Diabetes management
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"type 2 diabetes"[MeSH Terms] AND "management"[MeSH Terms]
Searching the Web
Type 2 diabetes management guidelines 2025 ADA
Reading File
Finding Sources
Searching PubMed
"type 2 diabetes mellitus"[MeSH Terms] AND "hypoglycemic agents"[MeSH Terms]
Reading File
Reading File
Searching PubMed
"diabetes mellitus type 2"[MeSH Terms] AND "SGLT2 inhibitors"[tiab]
Loading Image
Reading File
Reading File
Here is a comprehensive overview of Type 2 Diabetes Mellitus (T2DM) Management, synthesized from Goodman & Gilman's Pharmacological Basis of Therapeutics, Katzung's Basic and Clinical Pharmacology, the Textbook of Family Medicine, and aligned with the ADA Standards of Care 2025.
Type 2 Diabetes Mellitus - Full Management Overview
1. Goals of Management
The three primary therapeutic goals are:
- Lifestyle modification - cease smoking/alcohol, adopt a healthful eating plan, increase physical activity
- Weight reduction - modest 5-10% reduction from baseline significantly improves insulin sensitivity
- Pharmacologic therapy - introduce safe, effective agents in a timely manner to achieve individualized metabolic targets
- Textbook of Family Medicine 9e, p. 975
Glycemic targets are individualized. The general A1c target is ≤7%, though more or less stringent goals may apply depending on the patient's age, comorbidities, and hypoglycemia risk.
2. Lifestyle & Non-Pharmacologic Interventions
Diet
- Macronutrient composition should be individualized; typical split is ~45% carbohydrate, 25-35% fat, 10-35% protein
