morphine overdose Management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"opioid overdose"[MeSH Terms] AND "naloxone"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Searching PubMed
"opioid overdose" AND "naloxone" AND management
I now have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Morphine (Opioid) Overdose - Management
Recognition: The Classic Triad
Morphine overdose presents with a characteristic triad:
- Miosis (pinpoint pupils) - mydriasis only appears with severe brain anoxia
- Respiratory depression (slow, shallow respirations; RR <12)
- Reduced consciousness (stupor to coma)
Additional signs: bradycardia, hypothermia, cyanosis, cold/clammy skin. Blood or urine toxicology can confirm the diagnosis but immediate management must be based on clinical findings - do not wait for labs.
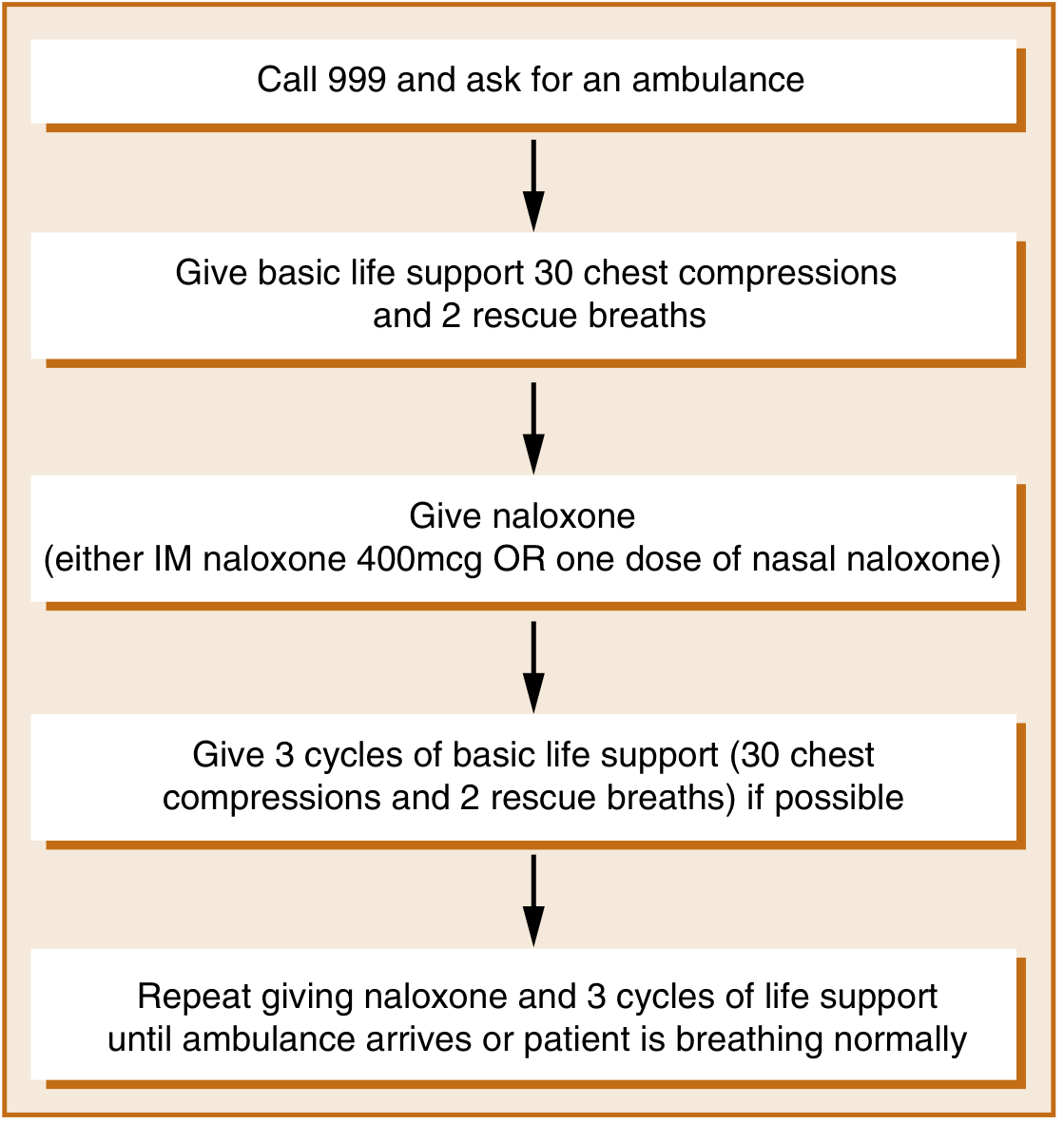
Step 1 - Activate Emergency Services & Basic Life Support
Call emergency services immediately. If the patient is unresponsive and not breathing normally, start BLS (30 chest compressions : 2 rescue breaths) while preparing naloxone.
