Teach me about most common ecg
Reading File
Finding Sources
Searching the Web
most common ECG patterns clinical interpretation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Searching Images
ECG normal sinus rhythm P wave QRS T wave
Searching Images
atrial fibrillation ECG irregular rhythm absent P waves
Searching Images
STEMI ST elevation myocardial infarction ECG
Searching Images
left bundle branch block right bundle branch block ECG comparison
Searching Images
AV heart block first degree second degree third degree ECG
Now I have plenty of material. Let me compile a comprehensive ECG teaching guide.
ECG: A Comprehensive Guide to the Most Common Patterns
1. The Normal ECG — Understanding the Baseline
Before recognizing abnormalities, you must master the normal tracing.
The Cardiac Cycle & ECG Waveforms

| Wave/Interval | What It Represents | Normal Values |
|---|---|---|
| P wave | Atrial depolarization (SA node → atria) | Duration < 0.12 s; upright in I, II, aVF |
| PR interval | AV nodal conduction delay | 0.12–0.20 s (3–5 small boxes) |
| QRS complex | Ventricular depolarization | < 0.12 s (3 small boxes) |
| ST segment | Early ventricular repolarization | Isoelectric (flat) |
| T wave | Ventricular repolarization | Upright in most leads |
| QT interval | Total ventricular depolarization + repolarization | < 0.44 s (rate-corrected QTc) |
ECG Paper Calibration
- Horizontal axis: 1 small box = 0.04 s; 1 large box = 0.20 s
- Vertical axis: 1 mm = 0.1 mV
- Rate formula: Rate = 300 ÷ (number of large boxes between R-R intervals)
Normal Sinus Rhythm (NSR) — The Template
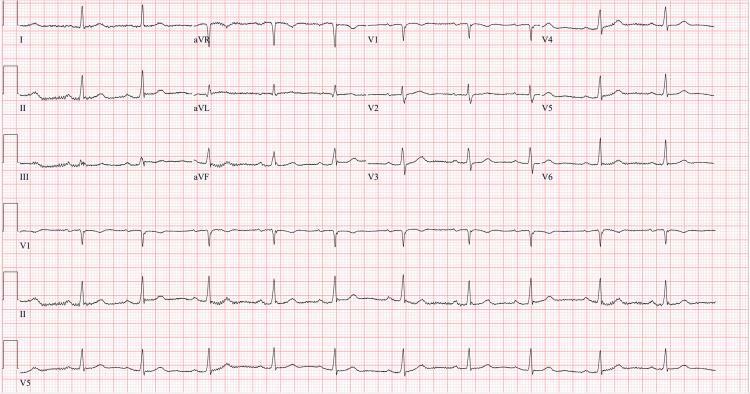
Criteria:
- P wave before every QRS
- Regular R-R intervals
- Rate 60–100 bpm
- Normal PR interval (0.12–0.20 s)
- Normal QRS morphology with R-wave progression V1→V6
The 5-Step Interpretation Approach
- Rate — 300/large boxes between R waves
- Rhythm — regular vs. irregular; P wave present?
- Axis — normal (−30° to +90°); left or right deviation?
- Intervals — PR, QRS, QT within normal limits?