- Limiting carbohydrates and substituting with monounsaturated fats (olive oil, nuts, avocados) lowers triglycerides and raises HDL
- Mediterranean-style eating improves glycemic control and reduces cardiovascular/stroke endpoints
- Caloric restriction and weight loss are key goals for obese patients
Physical Activity
- Regular exercise improves insulin sensitivity and is especially important in metabolically obese, normal-weight patients
Weight Loss
Approved pharmacologic options for obesity co-management include:
- Orlistat
- Phentermine/topiramate
- Naltrexone + extended-release bupropion
- High-dose liraglutide
- Semaglutide
Bariatric surgery (Roux-en-Y gastric bypass, gastric sleeve, etc.) can result in T2DM remission in selected patients.
- Katzung's Basic and Clinical Pharmacology 16e, p. 1193, 1195
3. Treatment Algorithm
The stepwise approach below is the consensus framework (ADA, EASD, NICE guidelines):
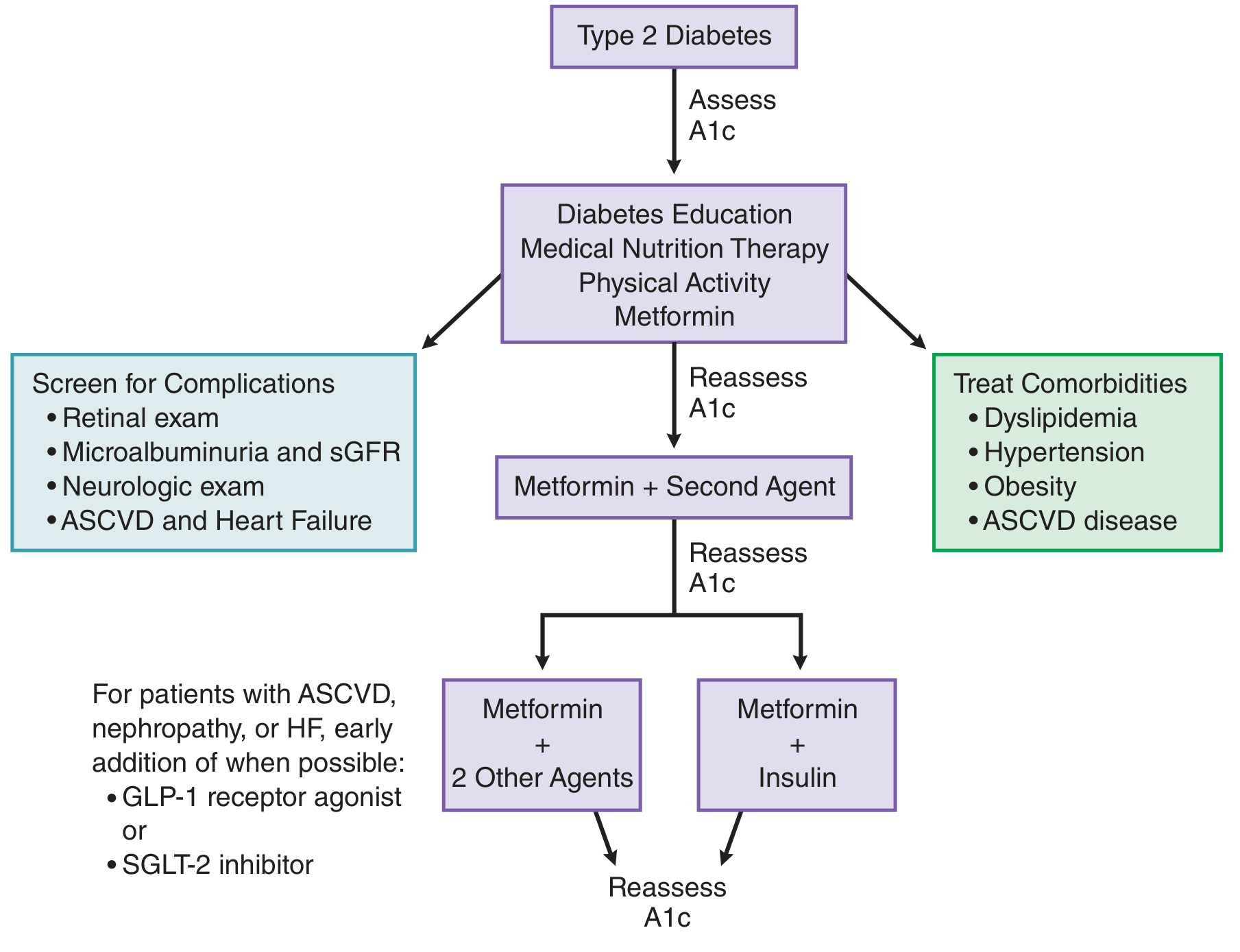
Step 1 - Diagnosis: Assess A1c, start diabetes education, medical nutrition therapy, physical activity, and metformin
Step 2 - Reassess A1c (2-3 months): If target not met, add a second agent
Step 3 - If still not at target: Escalate to metformin + 2 other agents or metformin + insulin
Special note: For patients with ASCVD, nephropathy, or heart failure, add a GLP-1 receptor agonist or SGLT-2 inhibitor early in the treatment course, even as a second agent.
- Goodman & Gilman's 14e, p. 1061
Alongside pharmacotherapy, always screen for complications (retinal exam, microalbuminuria, eGFR, neurologic exam, ASCVD/HF) and treat comorbidities (dyslipidemia, hypertension, obesity).