Step 2 - Secure the Airway
- Position the patient and ensure a patent airway
- Intubation and mechanical ventilation may be necessary if the patient cannot protect their airway or respiratory depression is severe
- Supplemental oxygen
Step 3 - Naloxone (Specific Antidote)
Naloxone is a highly specific opioid receptor antagonist. It rapidly displaces opioid molecules from receptors, reversing respiratory depression and coma within 1-2 minutes of IV administration.
| Route | Dose | Notes |
|---|---|---|
| IV (preferred) | 0.4 - 2.0 mg | Onset ~1-2 min |
| IM | 400 mcg | Good for pre-hospital/community use |
| Intranasal | 2 mg per kit | Equivalent onset to 400 mcg IM, longer peak |
| Endotracheal | 0.4 - 2.0 mg | If no IV/IM access |
Key principles:
- Repeat doses every 2-3 minutes if there is no response; total doses may reach 10 mg or more for high-potency opioids (fentanyl, buprenorphine)
- Goal = reverse respiratory depression, NOT induce full opioid withdrawal. Titrate carefully.
- Naloxone's half-life is shorter than most opioids (morphine, methadone, fentanyl all outlast it) - redosing or infusion is almost always required
Naloxone Continuous Infusion
Because naloxone lasts only a few hours while morphine/methadone last considerably longer, an IV naloxone infusion is frequently employed for 24-72 hours:
"One-half to two-thirds of the initial naloxone dose that reversed the respiratory depression is administered on an hourly basis." - Harrison's Principles of Internal Medicine, 22e
Naloxone is NOT required if the patient has been intubated (mechanical ventilation manages the respiratory depression).
Special Opioid Considerations
- Fentanyl overdose: Naloxone dose may need to be twice the standard dose; newer rescue preparations already contain twice the traditional amount
- Buprenorphine overdose: May require ≥10 mg naloxone total due to high receptor affinity; note that primary buprenorphine overdose is uncommon given its partial agonist ceiling effect
- Methadone overdose: Extremely long duration - requires prolonged naloxone infusion (up to 72 h)
- Meperidine/tramadol overdose: Unique risk of seizures (unlike most opioids)
Step 4 - Vital Signs Support
Beyond naloxone, the following must be managed:
| Problem | Intervention |
|---|---|
| Respiratory failure | Intubation + mechanical ventilation |
| Hypotension | IV fluids; vasopressors if refractory |
| Hypoxia | Supplemental O₂, consider CPAP/BiPAP |
| Bradycardia | Monitor; treat if hemodynamically significant |
| Hypothermia | Active rewarming |
