Gas gangrene details for emergency medicine
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gas gangrene" OR "clostridial myonecrosis" management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Here is the full clinical reference:
Gas Gangrene (Clostridial Myonecrosis) - Emergency Medicine Reference
Definition
Gas gangrene (clostridial myonecrosis) is a rapidly progressive, life-threatening soft tissue infection characterized by muscle necrosis, gas production in tissues, and systemic toxemia. It is invariably fatal if untreated. - Harrison's Principles of Internal Medicine 22E, p. 1284
Microbiology
| Organism | Context |
|---|---|
| C. perfringens | ~90% of traumatic cases; produces alpha-, beta-, epsilon-, and theta-toxins |
| C. septicum | Spontaneous (non-traumatic) gas gangrene; associated with occult GI malignancy |
| C. novyi, C. sordellii, C. histolyticum | Less common; black-tar heroin injectors |
| Mixed aerobic/anaerobic flora | Common in postoperative and abdominal cases |
C. perfringens is found worldwide in soil and feces. It is a large, gram-positive, spore-forming, anaerobic bacillus with blunt ends. - Red Book 2021, p. 472; Campbell's Operative Orthopaedics 15th Ed 2026
Pathophysiology
C. perfringens produces at least 12 toxins. The two most critical are:
- Alpha-toxin (phospholipase C / lecithinase): Hemolytic, destroys platelets and PMNs, causes widespread capillary damage, forms intravascular platelet-neutrophil aggregates that block inflammatory cell translocation to the infection site.
- Theta-toxin: Synergizes with alpha-toxin in causing irreversible ischemic muscle necrosis, depresses myocardial contractility, and reduces vascular resistance contributing to shock.
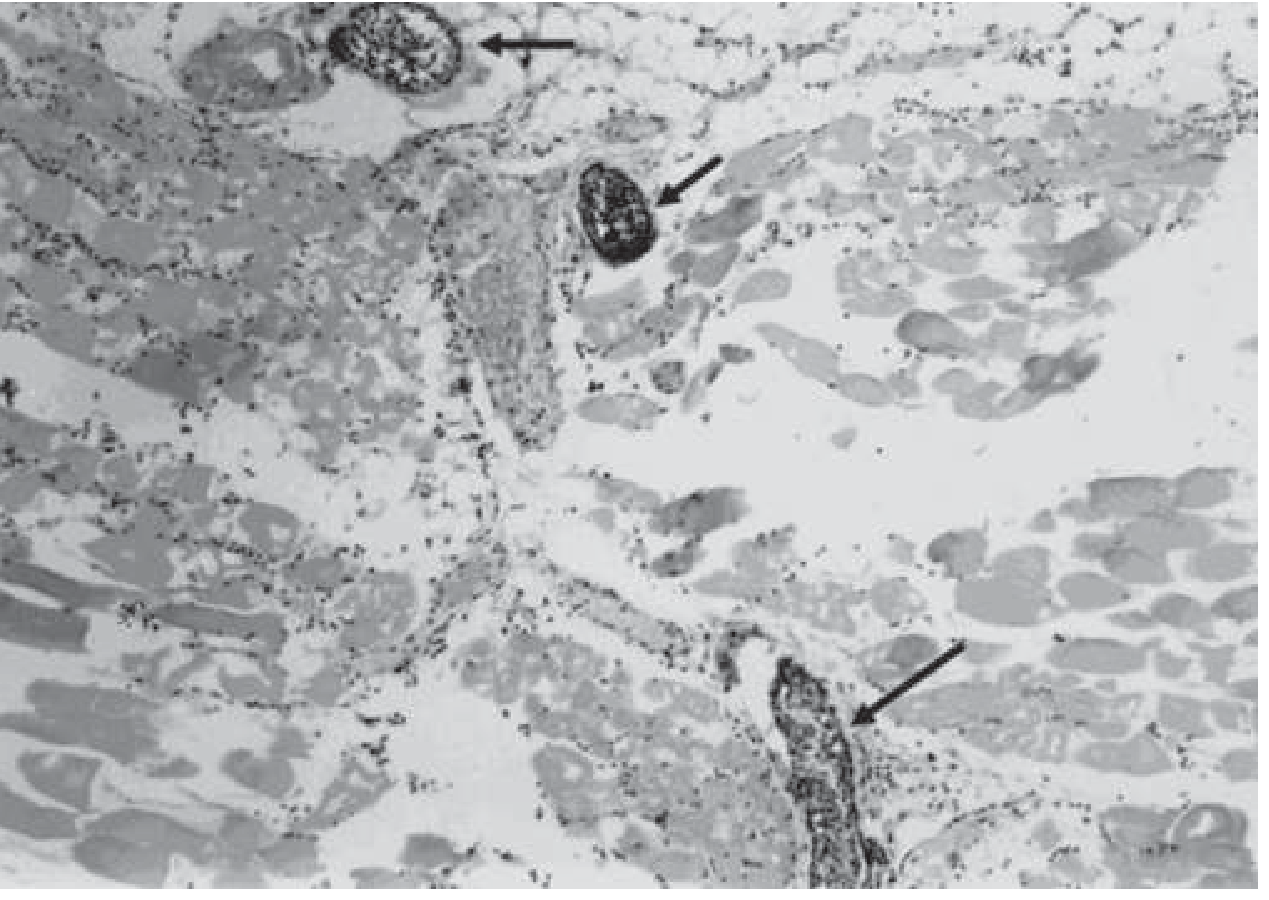
The result is a self-perpetuating cycle: toxins create an anaerobic, low-O2 environment that promotes further clostridial growth and toxin release, even in the absence of an inflammatory response. The characteristic histologic hallmark is widespread necrosis with a paucity of leukocytes in infected tissue and leukocyte accumulation in adjacent vessels. - Goldman-Cecil Medicine, p. 3058; Harrison's 22E
Risk Factors / Predisposing Conditions
Traumatic (most common):
- Crush injuries, open fractures of long bones contaminated with soil/clothing