4. Pharmacotherapy
First-Line: Metformin (Biguanide)
- Remains the consensus first-line agent unless contraindicated
- Mechanism: reduces hepatic glucose output, improves insulin sensitivity
- Weight neutral, low hypoglycemia risk, inexpensive
- Key risk: lactic acidosis (rare; avoid in significant renal impairment)
Second-Line Options (choose based on comorbidities, weight, cost, hypoglycemia risk)
| Drug Class | Examples | Efficacy | Weight Effect | Key Benefit | Key Risk |
|---|---|---|---|---|---|
| GLP-1 RA | Liraglutide, Semaglutide | High | Weight loss | CV benefit, ASCVD | GI effects, pancreatitis |
| Dual GIP/GLP-1 RA | Tirzepatide | High | Significant weight loss | CV + metabolic benefit | GI effects |
| SGLT2 inhibitors | Empagliflozin, Dapagliflozin | Moderate | Weight loss | CV + renal protection | UTI, genital infection, DKA |
| DPP-4 inhibitors | Sitagliptin, Saxagliptin | Moderate | Neutral | Well tolerated | Nasopharyngitis, joint pain |
| Sulfonylureas | Glipizide, Glyburide, Glimepiride | High | Weight gain | Cheap | Hypoglycemia, weight gain |
| Thiazolidinediones | Pioglitazone | High | Weight gain | CV benefit (mild) | Fracture risk, HF, possible bladder cancer |
| Meglitinides | Repaglinide, Nateglinide | High | Neutral | Post-meal control | Hypoglycemia |
| Basal Insulin | Glargine, Detemir | High | Weight gain | Flexible add-on | Hypoglycemia, weight gain |
Key evidence: The GRADE study (NIH-funded) found that adding liraglutide or basal insulin to metformin produced slightly better glycemic control than glimepiride or sitagliptin.
- Goodman & Gilman's 14e, pp. 1061-1062
- Katzung's Basic and Clinical Pharmacology 16e, pp. 1195-1196
5. Insulin Therapy
Insulin is often required as T2DM progresses and beta-cell reserve declines (measurable by C-peptide levels). Common regimens:
- Basal insulin (glargine or detemir) at bedtime + oral agent for daytime control
- Full basal-bolus regimen for more advanced cases
- Closed-loop insulin systems (automated pumps) are now available and improve time-in-range
6. Monitoring
| Parameter | Target |
|---|---|
| HbA1c | <7% (individualized: <6.5% to <8%) |
| Fasting blood glucose | 90-130 mg/dL |
| Postprandial glucose | <180 mg/dL (2h) |
| Time in Range (CGM) | >70% (70-180 mg/dL) |
Monitoring tools include:
- BGM (blood glucose monitoring) - self-testing with strips
- CGM (continuous glucose monitoring) - real-time glucose trends, especially useful with insulin or risk of hypoglycemia
7. Screening for Complications
At diagnosis and periodically thereafter:
| Complication | Screening |
|---|---|
| Retinopathy | Dilated retinal exam |
| Nephropathy | Microalbuminuria, eGFR |
| Neuropathy | Neurologic/foot exam |
| Cardiovascular | BP, lipids, ECG, ASCVD risk assessment |
8. Patient Education & Self-Management
Patients must be actively engaged - they make daily decisions about food, activity, dosing, and monitoring. Key education points:
-
Understanding glucose variability and its causes (exercise, meals, medications, illness)
-
Recognizing and treating hypoglycemia
-
Insulin dose adjustment for meals and activity (if on insulin)
-
Never blame patients for imperfect control - diabetes self-management is cognitively demanding
-
Textbook of Family Medicine 9e, p. 975
9. Cost Considerations
- Metformin and sulfonylureas are inexpensive generics
- GLP-1 RAs, SGLT2 inhibitors, DPP-4 inhibitors, and newer insulins are significantly more expensive
- Cost affects adherence and must be part of shared decision-making
- Insulin biosimilars are available but pricing remains high
2025 ADA Updates (Key)
Per the ADA Standards of Care in Diabetes 2025, notable updates include:
- New recommendations on nutrition and weight-loss medications
- Expanded guidance on diabetes technology (CGM, closed-loop systems)
- Updated algorithms for cardiovascular and renal comorbidity management
- Emphasis on weight management as a pillar of T2DM treatment (GLP-1/GIP agonists increasingly central)
This is a shared conversation. Sign in to Orris to start your own chat.