Anatomy of the skull
Reading File
Finding Sources
Searching the Web
skull anatomy bones foramina detailed overview
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Loading Image
I now have all the material needed for a thorough, well-illustrated answer. Here is the complete overview of skull anatomy.
Anatomy of the Skull
The skull is the bony framework of the head. It consists of 22 bones (excluding the ossicles of the middle ear) divided into two major regions: the neurocranium (cranium proper - encloses the brain) and the viscerocranium (facial skeleton).
- Gray's Anatomy for Students, p. 1000-1005
- PC Dikshit Textbook of Forensic Medicine and Toxicology, p. 193
1. Overview and Regions
| Region | Function | Key Bones |
|---|---|---|
| Neurocranium | Protects the brain | Frontal, parietal (x2), occipital, temporal (x2), sphenoid, ethmoid |
| Viscerocranium | Forms the face | Mandible, maxilla, zygomatic, nasal, lacrimal, palatine, vomer, inferior nasal concha |
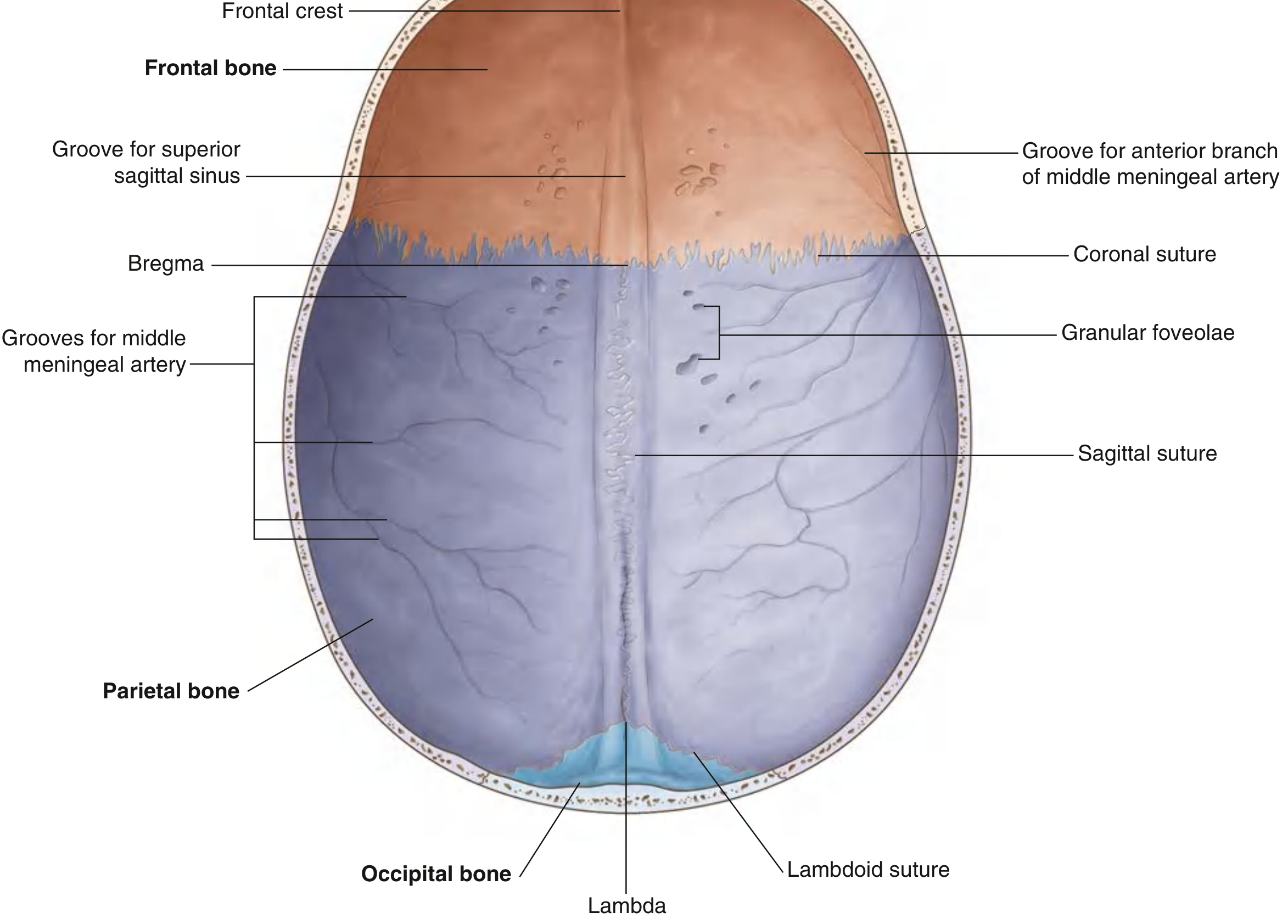
2. The Calvaria (Vault / Roof)
The calvaria is the dome-shaped roof of the cranial cavity. It is composed of:
- Frontal bone (anterior)
- Parietal bones (middle - paired)
- Occipital bone (posterior)
Sutures
These are fibrous joints between the flat bones of the skull:
| Suture | Bones Joined | Junction Point |
|---|---|---|
| Coronal suture | Frontal + parietal | - |
| Sagittal suture | Parietal + parietal | - |
| Lambdoid suture | Parietal + occipital | - |
| Bregma | Coronal + sagittal sutures meet | Anterior fontanelle in infants |
| Lambda | Lambdoid + sagittal sutures meet | Posterior fontanelle in infants |
Internal surface of the calvaria
- The frontal crest (midline ridge) and crista galli are attachment points for the falx cerebri
- The groove for the superior sagittal sinus runs in the midline from front to back
- Granular foveolae are pits that mark arachnoid granulations (involved in CSF reabsorption)
- Grooves for the middle meningeal artery branch laterally from the coronal suture
3. Bone Structure
The adult skull has a unique three-layer structure:
- Outer table - thick compact bone (~twice the inner table)
- Diploe - cancellous (spongy) bone containing red bone marrow; begins forming at ~4 years of age
- Inner table - thinner compact bone
Thickness varies by location:
- Temporal bone: ~4 mm (thinnest - most susceptible to fracture)
- Frontal and parietal: ~6-10 mm
- Occipital (midline): up to 15 mm (thickest)
Strong areas: greater wing of sphenoid, petrous temporal, sagittal ridge, occipital protuberance, glabella.
