Discuss Cutaneous Tuberculosis in 10marks for 3rd yr dermatology post graduate theory examination
Reading File
Finding Sources
Finding Sources
Searching PubMed
cutaneous tuberculosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
lupus vulgaris cutaneous tuberculosis skin
Reading File
Loading Image
Loading Image
I have comprehensive content from three authoritative dermatology textbooks. Now I'll compose a thorough 10-mark exam answer.
Cutaneous Tuberculosis
Introduction
Cutaneous tuberculosis (CTB) is infection of the skin caused by Mycobacterium tuberculosis, Mycobacterium bovis, or, occasionally, the attenuated bacille Calmette-Guérin (BCG) strain. It constitutes 1–2% of all tuberculosis cases worldwide and has resurged due to the HIV/AIDS epidemic, emergence of drug-resistant strains, and immigration from high-prevalence countries. — Fitzpatrick's Dermatology, Vol. 1&2
Etiology and Pathogenesis
M. tuberculosis is an acid- and alcohol-fast, obligate intracellular bacillus. The skin is infected by three routes:
- Exogenous inoculation — direct entry through a break in skin
- Endogenous spread — contiguous extension or autoinoculation from an internal TB focus
- Hematogenous dissemination — bacteremic seeding of the dermis
The host immune status is the single most important determinant of which clinical form develops. High cell-mediated immunity (CMI) → paucibacillary, localised disease (e.g., TB verrucosa cutis, lupus vulgaris); poor CMI → multibacillary, disseminated disease (e.g., miliary TB, orificial TB). — Andrews' Diseases of the Skin
Classification
| Route | Immune Status | Clinical Form |
|---|---|---|
| Exogenous | Naïve (non-immune) | Primary inoculation TB (tuberculous chancre) |
| Exogenous | High (sensitized) | TB verrucosa cutis |
| Endogenous – contiguous | Variable | Scrofuloderma |
| Endogenous – autoinoculation | Low | Orificial (periorificial) TB |
| Haematogenous | High | Lupus vulgaris |
| Haematogenous | Low/absent | Acute miliary TB, Tuberculous gumma |
| Tuberculids | High (hypersensitivity) | Papulonecrotic tuberculid, Lichen scrofulosorum, Erythema induratum |
— Fitzpatrick's Dermatology, Table 157-1
Clinical Forms
1. Primary Inoculation TB (Tuberculous Chancre)
Occurs 2–4 weeks after inoculation in a non-immune host. A painless, firm, red-brown papulonodule slowly erodes to form a sharply demarcated ulcer. Regional lymphadenopathy develops — analogous to the pulmonary Ghon complex. Heals spontaneously in 3–12 months, leaving an atrophic scar. Tuberculin test (TST) converts from negative to positive as immunity develops.
2. TB Verrucosa Cutis
Results from exogenous inoculation in a sensitized (immune) host. Prototype: "prosecutor's/pathologist's wart" — inoculation during post-mortem. Clinically: a small, asymptomatic, wart-like indurated papule that enlarges peripherally into a firm reddish-brown verrucous plaque. Surface may fissure, discharging purulent/keratinous debris. Sites: dorsum of fingers and hands (adults), ankles and buttocks (children). TST strongly positive.
Histology: Pseudoepitheliomatous hyperplasia, hyperkeratosis, suppurative and granulomatous inflammation in dermis. AFB scanty; culture positive in ~50%.
3. Scrofuloderma
The most common form in developing countries. Develops from contiguous spread from underlying TB lymph nodes (most common), bones, joints, or epididymis. Begins as a firm subcutaneous cold abscess → becomes fluctuant → ruptures → forms ulcers and sinus tracts. Ulcer edges are undermined, violaceous/blue, with soft granulation tissue at the base. On healing: keloids and retracted tethered scars.
Histology: Suppurative necrosis at centre, tuberculous granulomas at periphery.
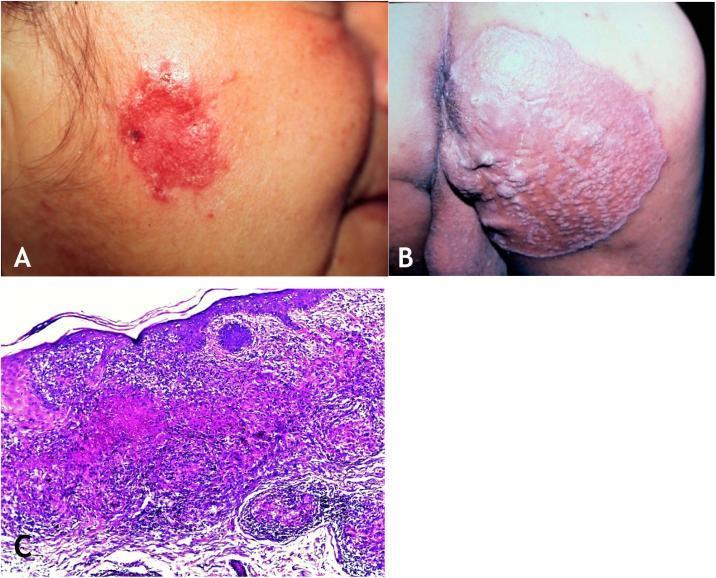
4. Lupus Vulgaris (LV)
The most common form in Europe; more common in women. Occurs at sites of prior inoculation, scrofuloderma scars, or by hematogenous spread. ~50% have evidence of TB elsewhere. TST strongly positive.
