for mortons neuroma in podiatry uk, give me a definition, assessment- 2 clinical tests with reasoning, risk factors, 3 differential diagnoses with reasoning why it isnt those, managemnet and an insole prescription with reasoning.
Reading File
Finding Sources
Finding Sources
Searching the Web
Morton's neuroma podiatry UK assessment management insole prescription clinical guidelines 2024
Searching PubMed
"Morton neuroma" AND treatment
Reading File
Reading File
Reading File
Reading Web Page
clinical tests assessment Morton neuroma sensitivity specificity
Reading Article
Finding Sources
Loading Image
I now have everything needed to compile a thorough, UK podiatry-focused response. Here it is:
Morton's Neuroma — UK Podiatry Clinical Reference
Definition
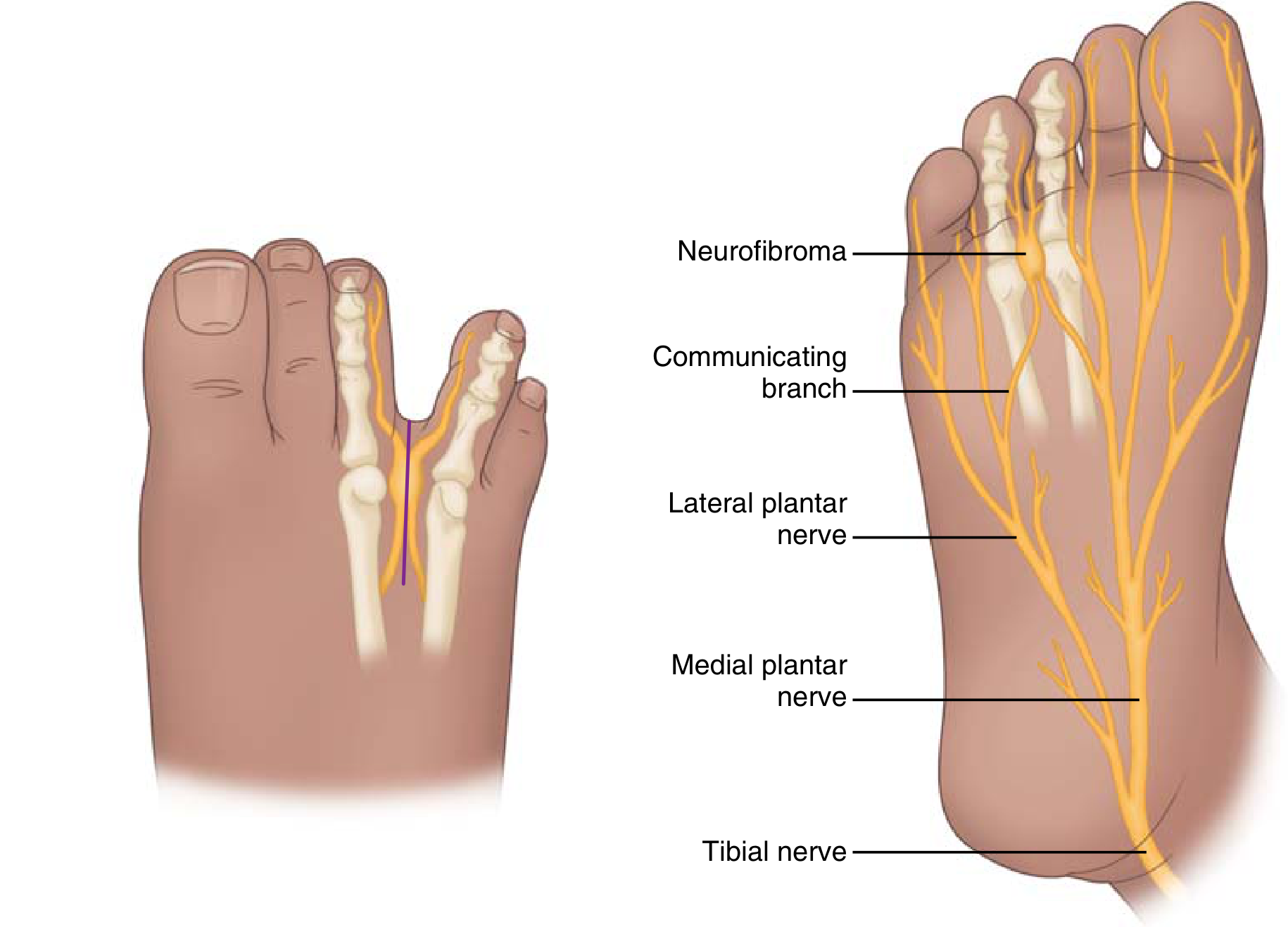
Morton's neuroma (MN) is a compressive neuropathy of the common plantar digital nerve, most commonly occurring in the 3rd intermetatarsal web space (43–86% of cases), followed by the 2nd web space. Despite the name, it is not a true neuroma — it is a degenerative, not neoplastic, lesion. Histologically it demonstrates perineural fibrosis, endoneural oedema, arterial degeneration, and neural degeneration rather than neoplastic proliferation.