Thin areas: parieto-temporal, lateral frontal, lateral occipital zones.
4. The Cranial Cavity and its Three Fossae
The floor of the cranial cavity is divided into three stepped regions (fossae).
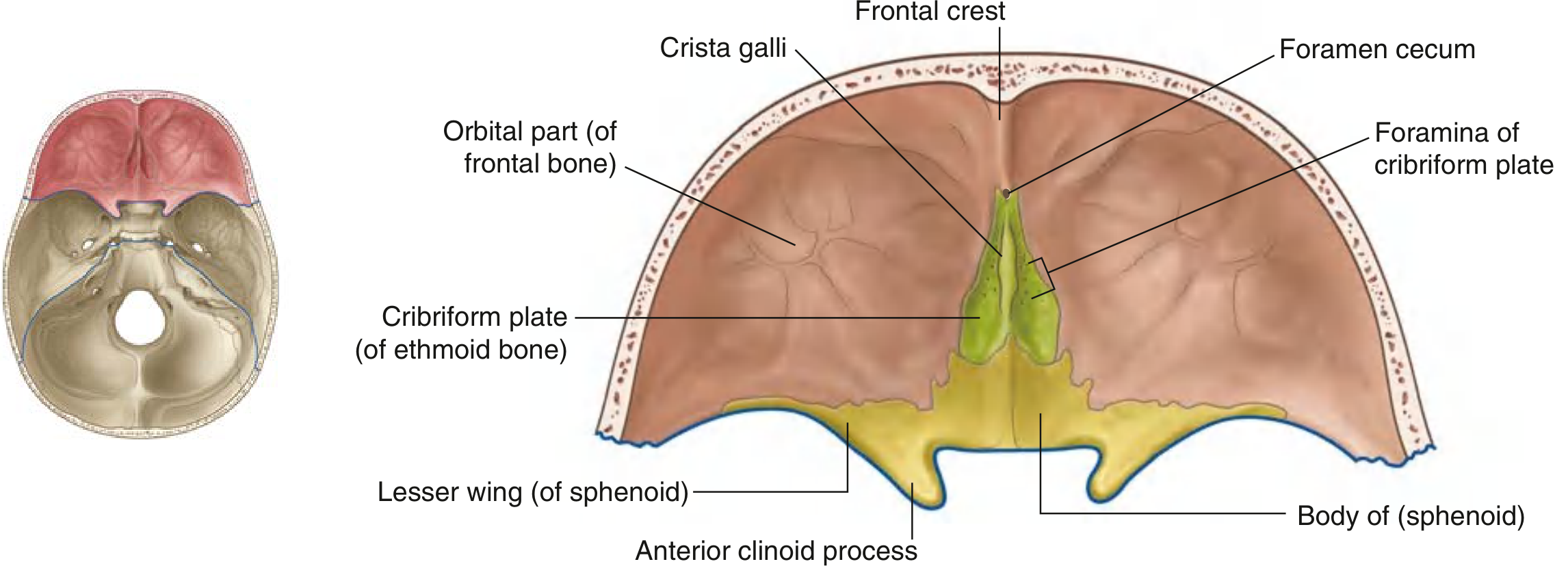
Anterior Cranial Fossa
Bones: Frontal, ethmoid (cribriform plate, crista galli), and sphenoid (body + lesser wings)
Contents: Frontal lobes of the cerebrum
Key features:
- Cribriform plate of ethmoid - sieve-like plate transmitting olfactory nerve (CN I) fibres from the nasal mucosa to the olfactory bulb
- Crista galli - midline bony projection; attachment for the falx cerebri
- Frontal crest - another falx cerebri attachment
- Foramen cecum - may transmit emissary veins connecting nasal cavity to superior sagittal sinus
- Anterior clinoid processes (lesser wings of sphenoid) - attachment for the tentorium cerebelli
- Boundary with middle fossa: anterior edge of the prechiasmatic sulcus
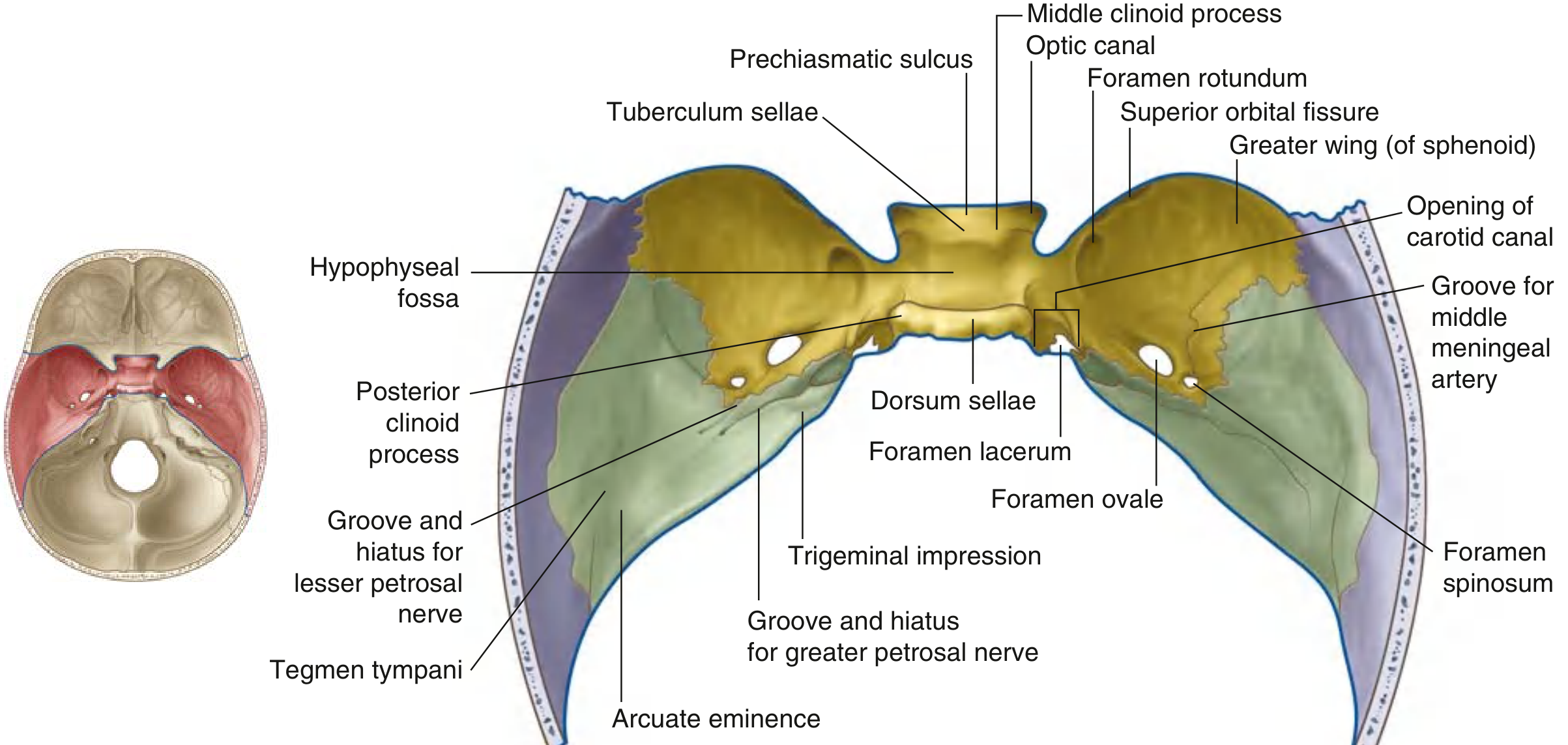
Middle Cranial Fossa
Bones: Sphenoid (body + greater wings) and temporal bones (squamous part)
Contents: Temporal lobes of the cerebrum and the pituitary gland
Key features:
- Sella turcica - the "Turkish saddle" in the body of sphenoid; contains the hypophyseal fossa (housing the pituitary gland), bounded anteriorly by the tuberculum sellae and posteriorly by the dorsum sellae
- Posterior clinoid processes - tops of dorsum sellae; attachment for tentorium cerebelli
- Carotid sulcus - groove for the internal carotid artery
- Tegmen tympani - thin bony roof of the middle ear cavity
- Arcuate eminence - rounded bony protrusion overlying the anterior semicircular canal
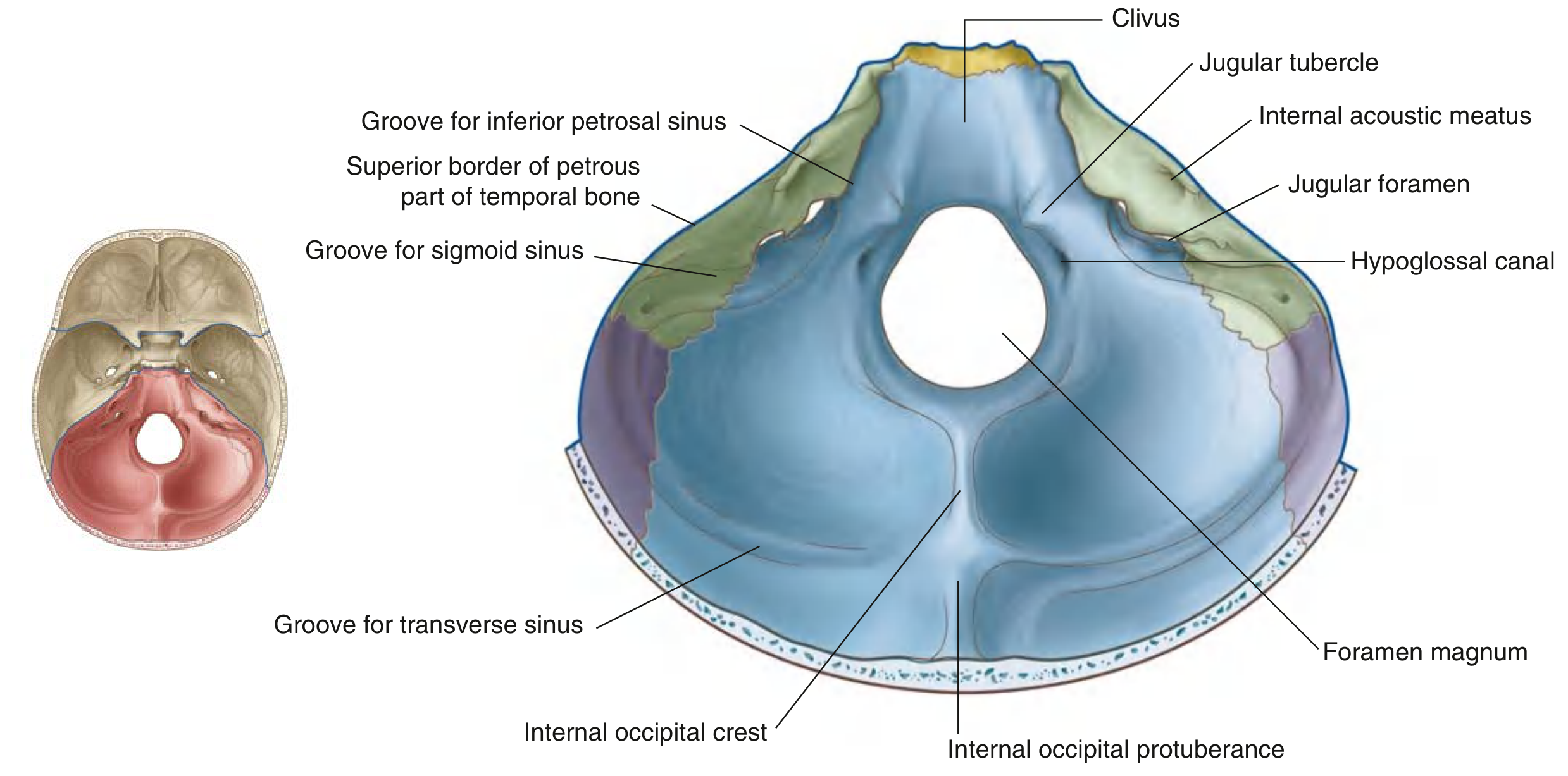
Posterior Cranial Fossa