Classic lesion: A single, slowly enlarging plaque composed of grouped red-brown "lupomas" (soft translucent papules). Pathognomonic sign: "apple-jelly" colour on diascopy (blanching reveals pale yellow-brown nodules — epithelioid granulomas in dermis).
Morphological variants: plaque (most common), hypertrophic/verrucous, ulcerative, atrophic/scarring, papular/nodular.
Sites: head and neck (most common — nose, cheek, ear), buttocks, extremities.
Complications: squamous cell carcinoma (5–10% of long-standing LV), contractures, lymphoedema, destruction of nose/ear cartilage.

Histology: Tuberculoid granulomas (epithelioid cells + Langhans giant cells) with minimal or absent caseation. AFB rarely found. As shown below:
5. Orificial (Periorificial) TB
Results from autoinoculation from advanced internal TB (pulmonary, intestinal, anogenital). Affects individuals with severely impaired CMI. Presents as painful ulcers at or around the mouth, anus, or genitalia. Lesions are recalcitrant and do not heal spontaneously. TST may be negative.
6. Acute Miliary TB
Rare; occurs in infants and severely immunosuppressed adults. Haematogenous seeding produces widespread small erythematous papules, vesicles, or haemorrhagic pustules. TST is usually negative. AFB abundant on biopsy.
7. Tuberculous Gumma (Metastatic Tuberculous Abscess)
Results from haematogenous spread in patients with compromised immunity. Forms a painless, fluctuant subcutaneous abscess that may ulcerate and discharge. TST may be negative.
Tuberculids
Tuberculids are hypersensitivity eruptions that represent the skin's response to haematogenous dissemination of TB antigen in persons with high immunity. Bacilli are rarely cultured. Characteristic features: bilateral symmetry, TST strongly positive, resolution with anti-TB therapy, and often PCR-detectable mycobacterial DNA.
| Type | Features |
|---|---|
| Papulonecrotic tuberculid | Recurrent, symmetrical, asymptomatic necrotic papules on extensor extremities (elbows, knees, dorsal hands/feet); heals with varioliform scars; ♀ > ♂ (3:1) |
| Lichen scrofulosorum | Asymptomatic, lichenoid, perifollicular papules in a grouped/discoid pattern on trunk; associated with TB lymphadenitis or bone TB |
| Erythema induratum (Bazin's disease) | Tender, deep nodules on posterior calves → ulcerate; predominantly in women; shows lobular panniculitis with granulomas on histology |
Diagnosis
| Investigation | Comment |
|---|---|
| Tuberculin skin test (TST/Mantoux) | Strongly positive in LV, TB verrucosa cutis, scrofuloderma, tuberculids; may be negative in miliary TB, orificial TB |
| IGRA (QuantiFERON-TB Gold, T-SPOT) | More specific than TST in BCG-vaccinated individuals; preferred when TST is unreliable |
| Skin biopsy (H&E) | Tuberculoid granulomas ± caseation (hallmark); Ziehl-Neelsen stain for AFB |
| AFB culture (Lowenstein-Jensen medium) | Gold standard for diagnosis and drug sensitivity; takes 4–8 weeks |
| PCR | Detects mycobacterial DNA; 100% sensitivity/specificity in multibacillary forms; 55% sensitivity in paucibacillary disease |
| Chest X-ray / systemic workup | Mandatory; especially in LV (50% have associated internal TB) |
Treatment
Treatment of CTB follows the same principles as pulmonary TB. — Fitzpatrick's Dermatology
Standard regimen:
- Intensive phase (2 months): Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) → 2HRZE
- Continuation phase (4 months): Isoniazid + Rifampicin → 4HR
- Total duration: 6 months for most forms
Special considerations:
- Localised TB verrucosa cutis or LV without internal TB: may be treated with isoniazid alone for up to 12 months
- Therapy should continue for at least 2 months after complete involution of skin lesions (viable organisms can persist in clinically healed lesions)
- Scrofuloderma: surgical excision reduces morbidity and shortens chemotherapy duration
- Small LV lesions: surgical excision with concomitant anti-TB drugs
- MDR-TB: resistant to ≥ isoniazid + rifampicin → second-line agents (fluoroquinolones, injectable agents)
- XDR-TB: additional resistance to any fluoroquinolone + at least one injectable agent (capreomycin, kanamycin, or amikacin)
Summary Table — Key Differentiating Features
| Feature | Chancre | TB verrucosa cutis | Scrofuloderma | Lupus vulgaris | Orificial TB | Miliary TB |
|---|---|---|---|---|---|---|
| Immunity | Naïve | High | Variable | High | Low | Very low |
| Source | Exogenous | Exogenous | Endogenous | Haematogenous | Autoinoculation | Haematogenous |
| Bacilli load | High | Low | Moderate | Very low | High | Very high |
| TST | Becomes + | Strongly + | Usually + | Strongly + | Often – | Often – |
| AFB on biopsy | + | Rare | Occasional | Rare | + | + |
Complications of Lupus Vulgaris (High-yield)
- Squamous cell carcinoma (5–10% in longstanding disease)
- Disfigurement: destruction of nasal/auricular cartilage
- Contractures and lymphoedema
- Rarely: basosquamous carcinoma, sarcoma
Sources: Dermatology 2-Volume Set, 5e (Bolognia); Fitzpatrick's Dermatology, Vol. 1&2; Andrews' Diseases of the Skin, Clinical Dermatology
This is a shared conversation. Sign in to Orris to start your own chat.