The nerve becomes entrapped beneath the deep transverse intermetatarsal ligament and is subject to repetitive compression and traction, leading to demyelination and eventual fibrosis. In the UK, the condition affects approximately 87.5 females and 50.2 males per 100,000 population and is the third most common condition referred to foot and ankle surgeons in the UK (Pitcher et al., Foot & Ankle Orthopaedics, 2024).
Assessment
Subjective History
Key presenting symptoms include:
- Burning or shooting pain in the plantar forefoot/web space, often radiating into the toes (>60% of patients)
- Sensation of "walking on a pebble"
- Symptoms aggravated by walking (sensitivity 91–92%) and relieved by rest (sensitivity 81–89%)
- Patient-reported clicking has been found to be clinically useful in diagnosis
- Paroxysmal numbness or tingling into adjacent toes (~40% of patients)
- Symptoms worsened by narrow or high-heeled footwear
Clinical Test 1: Mulder's Sign (Squeeze Test)
Technique: With the patient seated or supine, apply lateral compression of the forefoot with one hand (squeezing the metatarsal heads together mediolaterally), while simultaneously applying direct plantar pressure with the thumb of the other hand into the affected web space. A positive test is reproduction of the patient's pain and/or a palpable/audible "click" (Mulder's click) as the neuroma is displaced plantarly.
Reasoning: Lateral compression narrows the intermetatarsal space, increasing pressure on the entrapped nerve and displacing the fibrotic mass. The click represents the neuroma subluxing under the examiner's thumb out of the inter-metatarsal space. A 2024 systematic review (Pitcher et al., University of Hertfordshire) found sensitivity ranging from 29–94% and specificity from 17–100%, with the highest-quality studies reporting specificity of 87–100%. Likelihood ratios were weak to moderate. Mulder's sign is nonetheless endorsed as a key test by the American College of Foot and Ankle Surgeons (ACFAS) and Association of Extremity Nerve Surgeons. It is most useful when positive in the clinical context of a typical history. — Miller's Review of Orthopaedics 9th ed.
Clinical Test 2: Webspace Tenderness / Direct Palpation Test
Technique: With the patient seated, use your index finger to apply direct plantar pressure into the affected web space between the metatarsal heads (just distal to the metatarsal heads, in the plantar interdigital space). A positive result is focal, reproducible tenderness that matches the patient's reported pain site. This should be compared to adjacent web spaces to confirm specificity.
Reasoning: The neuroma forms at the plantar aspect of the web space, plantar to the deep transverse intermetatarsal ligament. Direct compression over this site mechanically irritates the fibrotic nerve sheath. It is a discriminating test when combined with the history — tenderness that is web space specific (rather than diffuse metatarsal head tenderness) distinguishes MN from generalised metatarsalgia. Pitcher et al. (2024) confirmed webspace tenderness testing is considered a key examination test by expert consensus (Delphi study). When used alongside Mulder's sign and a positive history (clicking, radiating burning pain), diagnostic confidence is substantially increased — Miller's Review of Orthopaedics 9th ed.; Roberts & Hedges' Clinical Procedures in Emergency Medicine.
Risk Factors
| Category | Risk Factor | Mechanism |
|---|---|---|
| Footwear | Narrow toe box, high heels | Increased lateral compression of metatarsal heads; forced plantarflexion of MTP joints increases traction on digital nerves |
| Sex | Female sex | 87.5/100,000 vs 50.2/100,000 males — likely related to footwear habits and narrower forefoot morphology |
| Biomechanical | Pes planus (hyperpronation), forefoot valgus | Altered loading causes increased nerve traction during propulsion |
| Biomechanical | Hallux valgus, tight Achilles | Shifts load laterally onto 2nd/3rd MTP; increases forefoot pressure |
| Occupation/Activity | High-impact sport, prolonged standing, ballet | Repetitive microtrauma to interdigital nerve |
| Anthropometric | Wide forefoot, splayed metatarsals | Reduced intermetatarsal space at midstance |
| Age | Middle age (peak 4th–6th decade) | Cumulative microtrauma; age-related perineural changes |
Differential Diagnoses
1. Metatarsalgia / MTP Synovitis
Presentation overlap: Plantar forefoot pain at the metatarsal heads, worsened by walking, often bilateral.