- Morphology — ST segments, T waves, Q waves, R-wave progression
2. Arrhythmias
2a. Atrial Fibrillation (AF) — Most Common Sustained Arrhythmia
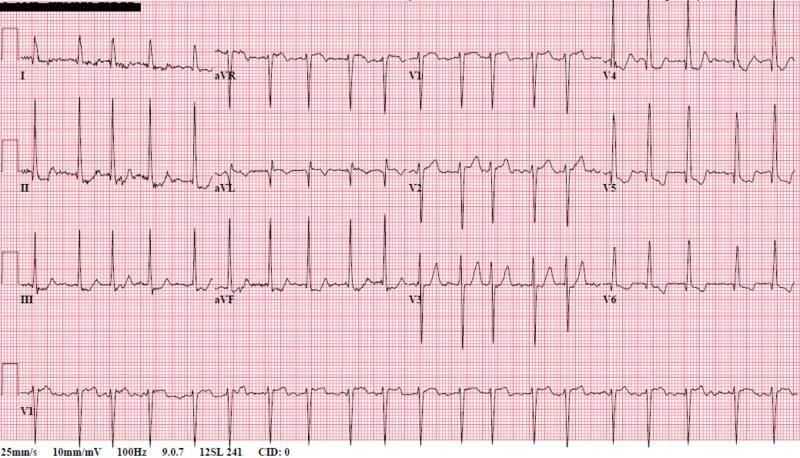
ECG Hallmarks:
- Absent P waves — replaced by fine chaotic fibrillatory (f) waves
- Irregularly irregular R-R intervals (no two R-R intervals are equal)
- Narrow QRS (unless aberrant conduction)
- Ventricular rate typically 100–160 bpm if untreated (AF with rapid ventricular response)
Causes: hypertension, valvular disease, heart failure, thyrotoxicosis, alcohol (holiday heart), ischemia
2b. AV Blocks
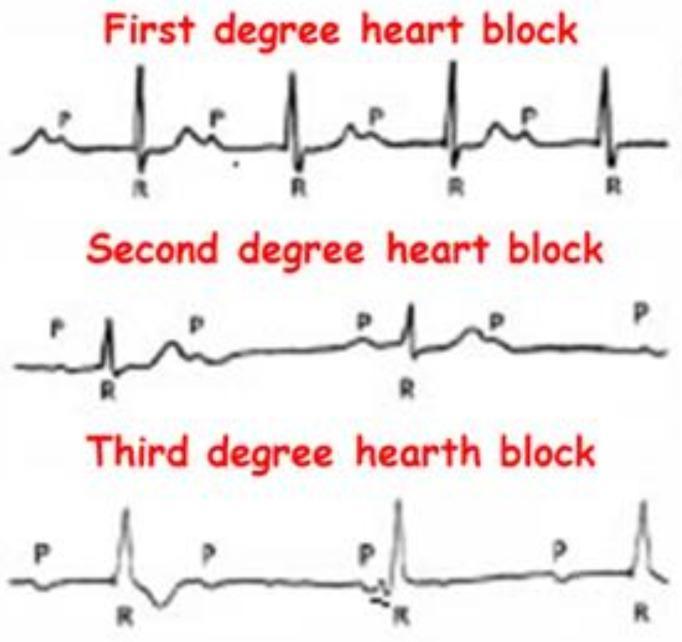
| Type | ECG Feature | Clinical Significance |
|---|---|---|
| 1st Degree | PR > 0.20 s (>1 large box); every P conducts | Benign; no treatment usually needed |
| 2nd Degree — Mobitz I (Wenckebach) | Progressive PR lengthening → dropped QRS | Usually at AV node; benign; often inferior MI |
| 2nd Degree — Mobitz II | Fixed PR; sudden dropped QRS (no warning) | Below His bundle; can progress to complete block |
| 3rd Degree (Complete) | P waves and QRS completely dissociated; AV dissociation; slow escape rhythm | Emergency — pacemaker needed |
From Morgan and Mikhail's Clinical Anesthesiology: Mobitz II nearly always reflects infra-Hisian conduction disease and frequently progresses to complete AV block, especially after anterior MI.
3. Conduction Abnormalities — Bundle Branch Blocks
3a. Right Bundle Branch Block (RBBB)
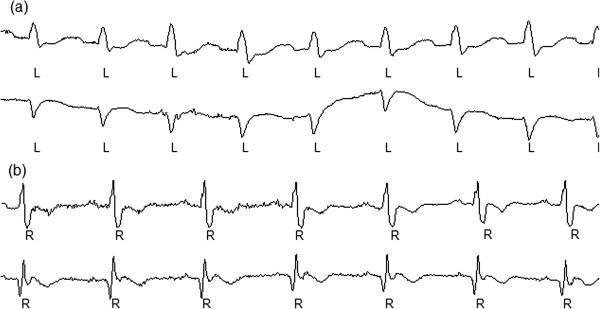
ECG Criteria:
- QRS ≥ 0.12 s (≥ 3 small boxes)
- rSR' ("M-shape") pattern in V1
- Wide, slurred S wave in I and V6
- Discordant ST-T changes in V1–V2
Mnemonic: "MaRRoW" — in RBBB, look for the M in V1 (right), the W in V6 (left)
Clinical significance: Can be congenital or represent organic heart disease; alone with normal PR interval, rarely progresses to complete block.
3b. Left Bundle Branch Block (LBBB)
ECG Criteria:
- QRS ≥ 0.12 s
- Broad notched R without q in I, aVL, V5–V6 ("W" pattern in V1)
- rS or QS in V1
- Discordant ST-T changes throughout V1–V6
Mnemonic: "WiLLiaM" — in LBBB, W in V1, M in V6
From Goldman-Cecil Medicine and Morgan and Mikhail's: LBBB almost always indicates underlying organic heart disease and masks ischemic changes — a new LBBB in chest pain should be treated like a STEMI.