- Laceration of large/medium arteries (creates ischemia + anaerobic environment)
- Knife or gunshot wounds breaching bowel wall
- Hip surgery, leg amputation for peripheral vascular disease (proximity to fecal flora)
- Adrenaline injections into the buttocks
- Subcutaneous/IM injection of black-tar heroin
Postoperative:
- Bowel or biliary surgery (~30% of cases; bacterial gut translocation)
- Chemotherapy-induced neutropenic enterocolitis (esp. acute leukemia)
Spontaneous (non-traumatic):
- Occult colonic neoplasm (most important - C. septicum bacteremia)
- Inflammatory bowel disease, diverticulitis, necrotizing enterocolitis
- Leukemia, diabetes mellitus, neutrophil dysfunction
Red Book 2021; Harrison's 22E; Goldman-Cecil Medicine
Clinical Presentation
Timeline
| Time | Features |
|---|---|
| Incubation | 6 hours to 4 days (mean <24 h; can be as short as 6 h) |
| Early | Sudden, excruciating pain at wound site - pain out of proportion to appearance |
| Hours later | Tense, exquisitely tender, brawny edema; skin progresses pale → bronze → purple/red/black |
| Wound discharge | "Dishwater" appearance; foul-sweet smell; thin serosanguineous fluid with gas bubbles |
| Skin | Tense bullae filled with bluish-to-maroon fluid → skin sloughing |
| Crepitus | Gas felt under skin (suggestive, not pathognomonic - not always present) |
| Systemic | Tachycardia disproportionate to fever, pallor, diaphoresis → hypotension → multiorgan failure |
Key clinical pearl: The margin between healthy and necrotic tissue can advance several inches (up to 10 cm) per hour despite antibiotics. Muscle involvement is always more extensive than skin changes suggest. - Campbell's Orthopaedics 15th Ed; Red Book 2021
Postoperative clue: Suspect gas gangrene if a surgical site infection develops less than 24 hours after bowel or biliary surgery. - Goldman-Cecil Medicine
Spontaneous type: No preceding wound; abrupt severe muscle pain, rapid edema and bullae. Look for GI malignancy - surviving bacteremia due to C. septicum mandates aggressive GI workup. - Harrison's 22E
Diagnosis
Clinical Diagnosis (Do NOT delay surgery to confirm imaging)
Diagnosis is primarily clinical. Imaging and labs should never delay surgical exploration if suspicion is high.