Why it is NOT Morton's neuroma:
- Pain in metatarsalgia is diffuse across the metatarsal heads rather than web space-specific; it does not radiate neurologically into the toes
- Tenderness is dorsal and directly over the MTP joint rather than plantar and interdigital
- Mulder's sign is negative — no click and no web space reproduction of pain
- MTP synovitis may show dorsal MTP swelling, plantar plate laxity, and a positive Lachman's test of the toe (vertical instability of the proximal phalanx)
- Imaging (USS/MRI) shows joint effusion or synovitis rather than a plantar web space mass
- Miller's Review of Orthopaedics: "Metatarsalgia and MTP synovitis often manifest similarly and should be ruled out"
2. Intermetatarsal Bursitis
Presentation overlap: Pain and localised swelling in the web space, can produce a click and forefoot tenderness very similar to MN.
Why it is NOT Morton's neuroma:
- The intermetatarsal bursa lies on the dorsal aspect of the interdigital nerve; bursitis pain is therefore more diffuse and dorsal rather than plantar and focal
- No neurological symptoms — no burning, no radiation into toes, no numbness
- Mulder's sign may be positive (bursa can be displaced) but no neurological sensory change into the toes
- USS distinguishes the two: bursitis shows a fluid-filled, compressible anechoic sac rather than a solid hypoechoic mass
- Bursitis more commonly associated with inflammatory arthropathy (RA, gout) — check bloods (ESR, CRP, uric acid)
- Pfenninger & Fowler's Procedures for Primary Care: "care must be taken to differentiate intermetatarsal bursa from a Morton's neuroma"
3. Stress Fracture of the Metatarsal (2nd or 3rd)
Presentation overlap: Localised forefoot pain, worsened by weight-bearing, tenderness between metatarsals.
Why it is NOT Morton's neuroma:
- Pain is bony and activity-related (worse during exercise, improving with rest) rather than a burning neurological quality
- Tenderness is over the metatarsal shaft (often dorsal), not in the plantar web space
- No neurological features — no radiation, burning, numbness or tingling
- History typically involves recent increase in training load or high-impact activity (overuse context)
- Positive "tuning fork test" or "bump test" (axial loading elicits pain at fracture site)
- Plain X-ray may be normal initially; MRI or bone scan confirms periosteal reaction or stress response
- Mulder's sign is negative
- Rosen's Emergency Medicine: "MRI may be helpful to clarify diagnostic challenges for entities such as Morton's neuroma, tendinitis, stress fractures, and turf toe"
Management (UK Podiatry Stepwise Approach)
Step 1 — Conservative (First-line, all patients)
- Footwear modification: Widened toe box, low heel (<2.5 cm), cushioned sole — this is the most important initial intervention. Narrow, high-heeled or thin-soled footwear must be avoided. (NHS York Hospitals guidance)
- Orthotic insoles: See detailed prescription below
- Activity modification: Reduce high-impact activities temporarily
- Patient education: Reassurance that MN is benign; avoid aggravating footwear
Step 2 — Pharmacological
- NSAIDs (e.g., ibuprofen 400mg TDS with food) for short-term pain relief — discuss with prescriber if comorbidities
- Topical NSAIDs if GI risk
Step 3 — Injection Therapy
- Corticosteroid + local anaesthetic injection (e.g., methylprednisolone + 1% lidocaine): ~50–80% report short-term relief; however the 2024 Cochrane Review (Matthews et al., Cochrane Database Syst Rev, PMID: 38334217) found low-certainty evidence that CS+LA confers little to no difference over LA alone for pain or function at 3–6 months. No long-term benefit demonstrated. Limit to 2–3 injections to avoid plantar fat pad atrophy and risk of hammer-toe deformity.
- Sclerosing alcohol injections: Not recommended — not proven effective (Miller's)
- Ultrasound guidance increases accuracy and is standard in UK specialist practice
Step 4 — Imaging
- Ultrasound (USS): First-line imaging in UK — confirms hypoechoic mass in web space, excludes bursitis. USS-guided injection if doubt exists.