Step 5 - Consider Polydrug Overdose
When naloxone has limited or no effect, consider coingestants:
- Benzodiazepines (most common cointoxicant) - use flumazenil 0.2 mg/min IV (with caution in benzodiazepine-dependent patients due to seizure risk)
- Alcohol, barbiturates, antidepressants
Step 6 - Discharge & Prevention
- Patients discharged on >50 morphine milligram equivalents (MME)/day are at elevated overdose risk and should receive a take-home naloxone prescription
- Patients with opioid use disorder (OUD) should be warned about loss of tolerance after any period of abstinence (e.g., hospitalization, incarceration)
- Naloxone home rescue kits have been shown to reduce opioid overdose mortality
- Consider referral for opioid substitution therapy (OST) with methadone or buprenorphine for ongoing OUD management
Nalmefene - Alternative Reversal Agent
Nalmefene has recently become available as an alternative to naloxone. It has:
- Higher potency than naloxone
- Longer duration of action - useful for long-acting opioid overdoses
- Similar mechanism (pure opioid antagonist)
Summary Table: Management of Opioid Overdose
| Priority | Action |
|---|---|
| 1 | Activate emergency services + BLS if pulseless/apneic |
| 2 | Establish/secure airway; intubate if needed |
| 3 | Naloxone 0.4-2 mg IV/IM/IN; repeat q2-3 min PRN |
| 4 | Start naloxone infusion (2/3 of reversal dose per hour) for 24-72 h |
| 5 | Support BP, temperature, oxygenation |
| 6 | Investigate for polydrug use; consider flumazenil if benzo suspected |
| 7 | Discharge planning with take-home naloxone + OUD referral |
Sources:
- Harrison's Principles of Internal Medicine, 22e (2025), Table 467-2
- Maudsley Prescribing Guidelines in Psychiatry, 15th ed., p. 523-524
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- The Washington Manual of Medical Therapeutics
- Saari TI et al. Clinical Pharmacokinetics and Pharmacodynamics of Naloxone. Clin Pharmacokinet 2024 [PMID: 38485851]
Paracetamol overdose management protocol
Finding Sources
Finding Sources
Searching PubMed
"acetaminophen poisoning"[MeSH Terms] AND "acetylcysteine"[MeSH Terms]
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acetaminophen overdose" AND treatment AND "N-acetylcysteine"
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have everything needed. Let me now compile the comprehensive protocol.
Paracetamol (Acetaminophen) Overdose - Management Protocol
Mechanism of Toxicity
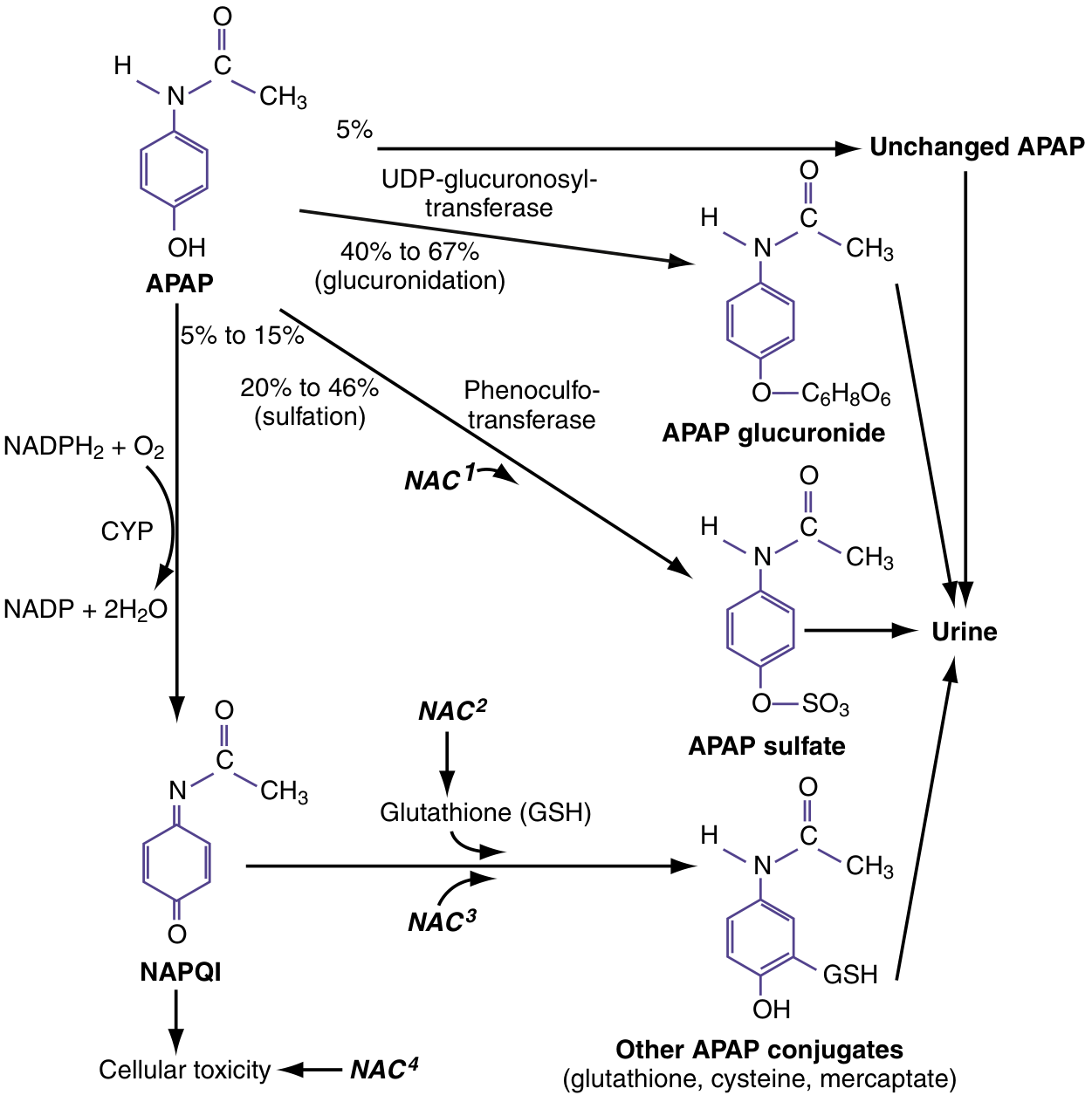