Gram Stain (Key bedside test)
- Large gram-positive (or gram-variable) rods
- Absence of PMNs (neutrophils) - this is pathognomonic
- Widespread soft tissue necrosis on biopsy
Imaging
- X-ray: Gas in soft tissues (nonspecific, not always present)
- CT/MRI: Best for determining extent of infection along fascial planes; NOT a substitute for surgery
- Needle aspiration or punch biopsy: may provide etiologic diagnosis in ~20% of cases
Intraoperative Findings
- Muscle does not bleed and does not contract when stimulated
- Grossly edematous muscle with reddish-blue to black discoloration
- "Dead muscle" on inspection
Lab/Micro
- Anaerobic cultures: wound exudate, soft tissue/muscle biopsy, blood cultures (bacteremia precedes cutaneous signs in spontaneous type)
- MALDI-TOF: FDA-approved for C. perfringens identification
- Note: Clostridium spp. are ubiquitous; recovery from a wound alone is not diagnostic without clinical correlation
Goldman-Cecil Medicine; Red Book 2021; Harrison's 22E
Emergency Management
1. Immediate Surgery (Most Critical Intervention)
"Radical amputation remains the single best life-saving intervention." - Harrison's 22E, p. 1284
- Emergent surgical debridement of all devitalized tissue - this is the priority
- Resect widely back to healthy, viable, bleeding muscle
- Amputation of a limb may be required to control infection spread
- Fasciotomy if compartment syndrome is present
- Delay wound closure by 5-6 days until confirmed infection-free
- Repeated debridements are often required
- Vacuum-assisted wound closure (VAC) can be used after multiple debridements
2. Antibiotic Therapy
First-line combination (preferred):
- Penicillin G (high-dose IV) + Clindamycin
Rationale for combination:
- Penicillin: active against Clostridium in vitro
- Clindamycin: inhibits bacterial protein/toxin synthesis (ribosomal effect, not cell wall), effective regardless of bacterial load or growth phase, superior efficacy in animal models and some clinical reports
Duration: 10-14 days
Alternatives/Special situations:
| Situation | Antibiotic |
|---|---|
| Penicillin allergy | Clindamycin monotherapy |
| Polymicrobial infection | Beta-lactam/beta-lactamase inhibitor or carbapenem + clindamycin |
| Alternatives (allergy/resistance) | Metronidazole, tetracyclines, chloramphenicol, meropenem, ertapenem |
Resistance note: C. perfringens remains largely susceptible to penicillin (universal susceptibility in most series). Clindamycin resistance has been reported in 3.8% of bloodstream isolates (Canadian study, 2014) and is increasing - check susceptibilities. - Harrison's 22E; Goldman-Cecil Medicine; Red Book 2021
Prophylaxis for grossly contaminated wounds: Penicillin G 50,000 U/kg/day or clindamycin 20-30 mg/kg/day - Red Book 2021
3. Hyperbaric Oxygen (HBO)
- May be beneficial as adjunct by creating a high-O2 environment hostile to obligate anaerobes and may halt alpha-toxin production
- No adequately controlled clinical trial data confirming efficacy
- Should never delay surgical debridement
- Use only when available without compromising surgical timing
4. Supportive ICU Care
- Aggressive fluid resuscitation (refractory hypotension common)
- Treatment of hemolytic anemia (brisk intravascular hemolysis in ~15% of bacteremic patients)
- Renal replacement if acute kidney injury develops
- Standard infection control precautions (no isolation required beyond standard)
Prognosis
- Overall mortality: ~20-40% (historical reports up to 40%; more recent reports show survival rates >90% with aggressive early management)
- Bacteremic patients: mortality >50%
- All patients who died in one series had shock at time of diagnosis; 40% of patients with shock died vs. 20% overall
Worse prognosis: shock at presentation, advanced age, leukopenia, hemolysis, truncal/spontaneous infection
Better prognosis: younger age, single-limb involvement, early aggressive debridement
Goldman-Cecil Medicine; Campbell's Orthopaedics 15th Ed 2026
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Necrotizing fasciitis (Type I - polymicrobial) | Fascia involved more than muscle; mixed flora; slower; LRINEC score useful |
| Necrotizing fasciitis (Type II - Group A Strep) | No gas; toxic shock; GAS on culture |
| Crepitant cellulitis (non-clostridial) | Gas but no myonecrosis; less systemic toxicity; non-clostridial organisms |
| Fournier's gangrene | Perineal/scrotal location; polymicrobial |
| Simple wound contamination with Clostridium | No systemic toxicity, no muscle necrosis; do not over-diagnose |
High-Yield Emergency Medicine Points
- Pain out of proportion to wound appearance is the earliest and most critical warning sign.
- Do not wait for imaging to confirm gas if clinical picture is compelling - go to the OR.
- Gram stain showing gram-positive rods WITHOUT neutrophils is nearly diagnostic.
- The infection can advance 10 cm/hour - time to surgery is paramount.
- Postoperative gas gangrene <24 h after bowel/biliary surgery = high suspicion.
- Spontaneous gas gangrene by C. septicum = find the colon cancer.
- Amputation is life-saving and should not be delayed out of reluctance.
- Combination penicillin G + clindamycin is the regimen of choice; clindamycin's toxin-inhibiting mechanism is the key rationale.
- HBO is adjunctive only - never let it delay the OR.
- IVDU (black-tar heroin) is a modern risk factor for cutaneous/soft tissue gas gangrene.
Recent Literature
Two recent reviews are available on this topic:
- Clostridial Myonecrosis: Toxin Pathophysiology and Management (2024) - Microorganisms (PMID 39065232)
- Hyperbaric Oxygen in Necrotizing Soft Tissue Infections (2025) - J Clin Med (PMID 40429506) - provides the most current review of HBO evidence
Sources: Harrison's Principles of Internal Medicine 22E (2025), Goldman-Cecil Medicine International Edition, Campbell's Operative Orthopaedics 15th Ed (2026), Red Book 2021, Pye's Surgical Handicraft 22nd Ed, Bailey & Love's Short Practice of Surgery 28th Ed, Fitzpatrick's Dermatology
This is a shared conversation. Sign in to Orris to start your own chat.