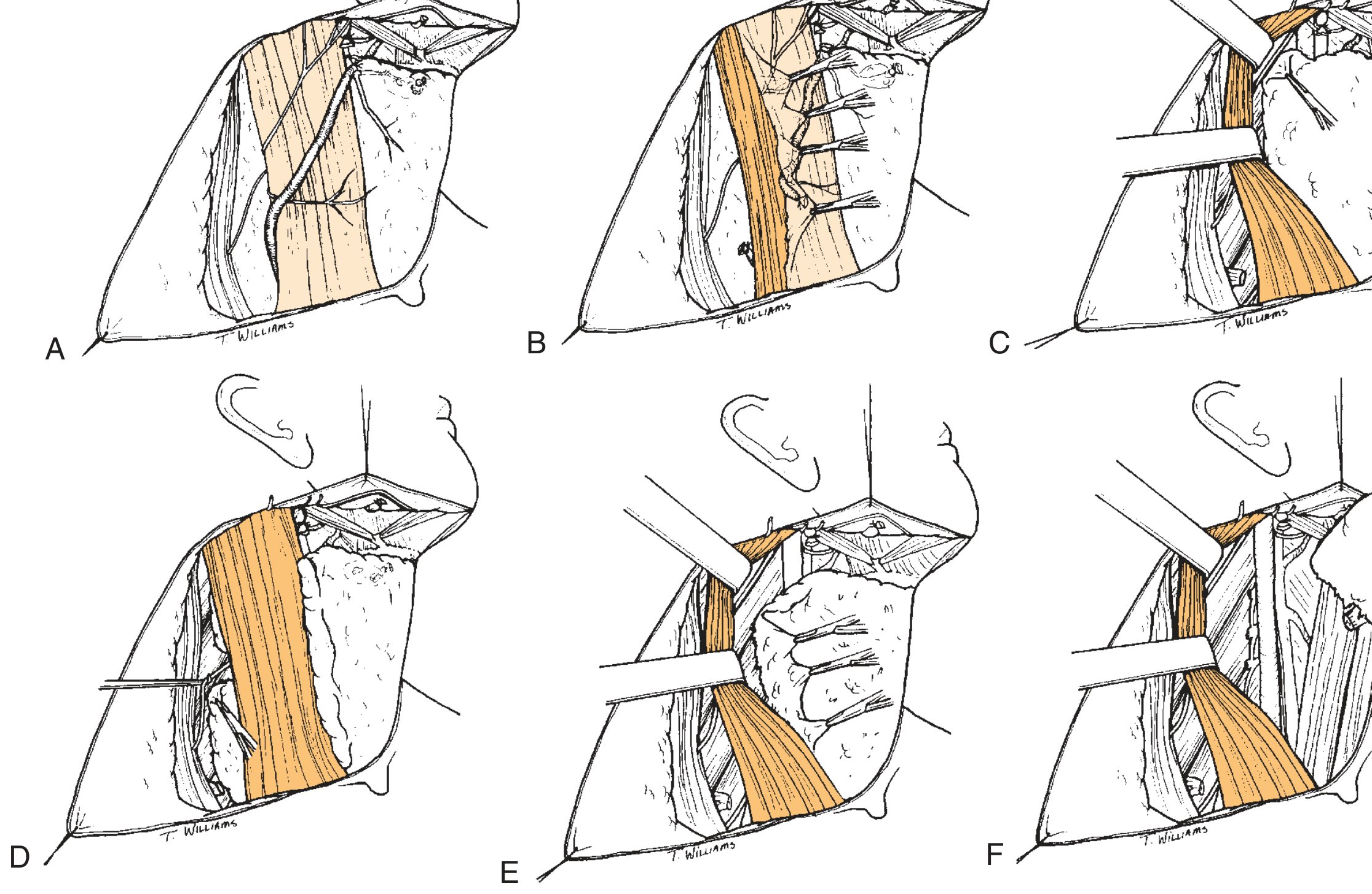
Fig. 118.7 from Cummings: Steps of MRND (A-F)
Step-by-step flowchart:
STEP 1: INCISION AND SKIN FLAP
Subplatysmal flaps raised (same as RND)
↓
STEP 2: PROTECT MANDIBULAR BRANCH of FACIAL NERVE
(Level I dissection - submandibular triangle)
↓
STEP 3: IDENTIFY SAN IN POSTERIOR TRIANGLE
Found at Erb's point (exits SCM posteriorly)
Nerve stimulator may help identify it
↓
STEP 4: DISSECT SAN FREE from fibrofatty tissue
From Erb's point → where it enters trapezius
↓
STEP 5: INCISE ANTERIOR BORDER OF SCM
SCM retracted laterally; fibrofatty tissue
dissected away from the muscle
↓
STEP 6: CLEAR POSTERIOR TRIANGLE
Dissect from trapezius medially
Pass tissue ABOVE SAN → beneath it
Then sweep beneath elevated SCM
↓
STEP 7: DISSECT OFF IJV
Sharp dissection separating contents from
carotid artery and jugular vein
IJV tributaries ligated
↓
STEP 8: SUBMANDIBULAR & SUBMENTAL TRIANGLES
Remove contents; ligate anterior facial vein
↓
STEP 9: DRAIN PLACEMENT AND WOUND CLOSURE
Drains through separate stab incisions
Two-layer closure (platysma + skin)
ADVANTAGES OF MRND OVER RND
| Feature | RND | MRND |
|---|---|---|
| Shoulder function | Poor (SAN removed) | Good (SAN preserved) |
| Cosmesis | Poor (no SCM) | Better (SCM preserved) |
| Bilateral surgery risk | High (both IJVs removed = face swelling) | Safe if IJV preserved |
| Cancer control | Same | Same (equivalent oncologically) |
| Quality of life | Lower | Higher |
COMPLICATIONS
Early Complications
- Hemorrhage - Most common early. Hematoma forms under skin flaps. Needs re-exploration if large.