At therapeutic doses, paracetamol is safely conjugated via glucuronidation (40-67%) and sulfation (20-46%). A small fraction (5-15%) is oxidized by CYP450 enzymes to the toxic metabolite NAPQI (N-acetyl-p-benzoquinone imine), which is rapidly neutralized by hepatic glutathione.
In overdose, glucuronidation and sulfation pathways become saturated, shunting more drug through CYP450. NAPQI production overwhelms glutathione stores, and free NAPQI covalently binds hepatocyte proteins, triggering cell death - initially in hepatic zone III (centrilobular).
Clinical Stages
| Stage | Time Course | Name | Symptoms | Signs |
|---|---|---|---|---|
| 1 | 0 - 24-36 h | Pre-injury | Nausea, vomiting, anorexia, malaise, diaphoresis | Elevated serum paracetamol concentration |
| 2 | 8 - 36 h | Liver injury | RUQ pain/tenderness, vomiting, jaundice | Rising AST/ALT, elevated PT/INR, rising bilirubin |
| 3 | 72 - 96 h | Peak injury | Hepatic encephalopathy, coagulopathy | AST/ALT peak; metabolic acidosis, renal injury, fulminant hepatic failure |
| 4 | 4 days - 2 wk | Recovery | Resolution | Aminotransferases return to baseline over 5-7 days; no long-term sequelae |
Key: AST elevates at 8-36 h, peaks at 2-4 days. ALT, PT, and bilirubin peak hours after AST. With massive ingestions, altered mental status and metabolic acidosis can occur very early (serum levels >300-500 mg/L).
Step 1 - Immediate Assessment
Assess time of ingestion and amount - single acute vs. staggered/chronic supratherapeutic ingestion.
Check for high-risk features:
- Chronic alcohol use
- Malnutrition / dehydration
- Hepatic disease
- Concurrent use of CYP450 inducers (isoniazid, rifampicin, carbamazepine, phenytoin, valproic acid)
- Ingestion of other hepatotoxins
Investigations (mandatory for all known or suspected paracetamol exposure):
| Test | Timing | Purpose |
|---|---|---|
| Serum paracetamol level | At 4 hours post-ingestion (or on arrival if >4 h) | Risk stratification via Rumack-Matthew nomogram |
| Serum salicylate | On arrival | Co-ingestion common (OTC confusion) |
| AST, ALT | Baseline + serial | Detect hepatotoxicity |
| PT/INR | Baseline + serial | Coagulopathy marker |
| Bilirubin | Baseline | Liver function |
| Creatinine | Baseline | Renal function |
| Blood glucose | Urgent | Hypoglycaemia in hepatic failure |
| Bicarbonate / ABG | If severe | Metabolic acidosis screening |
Step 2 - Rumack-Matthew Nomogram (Risk Stratification)
Plot the 4-hour serum paracetamol level against time post-ingestion. Treat if the level falls on or above the treatment line.