- MRI: For diagnostic uncertainty or when surgery is planned; best on short-axis sequences; T1 shows low-signal fibrotic mass against high-signal fat
Step 5 — Surgical Referral
Indicated when conservative care (minimum 3–6 months) and injection therapy have failed:
- Neurectomy (dorsal approach most common): Nerve resected 2–3 cm proximal to the intermetatarsal ligament to allow stump retraction; success ~80%; risk of stump neuroma (~1%)
- Decompression (ligament release): Alternative nerve-sparing option
- Cryosurgery: Emerging minimally invasive option; limited evidence but increasingly used in UK (mortonsneuroma.co.uk)
- The 2024 meta-analysis (Lee et al., Foot Ankle Surg, PMID: 38880729) found no significant difference in outcomes between dorsal and plantar surgical approaches
Insole Prescription with Reasoning
Prescription
Semi-rigid custom-moulded functional foot orthosis with the following specific features:
| Feature | Specification | Clinical Reasoning |
|---|---|---|
| Metatarsal dome / bar | 5–6mm EVA dome placed proximal to the symptomatic metatarsal heads (typically proximal to MT3–MT4 junction for 3rd web space MN) | Elevates and splays the metatarsal shafts, widening the intermetatarsal space during weight-bearing and indirectly decompressing the entrapped digital nerve. This is the single most evidence-informed orthotic component for MN. Miller's: "Metatarsal pads placed proximal to the focus of pain can prevent direct pressure and widen the intermetatarsal space during weight bearing, thereby indirectly decompressing the nerve" |
| Metatarsal head relief / excavation | Shallow relief (1–2mm) cut out directly beneath MT3 head (or affected head) in insole shell | Directly reduces plantar pressure over the most compressed point, providing immediate symptom relief during stance and propulsion |
| Arch support / medial longitudinal arch control | Neutral to mild arch support (3–5° varus posting if hyperpronation present) | Hyperpronation causes lateral displacement of the forefoot and increased nerve traction across the intermetatarsal ligament during propulsion. Arch control reduces this traction force. For patients with confirmed pes planus: use pronation control orthotic |
| Rearfoot posting | Neutral or mild varus (2–4°) if foot is pronated | Addresses rearfoot-driven forefoot compensation and reduces torsional forces transmitted to the forefoot |
| Top cover | 3mm Poron or PPT cushioned top cover | Reduces repetitive mechanical loading and shock to the plantar forefoot; provides comfort especially during propulsion |
| Shell material | 3mm Polypropylene or 35–45 Shore A EVA for active patients; softer EVA for elderly/sensitive patients | Firm enough to maintain functional correction; flexible enough for comfort within shoe |
| Heel cup | Standard 14–16mm heel cup | Controls rearfoot position; optimises pronation control function of device |
| Forefoot width extension | Full-length or 3/4 length device — ensure device fits in wide, low-heeled shoe | Ineffective if patient continues in narrow or high-heeled footwear — always prescribe alongside footwear advice |
Key Prescribing Considerations
- Location of the dome is critical: Too distal = the dome sits under the nerve (increases compression); too proximal = no mechanical effect. Aim 1–1.5cm proximal to the symptomatic web space.
- Confirm footwear compatibility: A well-designed insole worn in a narrow shoe provides no net benefit — footwear change is a prerequisite.
- Biomechanical assessment first: If the patient overpronates, this must be controlled — the intermetatarsal traction occurs primarily during the propulsive phase in a pronated foot. A purely cushioning insole without biomechanical correction will underperform.
- Review at 6–8 weeks: Reassess dome position clinically — if symptoms persist, adjust dome 3–5mm proximally.
Recent Evidence Summary
| PMID | Study | Finding |
|---|---|---|
| 38334217 | Cochrane Review 2024 — Matthews et al. | Corticosteroid + LA = low-certainty evidence of little/no benefit over LA alone; surgery superior to conservative care at 12 months |
| 38880729 | Meta-analysis 2024 — Lee et al. | Dorsal vs plantar neurectomy: no significant outcome difference |
| Pitcher et al. 2024 (Univ. Hertfordshire) | Systematic review of clinical tests | Mulder's sign: sensitivity 29–94%, specificity 87–100% in better-quality studies; patient-reported clicking most diagnostically useful subjective feature |
Summary for practice: MN is primarily a clinical diagnosis. Two key tests — Mulder's sign and webspace tenderness — supported by a characteristic history (burning, radiating pain, clicking, worsened by narrow footwear) are sufficient to diagnose and begin conservative management. First-line UK podiatry management is footwear advice + metatarsal dome orthosis. Injection provides short-term relief but limited long-term benefit. Refer for surgical neurectomy after 3–6 months of failed conservative care.
Can you put this in a word document
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Running Command
The file is a valid DOCX (18 KB, proper ZIP structure with all required XML components). Here's your download link:
Mortons Neuroma UK Podiatry
Word Document · DOCX
The document includes:
- Header with document title on every page
- Page numbers in the footer
- 7 formatted sections: Definition, Assessment (both clinical tests), Risk Factors, Differentials, Management, Insole Prescription, and Evidence Summary
- Colour-coded tables with alternating row shading for the risk factors, insole prescription, and evidence tables
- Styled headings in navy/blue (H1 with underline rule, H2, H3)
- All references/sources listed at the foot of the document
This is a shared conversation. Sign in to Orris to start your own chat.