Iontophorosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive overview of iontophoresis drawn from multiple authoritative textbooks:
Iontophoresis
Definition & Mechanism
Iontophoresis uses direct electrical current (DC) to enhance the diffusion and absorption of charged medications or ions across the skin and mucous membranes. The fundamental principle is electrostatic repulsion: charged ions in solution are driven away from a like-charged electrode, forcing them into tissue.
- Penetration depth: 0.2 to 1.5 cm, depending on drug and tissue characteristics
- Drug delivery rate is generally proportional to the applied current, enabling programmable delivery
- For hyperhidrosis: the exact mechanism is not fully understood, but hypotheses include disruption of ion channels occluding the sweat gland, inhibition of sympathetic nerve transmission, and local pH changes affecting eccrine gland function
(Fitzpatrick's Dermatology; Dermatology 2-Volume Set 5e; Pfenninger & Fowler's Procedures for Primary Care)
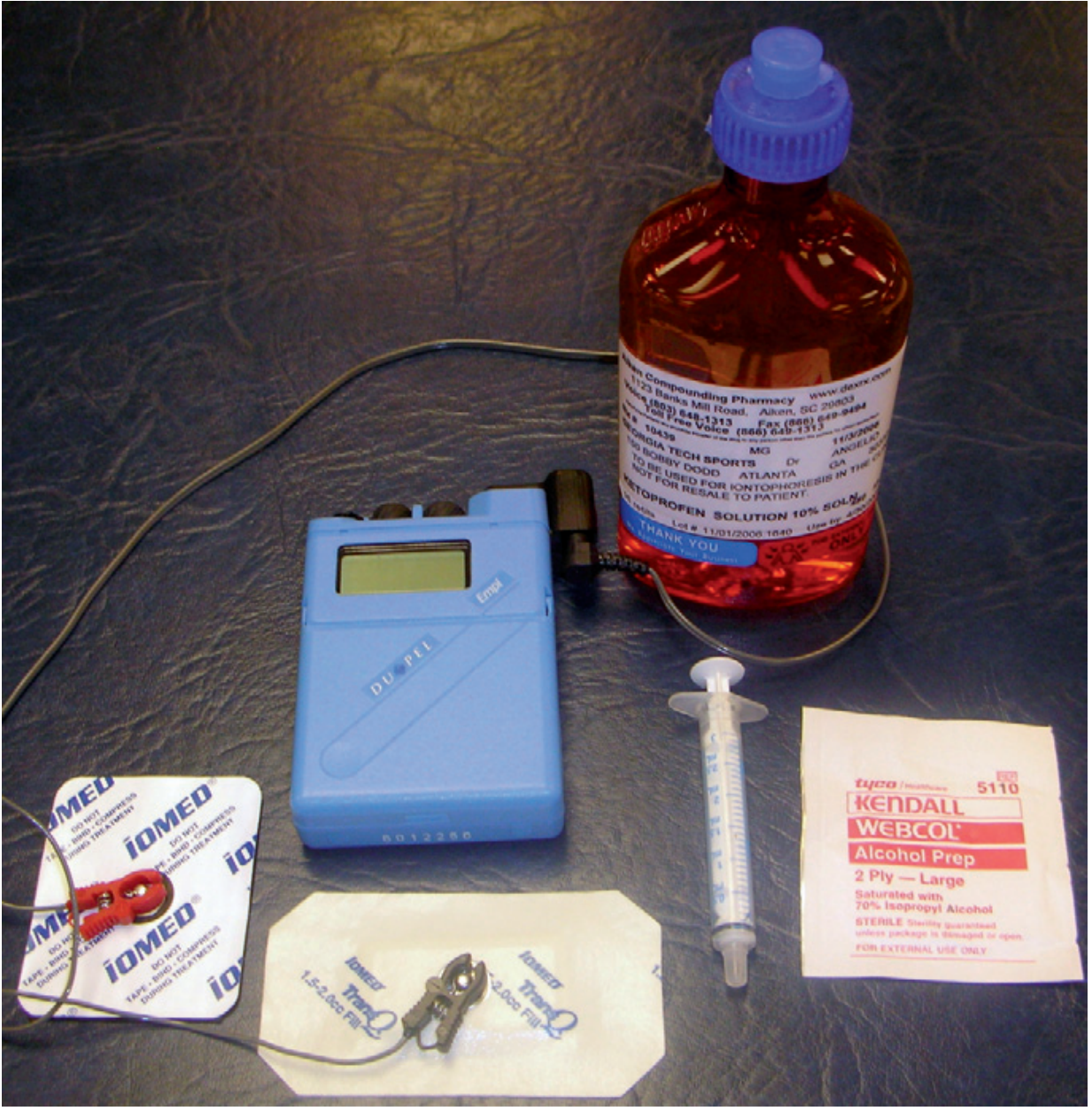
Equipment
- Direct-current (DC) generator with constant current output (calibrated in milliamperes)
- Active and dispersive electrodes
- Appropriate medications and coupling medium
- Alternatively: wearable, battery-powered iontophoresis patches (0.06–0.45 mA over 3–24 hours)
Current Parameters
| Parameter | Value |
|---|---|
| Current intensity | 0.1–4 mA (standard); up to 20 mA (hyperhidrosis) |
| Duration | 10–20 minutes per session |
| Dosage unit | mA × min (current × time) |
| Frequency | 3–8 sessions depending on response |
For hyperhidrosis, cessation of sweating typically requires 20 mA for 30 minutes daily.