Bones: Occipital (mostly), temporal (petrous + mastoid), small contributions from sphenoid and parietal
Contents: Brainstem (midbrain, pons, medulla) and cerebellum - it is the largest and deepest fossa
Key features:
- Foramen magnum - largest foramen in the skull; passage of the spinal cord/brainstem, vertebral arteries, meninges, and spinal roots of the accessory nerve (CN XI)
- Clivus - sloping bone (basilar part of occipital + sphenoid body) ascending from foramen magnum; supports the brainstem
- Internal occipital protuberance - where the transverse sinuses diverge
- Groove for transverse sinus - runs laterally to the internal occipital protuberance
- Groove for sigmoid sinus - S-shaped continuation leading to the jugular foramen
5. Key Foramina and What Passes Through Them
(From Gray's Anatomy for Students, Table 8.2)
Anterior Cranial Fossa
| Foramen | Structures |
|---|---|
| Foramen cecum | Emissary veins (nasal cavity to superior sagittal sinus) |
| Olfactory foramina (cribriform plate) | Olfactory nerves (CN I) |
Middle Cranial Fossa
| Foramen | Structures |
|---|---|
| Optic canal | Optic nerve (CN II); ophthalmic artery |
| Superior orbital fissure | CN III (oculomotor), CN IV (trochlear), CN V1 (ophthalmic), CN VI (abducent), ophthalmic veins |
| Foramen rotundum | CN V2 (maxillary nerve) |
| Foramen ovale | CN V3 (mandibular nerve); lesser petrosal nerve |
| Foramen spinosum | Middle meningeal artery |
| Foramen lacerum | Internal carotid artery (passes over, not through) |
| Hiatus for greater petrosal nerve | Greater petrosal nerve |
Posterior Cranial Fossa
| Foramen | Structures |
|---|---|
| Foramen magnum | Brainstem/spinal cord junction; vertebral arteries; spinal roots of CN XI; meninges |