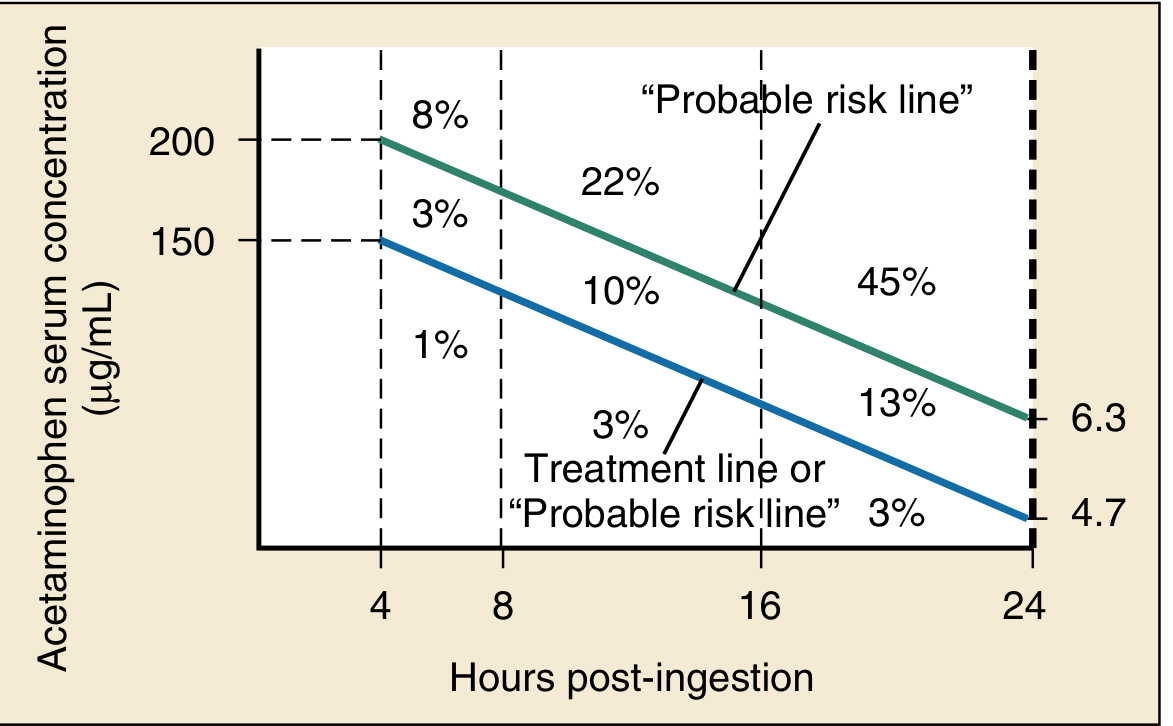
Treatment threshold (UK/international standard):
- 150 mcg/mL (1000 micromol/L) at 4 hours = treatment line
- Cannot be used for staggered ingestions or unknown time of ingestion - in these cases, start NAC empirically pending levels
Step 3 - Decontamination
Activated charcoal (50 g orally):
- Administer within 1-2 hours of ingestion if patient is alert and airway is protected
- Reduces paracetamol absorption by up to 50% if given early
- Do NOT delay NAC to give charcoal
Gastric lavage: not routinely recommended; consider only for massive ingestion within 1 hour.