Indications
Primary Therapeutic Applications
| Ion / Drug | Polarity | Therapeutic Use | Dose |
|---|---|---|---|
| Dexamethasone | Negative | Tendinitis, tenosynovitis, bursitis, arthritis | 1–4 mA × 15–20 min |
| Lidocaine 4% | Positive | Skin anesthesia (pre-procedural) | 4 mA × 20–30 min |
| Acetic acid | Negative | Calcified tendinitis, calcium deposits | 3–4 mA × 10–20 min |
| Sodium chloride | Negative | Keloids, scar tissue | 4 mA × 20–45 min |
| Copper sulfate | Positive | Fungal infection | 4 mA × 20–30 min |
| Hyaluronidase | Positive | Edema, lymphedema, scleroderma | 1–2 mA × 20–40 min |
| Iodine | Negative | Fibrosis, scar tissue, trigger finger | 2 mA × 1 min → 4 mA × 5 min |
| Methylprednisolone | Negative | Postherpetic neuralgia | 1–4 mA × 15–20 min |
| Salicylate | Negative | Analgesia, myalgia, plantar warts | 4 mA × 45 min |
| Zinc | Positive | Wound healing, ulcers | 4 mA × 15 min |
| Tap water | — | Palmoplantar/axillary hyperhidrosis | 20 mA × 30 min |
| Pilocarpine | Positive | Sweat stimulation (cystic fibrosis sweat test) | — |
| Glycopyrrolate (additive) | — | Enhances hyperhidrosis treatment | — |
Other Uses (limited evidence)
Ganglion cysts, ischemic ulcers, neuromas, post-traumatic edema, tinea pedis, warts, wound healing.
In Emergency Medicine
Lidocaine with epinephrine via iontophoresis provides adequate needle-free anesthesia before venipuncture in pediatric patients and is superior to EMLA for cutaneous anesthesia.
Contraindications
- Known allergy to the therapeutic agent
- Patients with cardiac pacemakers or other implanted electrical devices
- Application over the heart or carotid sinus
- Areas of abnormal skin sensation (impaired feedback → risk of overdosage)
- Superficial abrasions, cuts, bruises, or areas of recent bleeding
- Areas near embedded metallic objects (wires, screws, staples)
- Recent scars or skin grafts
Technique (Step-by-Step)
- Obtain prescription (if administered by a physical therapist)
- Position patient; inspect skin for contraindications
- Clip excess hair; clean area with 70% isopropyl alcohol
- Inject premeasured medication into the electrode reservoir