| Internal acoustic meatus | CN VII (facial), CN VIII (vestibulocochlear); labyrinthine artery |
| Jugular foramen | CN IX (glossopharyngeal), CN X (vagus), CN XI (accessory); internal jugular vein |
| Hypoglossal canal | CN XII (hypoglossal) |
6. External Skull Base - Key Landmarks
On the external surface of the base of the skull (viewed from below), notable features include:
- Occipital condyles - articulate with the atlas (C1)
- Mastoid process - attachment for sternocleidomastoid and other muscles
- Styloid process - attachment for stylohyoid, styloglossus, stylopharyngeus muscles and ligaments
- Stylomastoid foramen - exit of the facial nerve (CN VII) from the skull
- External acoustic meatus - entry to the ear canal
- Mandibular fossa - articulates with the condyle of the mandible (temporomandibular joint)
7. A Useful 3D Video Resource
Clinical Relevance
- Temporal bone fractures are most common at the thinnest point and can rupture the middle meningeal artery (inside the epidural space) causing an extradural hematoma
- Cribriform plate fractures cause anosmia and CSF rhinorrhoea
- Foramen magnum herniation (tonsillar herniation/"coning") compresses the brainstem
- Battle's sign (bruising over mastoid) and raccoon eyes (periorbital ecchymosis) indicate base of skull fractures
- The diploe and venous sinuses make the skull a site of haematogenous spread of infection
Upper limb anatomy
Finding Sources
Finding Sources
Searching the Web
upper limb anatomy overview bones muscles nerves
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content on the brachial plexus, terminal nerves, and their branches. I have enough information to write a thorough answer on upper limb anatomy. Let me compile the full response now.