Bundle Branch Block ECG Criteria Summary (from Goldman-Cecil Medicine):
| QRS Duration | Axis | Key Morphology | |
|---|---|---|---|
| RBBB | ≥ 0.12 s | Normal | rSR' in V1; wide S in I, V6 |
| LBBB | ≥ 0.12 s | Variable | Broad notched R in I, V5–V6; rS in V1 |
| LAFB | < 0.12 s | −45° to −90° | qR in aVL; left axis deviation |
| LPFB | < 0.12 s | +90° to +180° | Right axis deviation; rS in I, aVL |
4. Ischemia & Infarction
STEMI (ST-Elevation Myocardial Infarction)

ECG criteria for STEMI:
- New ST elevation ≥ 1 mm in ≥ 2 contiguous limb leads
- Or ≥ 2 mm in ≥ 2 contiguous precordial leads
- Convex (tombstone) morphology
- Reciprocal ST depression in opposite leads
Localizing the Infarct by Leads:
| Lead Group | Territory | Culprit Artery |
|---|---|---|
| V1–V4 | Anterior wall | LAD (left anterior descending) |
| I, aVL, V5–V6 | Lateral wall | LCx (left circumflex) |
| II, III, aVF | Inferior wall | RCA (right coronary artery) |
| V1–V2 (tall R, ST depression) | Posterior wall | RCA or LCx |
NSTEMI / Ischemia
- ST depression ≥ 1 mm in ≥ 2 contiguous leads
- T-wave inversions (symmetric, deep = Wellens syndrome in anterior leads)
- No ST elevation
Pathological Q Waves (old infarction)
- Duration > 0.04 s (1 small box)
- Depth > 25% of the R wave amplitude
- Indicate prior transmural infarction
5. Other Common Patterns
Left Ventricular Hypertrophy (LVH)
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 > 35 mm
- "Strain pattern": ST depression + T-wave inversion in lateral leads (I, aVL, V5–V6)
Right Ventricular Hypertrophy (RVH)
- Right axis deviation (> +90°)
- R/S ratio > 1 in V1
- Dominant R wave in V1
Prolonged QT Interval
- QTc > 440 ms (men), > 460 ms (women)
- Risk of Torsades de Pointes (polymorphic VT)
- Causes: drugs (quinolones, antipsychotics, sotalol), hypokalemia, hypomagnesemia, congenital
Hyperkalemia — ECG Progression
| Potassium Level | ECG Change |
|---|---|
| Mild (5.5–6.5 mEq/L) | Peaked (tent-shaped) T waves |
| Moderate (6.5–7.5) | Wide QRS, flat/absent P waves |
| Severe (> 7.5) | Sine wave pattern → VF → asystole |
Pericarditis
- Diffuse ST elevation (saddle-shaped, concave upward) in virtually all leads
- PR depression (very specific sign)
- No reciprocal changes (distinguishes from STEMI)
Wolff-Parkinson-White (WPW)
- Short PR interval (< 0.12 s)
- Delta wave (slurred upstroke of QRS)
- Wide QRS
- Risk of rapid conduction via accessory pathway in AF
6. Quick Reference Summary
| Pattern | Key ECG Finding | Mnemonic/Memory Aid |
|---|---|---|
| Normal sinus | P before every QRS, rate 60–100 | — |
| Atrial fibrillation | No P waves, irregularly irregular | "Absolutely No Ps" |
| 1° AV block | PR > 200 ms | "Prolonged PR" |
| Mobitz II | Fixed PR + dropped QRS | "Dropped without warning" |
| Complete heart block | P & QRS dissociated | "Nothing gets through" |
| RBBB | rSR' in V1 (M-shape) | "MaRRoW" (M in V1) |
| LBBB | Broad R in V5–V6, rS in V1 | "WiLLiaM" (W in V1) |
| STEMI | ST elevation + reciprocal depression | Territory = culprit artery |
| Hyperkalemia | Peaked T waves → wide QRS | "PAT on the back — P waves disappear" |
| WPW | Delta wave + short PR | "Pre-excited ventricle" |
Sources: Miller's Anesthesia 10e · Medical Physiology (Boron & Boulpaep) · Morgan & Mikhail's Clinical Anesthesiology 7e · Goldman-Cecil Medicine · Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.