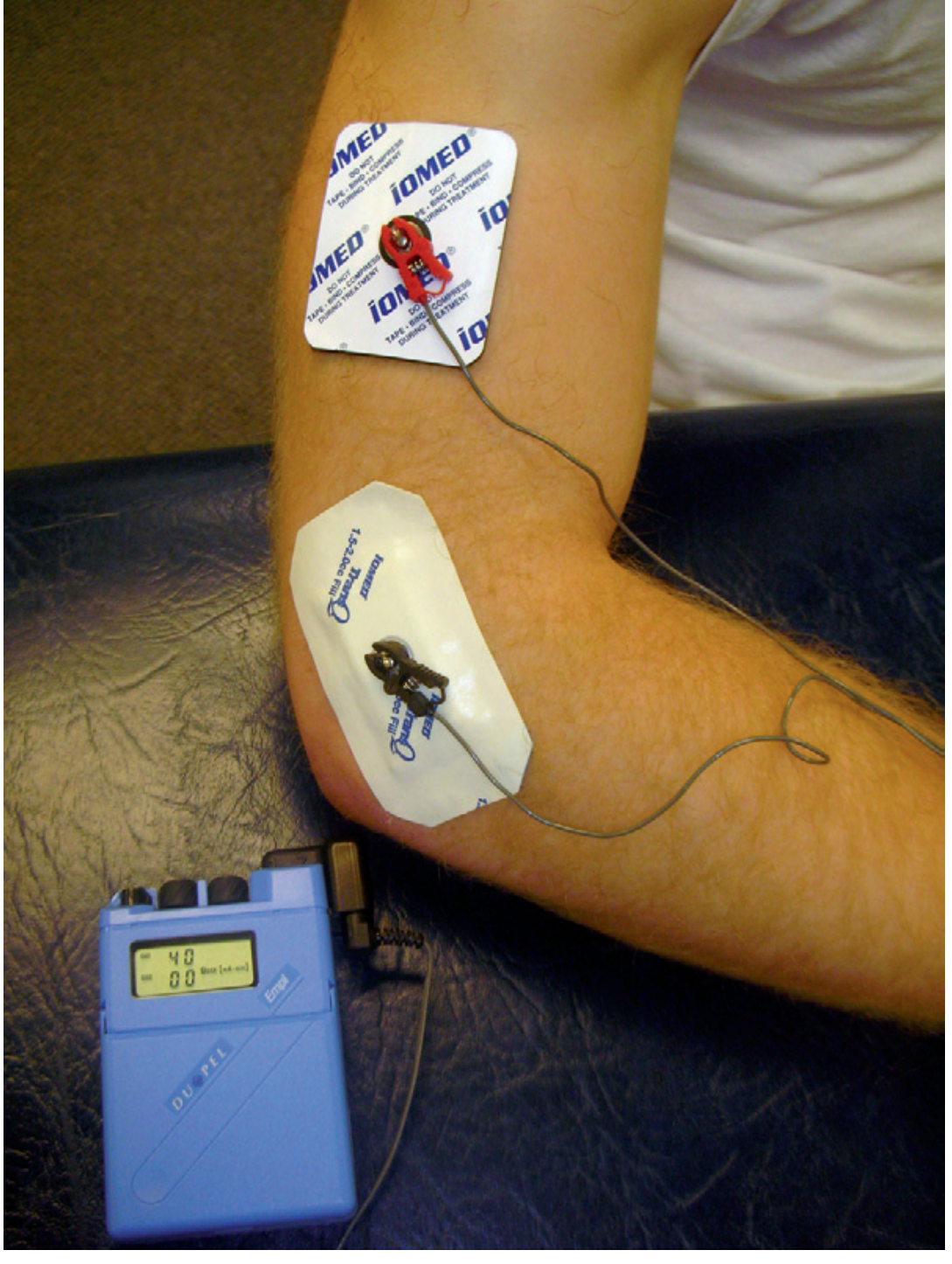
- Apply active electrode over treatment site; place dispersive electrode nearby
- Connect leads; set current to 0.1–4 mA
- Calculate dose (mA × min) based on diagnosis and Table 229-1
- Gradually increase current until patient barely feels tingling (sudden changes cause burning/stinging)
- Monitor patient every 2–4 minutes for adverse effects
- Remove electrodes when complete; advise patient to report delayed reactions
- Post-treatment erythema is common (pH change or histamine reaction)
Adverse Effects
| Effect | Cause |
|---|---|
| Skin irritation, erythema | Galvanic reaction, pH change |
| Hyperesthesia / tingling | Current stimulation |
| Blisters | Excessive current |
| Galvanic rash | Hypersensitivity to DC (within 5 min) |
| "Negative electrode burn" | Alkaline reaction at cathode (reduced by modern pH-stabilized electrodes) |
| Twitch response | Inadvertent nerve stimulation |
| Drug allergy/sensitivity | Previously unknown reaction |
Special Applications
Hyperhidrosis
Tap water (or tap water + glycopyrrolate) iontophoresis is used for palmar, plantar, and axillary hyperhidrosis. Tap water iontophoresis works best on palmar and plantar surfaces. A battery-powered home unit (Drionic®) is available. Botulinum toxin has since become a more efficient and longer-lasting alternative.
Sweat Chloride Test (Cystic Fibrosis Diagnosis)
Iontophoresis of pilocarpine nitrate is Step 1 of the standard sweat test to stimulate localized sweating for chloride collection.
Reverse Iontophoresis
Used in research/clinical glucose monitoring — extracts glucose from the skin non-invasively (e.g., GlucoWatch technology).
Drug Delivery Research
Miniaturized microprocessor systems now allow programmable, wearable iontophoretic drug delivery (fentanyl, sumatriptan for migraine, lidocaine, pilocarpine).
Sources:
- Fitzpatrick's Dermatology, Vol. 1–2
- Dermatology 2-Volume Set 5e (Chapter 124)
- Pfenninger and Fowler's Procedures for Primary Care, 3rd ed. (Chapter 229)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Tietz Textbook of Laboratory Medicine, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.