Step 4 - N-Acetylcysteine (NAC) - The Antidote
NAC is the cornerstone of treatment. It works via four mechanisms:
- GSH precursor - replenishes hepatic glutathione
- Sulfur-containing GSH substitute - directly binds/detoxifies NAPQI
- Enhanced sulfation - diverts APAP away from CYP450 pathway
- Free-radical scavenger / antioxidant - reduces systemic toxicity even after hepatic injury is established
When to start NAC:
- Level on or above the treatment line on nomogram
- Staggered overdose or unknown timing - start empirically
- Any patient with AST >1000 IU/L and suspicion of paracetamol ingestion - even with undetectable serum levels (NAC reduces transplant need and mortality in established hepatic failure)
IV NAC Protocol (Standard 3-bag regimen):
| Phase | Dose | Volume | Duration |
|---|---|---|---|
| Loading | 150 mg/kg | 200 mL 5% dextrose | 60 minutes |
| Second infusion | 50 mg/kg | 500 mL 5% dextrose | 4 hours |
| Maintenance | 100 mg/kg | 1000 mL 5% dextrose | 16 hours |
| Total | 300 mg/kg | 21 hours |
Continue IV NAC beyond 21 hours if:
- AST still rising
- INR > 1.3
- Creatinine elevated
- Patient clinically unwell
Oral NAC (if IV unavailable):
- Loading: 140 mg/kg orally
- Maintenance: 70 mg/kg every 4 hours for 17 doses (total = 72 h course)
- Dilute in juice or soda; serve in covered container through a straw to improve palatability
- Repeat any dose vomited within 1 hour; use ondansetron if vomiting persists
NAC Side Effects:
| Formulation | Common | Severe |
|---|---|---|
| IV NAC | Rash, flushing, pruritus, vomiting (2-18%) | Anaphylactoid reaction: bronchospasm, angioedema, hypotension (<1%) |
| Oral NAC | Vomiting (~15%), sulfur odor/taste | Very rare |
Managing IV NAC anaphylactoid reactions:
- Stop the infusion temporarily
- Treat with antihistamines ± salbutamol (if bronchospasm)
- Restart at a slower rate once reaction resolves
- Do NOT discontinue NAC - the risk of hepatotoxicity far outweighs the infusion reaction risk
Step 5 - Supportive Care
| Complication | Management |
|---|---|
| Nausea / vomiting | Ondansetron IV |
| Hypoglycaemia | 10% dextrose infusion |
| Coagulopathy (without bleeding) | Monitor only; do NOT give FFP unless bleeding or pre-procedure |
| Coagulopathy with active bleeding | FFP, vitamin K |
| Metabolic acidosis | Correct underlying liver failure; consider renal replacement therapy |
| Renal impairment | IV fluids; dialysis if indicated |
| Cerebral oedema (hepatic encephalopathy) | Head elevation, mannitol, intubation/ICP monitoring |
Step 6 - Liver Transplant Referral (King's College Criteria)
Refer to a liver transplant centre if any of the following are met (paracetamol-specific criteria):
| Criterion | Threshold |
|---|---|
| Arterial pH | < 7.30 after resuscitation (most sensitive single predictor) |
| OR all three: INR | > 6.5 |
| Creatinine | > 300 micromol/L |
| Grade III-IV | Hepatic encephalopathy |
Step 7 - Special Populations
| Population | Consideration |
|---|---|
| Pregnancy | NAC is safe - no teratogenic effects reported; use IV formulation; fetal prognosis mirrors maternal outcome |
| Chronic alcohol use | Higher risk due to CYP2E1 induction and depleted glutathione - treat at lower nomogram threshold in some protocols |
| Children (<6 years) | Less susceptible to hepatotoxicity (higher sulfation capacity); same NAC protocol with weight-based dosing |
| Staggered/chronic ingestion | Nomogram not applicable - start NAC empirically and check levels + LFTs |
Quick Reference Summary
1. Secure airway, IV access, baseline bloods
2. Activated charcoal if <2 h post-ingestion and airway protected
3. Serum paracetamol level at 4 h (or on arrival if >4 h)
4. Plot on Rumack-Matthew nomogram
5. Start IV NAC if level on/above treatment line:
150 mg/kg over 1 h → 50 mg/kg over 4 h → 100 mg/kg over 16 h
6. Start NAC empirically if:
- Staggered ingestion / unknown time
- AST >1000 despite undetectable level
7. Serial LFTs, INR, creatinine, glucose
8. Refer to liver unit if King's College Criteria met
9. Psychiatric review before discharge for intentional overdose
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 10e, Ch. 138
- The Washington Manual of Medical Therapeutics
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease
- Maudsley Prescribing Guidelines in Psychiatry, 15th ed.
- Lippincott Illustrated Reviews: Pharmacology
- Tamur S et al. Two vs. Three Infusion Regimens of NAC for Acetaminophen Overdose. Pediatr Rep 2024 [PMID: 38535516]
This is a shared conversation. Sign in to Orris to start your own chat.