Anatomy of the Upper Limb
The upper limb extends from the shoulder girdle to the fingertips and is highly specialised for mobility, dexterity, and fine motor control. It is divided into the shoulder/pectoral girdle, arm (brachium), elbow, forearm (antebrachium), wrist, and hand.
- Gray's Anatomy for Students, pp. 858-865
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
- Rosen's Emergency Medicine, Table 43.1
1. Bones of the Upper Limb
Pectoral Girdle
| Bone | Key Features |
|---|---|
| Clavicle | S-shaped; only bony link between the upper limb and the axial skeleton; fractures most commonly at the junction of middle and lateral thirds |
| Scapula | Triangular flat bone; has the glenoid cavity, acromion, coracoid process, spine, supraspinous and infraspinous fossae |
Arm
- Humerus - long bone with a rounded head articulating with the glenoid cavity; has the greater and lesser tubercles (rotator cuff attachments), the bicipital groove (for the long head of biceps), the deltoid tuberosity, and the medial and lateral epicondyles distally. The surgical neck is where the axillary nerve wraps around.
Forearm
- Radius - lateral bone; has the radial head proximally (articulates with the capitulum of the humerus); the radial styloid process and carpal articular surface distally
- Ulna - medial bone; has the olecranon and coronoid process forming the trochlear notch (articulates with the trochlea of the humerus); the styloid process distally
Wrist and Hand
- 8 Carpal bones (proximal row: scaphoid, lunate, triquetrum, pisiform; distal row: trapezium, trapezoid, capitate, hamate) - mnemonic: She Looks Too Pretty, Try To Catch Her
- 5 Metacarpals
- 14 Phalanges (3 per finger except thumb which has 2)
2. Joints
| Joint | Type | Key Features |
|---|---|---|
| Sternoclavicular | Synovial saddle | Only articulation between upper limb and thorax; has an articular disc |
| Acromioclavicular | Synovial plane | Stabilised by coracoclavicular ligament (conoid + trapezoid) |
| Glenohumeral (shoulder) | Ball and socket | Most mobile but least stable joint; glenoid labrum deepens the socket; 4 rotator cuff muscles stabilise it |
| Elbow | Hinge (trochlea/capitulum) | Includes the radioulnar joint (pivot); anterior capsule is thin, collateral ligaments medially and laterally |
| Radioulnar | Pivot (proximal + distal) | Allow pronation and supination |
| Wrist (radiocarpal) | Condyloid | Radius + articular disc articulate with proximal carpal row |
3. Muscles
Shoulder (Rotator Cuff) - "SITS"
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| Supraspinatus | Supraspinous fossa | Greater tubercle | Initiates abduction (0-15°) | Suprascapular (C5,C6) |
| Infraspinatus | Infraspinous fossa | Greater tubercle | External rotation | Suprascapular (C5,C6) |
| Teres minor | Lateral scapula border | Greater tubercle | External rotation | Axillary (C5,C6) |
| Subscapularis | Subscapular fossa | Lesser tubercle | Internal rotation | Upper/lower subscapular (C5-C7) |
The rotator cuff maintains the head of the humerus in the glenoid cavity; the deltoid provides the bulk of shoulder abduction beyond 15°.
Arm - Anterior Compartment (Flexors - Musculocutaneous nerve, C5-C7)
| Muscle | Action |
|---|---|
| Biceps brachii | Flexion of elbow, supination of forearm, weak shoulder flexion |
| Brachialis | Flexion of elbow (prime mover) |
| Coracobrachialis | Flexion and adduction of arm |
Arm - Posterior Compartment (Extensors - Radial nerve, C6-C8)
| Muscle | Action |
|---|---|
| Triceps brachii (3 heads: long, medial, lateral) | Extension of elbow; long head also extends and adducts arm |
| Anconeus | Assists elbow extension |
Forearm - Anterior Compartment (Flexors/Pronators)
Innervated mostly by the median nerve, except flexor carpi ulnaris and medial half of flexor digitorum profundus (ulnar nerve):
- Superficial: Pronator teres, Flexor carpi radialis, Palmaris longus, Flexor carpi ulnaris
- Intermediate: Flexor digitorum superficialis
- Deep: Flexor digitorum profundus, Flexor pollicis longus, Pronator quadratus
Forearm - Posterior Compartment (Extensors/Supinators)
All innervated by the radial nerve:
- Superficial: Brachioradialis, Extensor carpi radialis longus and brevis, Extensor digitorum, Extensor digiti minimi, Extensor carpi ulnaris
- Deep: Supinator, Abductor pollicis longus, Extensor pollicis longus and brevis, Extensor indicis
Hand Intrinsic Muscles
- Thenar muscles (opponens pollicis, abductor pollicis brevis, flexor pollicis brevis) - median nerve
- Hypothenar muscles (opponens digiti minimi, abductor digiti minimi, flexor digiti minimi) - ulnar nerve
- Lumbricals (1 and 2 = median; 3 and 4 = ulnar) - flex MCPs, extend IPs
- Interossei (all = ulnar nerve) - dorsal interossei abduct, palmar interossei adduct fingers ("DAB/PAD")
- Adductor pollicis - ulnar nerve
4. The Brachial Plexus
The brachial plexus is the nerve network supplying the entire upper limb, formed from the anterior rami of C5 to T1.