- Air leaks - Air enters through drain site; usually minor.
- Chylous fistula - Leakage of chyle from thoracic duct injury (on LEFT side, low Level IV). Incidence ~1.9%. Managed conservatively (pressure dressing, low-fat diet) or surgically.
- Wound infection - Risk higher after prior radiotherapy (>70 Gy).
Late Complications
- Shoulder dysfunction - Even in MRND with SAN preservation, EMG abnormalities seen in up to 65% at 4 months (due to nerve stretching during dissection). Most recover by 12 months.
- Numbness - Due to sacrifice of cutaneous branches of cervical plexus (greater auricular, transverse cervical nerves).
- Carotid artery injury - Rare but serious.
- Lymphedema of face - More common if bilateral IJV ligation.
- Phrenic nerve injury - Causes diaphragm paralysis.
- Hypoglossal nerve injury - Causes tongue deviation.
COMPLICATIONS OVERVIEW
|
_____|_______
| |
EARLY LATE
| |
- Hemorrhage - Shoulder dysfunction
- Air leak - Numbness/dysesthesia
- Chyle leak - Lymphedema
- Infection - Nerve palsies
COMPARISON: RND vs MRND vs SND
RND MRND SND (Selective)
(Crile, 1906) (Most common now) (For N0 neck)
| | |
Levels I-V Levels I-V Selected levels
| | (based on primary)
Removes SAN, Preserves 1 or Preserves all 3
IJV, SCM more: SAN/IJV/SCM structures
| | |
Maximum Moderate Minimal
morbidity morbidity morbidity
POSTOPERATIVE CARE
- Drain monitoring (watch for chyle, blood)
- Shoulder physiotherapy - started early in all patients
- EMG of trapezius at 1, 3, 6, 12 months if shoulder weakness noted
- Regular follow-up for recurrence
CONCLUSION
MRND achieves the same oncological clearance as classical RND (all 5 levels, I-V) while preserving one or more important structures (SAN, IJV, SCM). The key surgical landmark is the Spinal Accessory Nerve - identifying and protecting it is the main technical challenge. MRND has largely replaced the classic RND in most head and neck cancers because it gives equivalent cancer control with significantly less morbidity, particularly better shoulder function and quality of life.
KEY POINTS SUMMARY
| # | Key Point |
|---|---|
| 1 | MRND = en bloc removal of lymph nodes Level I-V, preserving at least one of: SAN, IJV, SCM |
| 2 | Main indication = mobile lymph node metastases not fixed to non-lymphatic structures |
| 3 | Main difference from RND = preservation of one or more non-lymphatic structures |
| 4 | SAN is the most important structure to identify and preserve (at Erb's point in posterior triangle) |
| 5 | Boundaries: mandible above - clavicle below - strap muscles medially - trapezius laterally |
| 6 | Three types: Type I (SAN preserved), Type II (SAN+IJV), Type III (all three = Functional ND) |
| 7 | Bilateral MRND is safer than bilateral RND because IJV preserved avoids facial swelling |
| 8 | Even with SAN preservation, shoulder dysfunction can occur due to nerve traction (mostly temporary) |
| 9 | Chylous fistula occurs in ~2% cases during level IV dissection (thoracic duct injury) |
| 10 | MRND has equivalent oncological outcomes to RND but better functional and cosmetic results |
References: Cummings Otolaryngology Head and Neck Surgery (7th ed.), pp. 2296-2309 | Scott-Brown's Otorhinolaryngology Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.