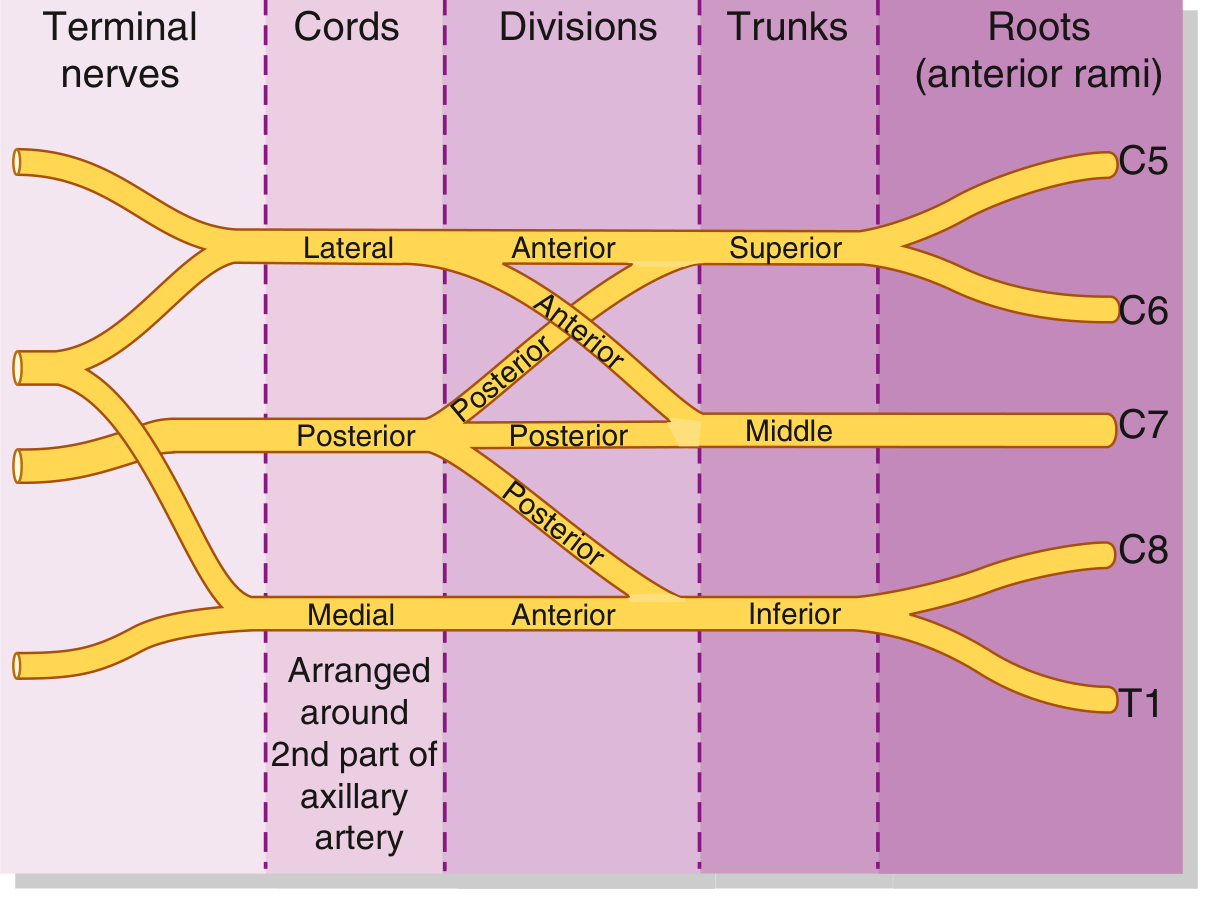
Structure: "Robert Taylor Drinks Cold Beer" (Roots, Trunks, Divisions, Cords, Branches)
| Level | Components |
|---|---|
| Roots | C5, C6, C7, C8, T1 (anterior rami) - pass between anterior and middle scalene muscles |
| Trunks | Superior (C5+C6), Middle (C7), Inferior (C8+T1) |
| Divisions | Each trunk splits into anterior + posterior (6 total) |
| Cords | Lateral (anterior div. of superior + middle), Medial (anterior div. of inferior), Posterior (all 3 posterior div.) - named relative to axillary artery |
| Terminal branches | 5 major nerves (see below) |
Branches and Their Cords of Origin
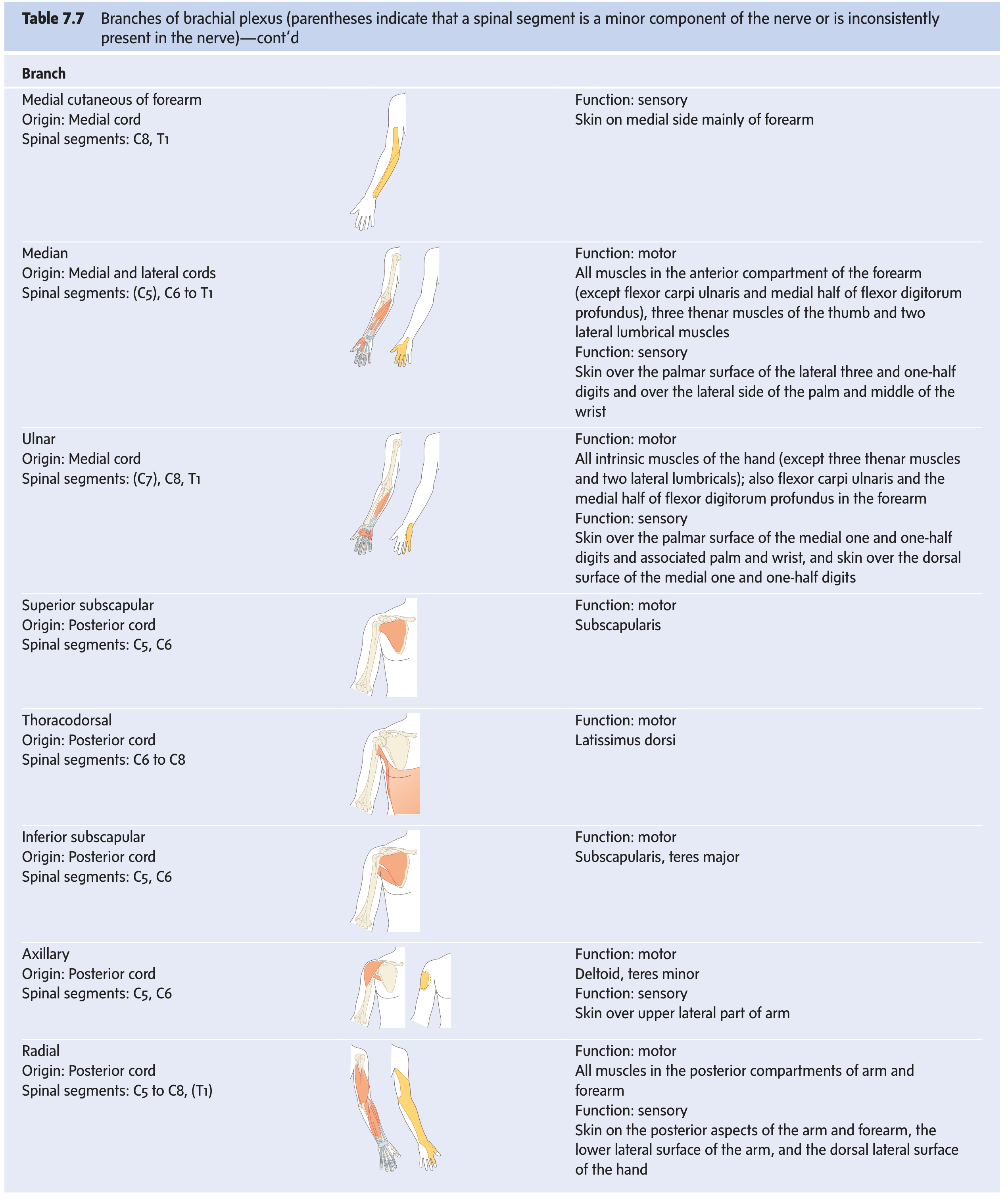
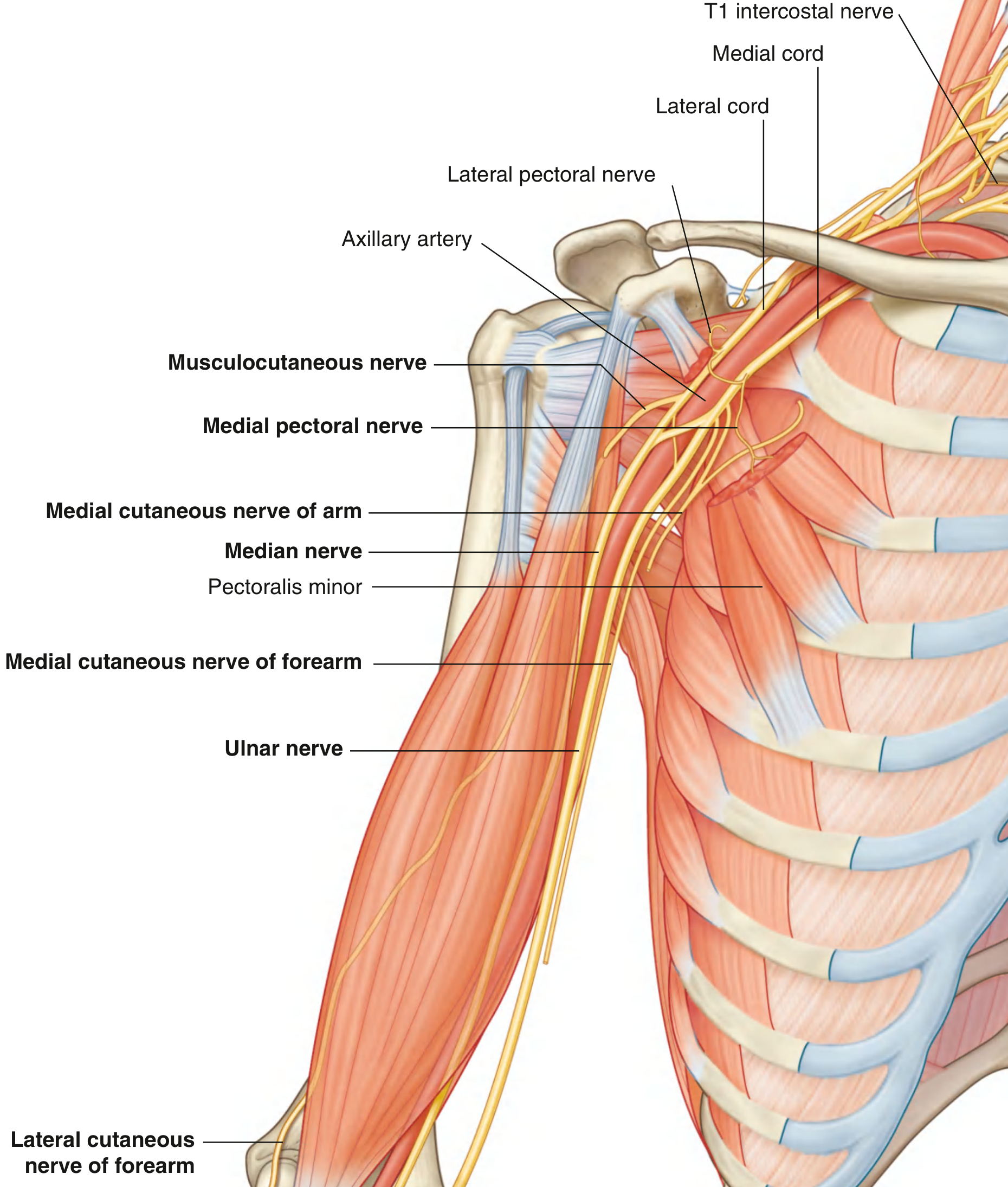
5. The Five Terminal Nerves
| Nerve | Cord | Roots | Motor | Sensory | Key injury |
|---|---|---|---|---|---|
| Musculocutaneous | Lateral | C5-C7 | All anterior arm muscles (biceps, brachialis, coracobrachialis) | Lateral forearm | Coracobrachialis penetration |
| Median | Lateral + Medial roots | C5-T1 | Anterior forearm (except FCU + med FDP), thenar muscles, lateral 2 lumbricals | Palmar lateral 3.5 digits | "Ape hand", carpal tunnel syndrome |
| Ulnar | Medial | C7-T1 | FCU, med FDP, all intrinsics except thenar + lat lumbricals | Medial 1.5 digits (palm + dorsum) | "Claw hand" (ring + little), cubital tunnel |
| Axillary | Posterior | C5-C6 | Deltoid, teres minor | Upper lateral arm | Surgical neck of humerus fracture |
| Radial | Posterior | C5-T1 | All posterior arm and forearm muscles | Posterior arm/forearm, dorsal lateral hand | "Wrist drop", spiral groove fracture |
6. Arterial Supply
The arterial tree of the upper limb runs in a continuous chain:
Subclavian artery → (crosses 1st rib) → Axillary artery → (crosses teres major) → Brachial artery → (bifurcates at the cubital fossa) → Radial artery + Ulnar artery → form the superficial and deep palmar arches in the hand → Digital arteries
Key branches:
- Axillary artery gives off the thoracoacromial, lateral thoracic, and posterior circumflex humeral arteries (the latter accompanies the axillary nerve through the quadrangular space)
- Brachial artery gives off the profunda brachii (deep brachial artery), which accompanies the radial nerve through the spiral groove of the humerus
- At the cubital fossa the brachial artery is medial to the biceps tendon and lateral to the median nerve (from medial to lateral: nerve, artery, tendon)
7. Venous Drainage
Superficial veins (clinically important for IV access)
- Cephalic vein - runs on the lateral side of the arm, drains into the axillary vein; accessible in the deltopectoral groove
- Basilic vein - runs medially, pierces the deep fascia at mid-arm, joins the brachial vein to form the axillary vein
- Median cubital vein - connects cephalic and basilic in the cubital fossa; the preferred site for venepuncture
8. Clinical Correlates - Nerve Injuries
| Injury | Nerve Damaged | Presentation |
|---|---|---|
| Erb-Duchenne palsy (upper trunk injury C5,C6) | Superior trunk | "Waiter's tip" - arm adducted, internally rotated, elbow extended, forearm pronated |
| Klumpke's palsy (lower trunk C8,T1) | Inferior trunk | Intrinsic hand muscle paralysis + "claw hand"; may have Horner's syndrome |
| Wrist drop | Radial nerve (spiral groove) | Inability to extend wrist and fingers; common in humeral shaft fractures |
| Carpal tunnel syndrome | Median nerve | Thenar wasting, loss of opposition; numbness in lateral 3.5 digits |
| Claw hand | Ulnar nerve | Ring + little finger hyperextension at MCP, flexion at IP joints; inability to abduct/adduct fingers |
| Axillary nerve injury | Axillary nerve | Deltoid paralysis (loss of shoulder abduction >15°); loss of sensation over "regimental badge" area |
| Long thoracic nerve injury | Serratus anterior | "Winging of scapula" - medial border protrudes when pushing against a wall |
9. Video Resource
This is a shared conversation. Sign in to Orris to start your own chat.