I am going to give you question you give answer with easy drawable diagram and clinical 10 marks
I'm ready! Go ahead and share your question. I'll provide a clear answer with an easy-to-draw diagram and clinical points, formatted for a 10-mark answer.
Movement at radioulnar joint
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Now I have excellent textbook content and diagrams. Let me compose the complete 10-mark answer.
Movement at the Radioulnar Joint
Overview
The radioulnar joints are two pivot (trochoid) joints that act together as a single functional unit to produce pronation and supination of the forearm. The ulna remains stationary while the radius rotates around the ulna.
Types of Radioulnar Joints
| Feature | Proximal RUJ | Distal RUJ |
|---|---|---|
| Location | Below elbow | Above wrist |
| Articulation | Head of radius in radial notch of ulna | Head of ulna in sigmoid notch of radius |
| Joint type | Pivot (trochoid) | Pivot (trochoid) |
| Stabilizer | Annular ligament | TFCC (Triangular Fibrocartilage Complex) |
Movement: PRONATION & SUPINATION
Axis of Movement
Runs obliquely from the centre of the radial head (proximal RUJ) to the fovea of the ulnar head / styloid process of ulna (distal RUJ).
Range
- Supination: 0 - 90°
- Pronation: 0 - 90°
- Total rotation: ~180° (with shoulder adding ~270°)
Easy Drawable Diagram
SUPINATION PRONATION
(Palm faces UP) (Palm faces DOWN)
PROXIMAL VIEW: PROXIMAL VIEW:
[Radius] [Ulna] [Radius crosses
parallel over Ulna]
↑ ↑
Annular lig. Annular lig.
holds radius holds radius
in radial notch in radial notch
ANTERIOR VIEW (Right forearm):
SUPINATION PRONATION
R U U
| | / \
| | R |
| | | |
R = Radius, U = Ulna
(parallel) (radius crosses over ulna)
AXIS LINE:
Radial head (above)
|
| (oblique axis)
|
Ulnar styloid (below)
DISTAL RUJ CROSS SECTION:
SUPINATION: NEUTRAL: PRONATION:
[R][U] [R][U] [U][R]
side by side in contact radius crossed
Muscles Producing Movement
SUPINATION (stronger movement)
| Muscle | Nerve | Note |
|---|---|---|
| Biceps brachii | Musculocutaneous (C5, C6) | Most powerful supinator; best when elbow flexed at 90° |
| Supinator | Posterior interosseous nerve (C6) | Works at all positions |
| Brachioradialis | Radial nerve | Returns from mid-position |
Mnemonic: "SUPinator + BICeps = SUPination" - The Biceps also SUPinates
PRONATION (weaker than supination)
| Muscle | Nerve | Note |
|---|---|---|
| Pronator teres | Median nerve (C6, C7) | Main pronator |
| Pronator quadratus | Anterior interosseous nerve (C8) | Works alone in slow pronation |
| Flexor carpi radialis | Median nerve | Weak accessory |
| Brachioradialis | Radial nerve | Returns from full supination |
Mnemonic: "Pronator Teres + Pronator Quadratus = Pronation"
Connecting Structure: Interosseous Membrane
- A fibrous sheet between the shafts of radius and ulna
- Transmits force from radius to ulna (e.g., falls on outstretched hand)
- Fibers run obliquely: downward and medially from radius to ulna
- Functionally links proximal and distal RUJ - movement of one joint is always accompanied by movement of the other
- Central band is thickest = main load transfer
Easy Diagram: Interosseous Membrane
RADIUS (lateral) ULNA (medial)
| \\\\\\\\\\\\\\\\\\ |
| \\\\\\\\\\\\\\\\\ |
| \\\\\\\\\\\\\\\\ | ← Oblique fibers
| \\\\\\\\\\\\\\\ | (radius → ulna,
| \\\\\\\\\\\\\\ | downward + medially)
| |
[Radial [Ulnar
tuberosity] attachment]
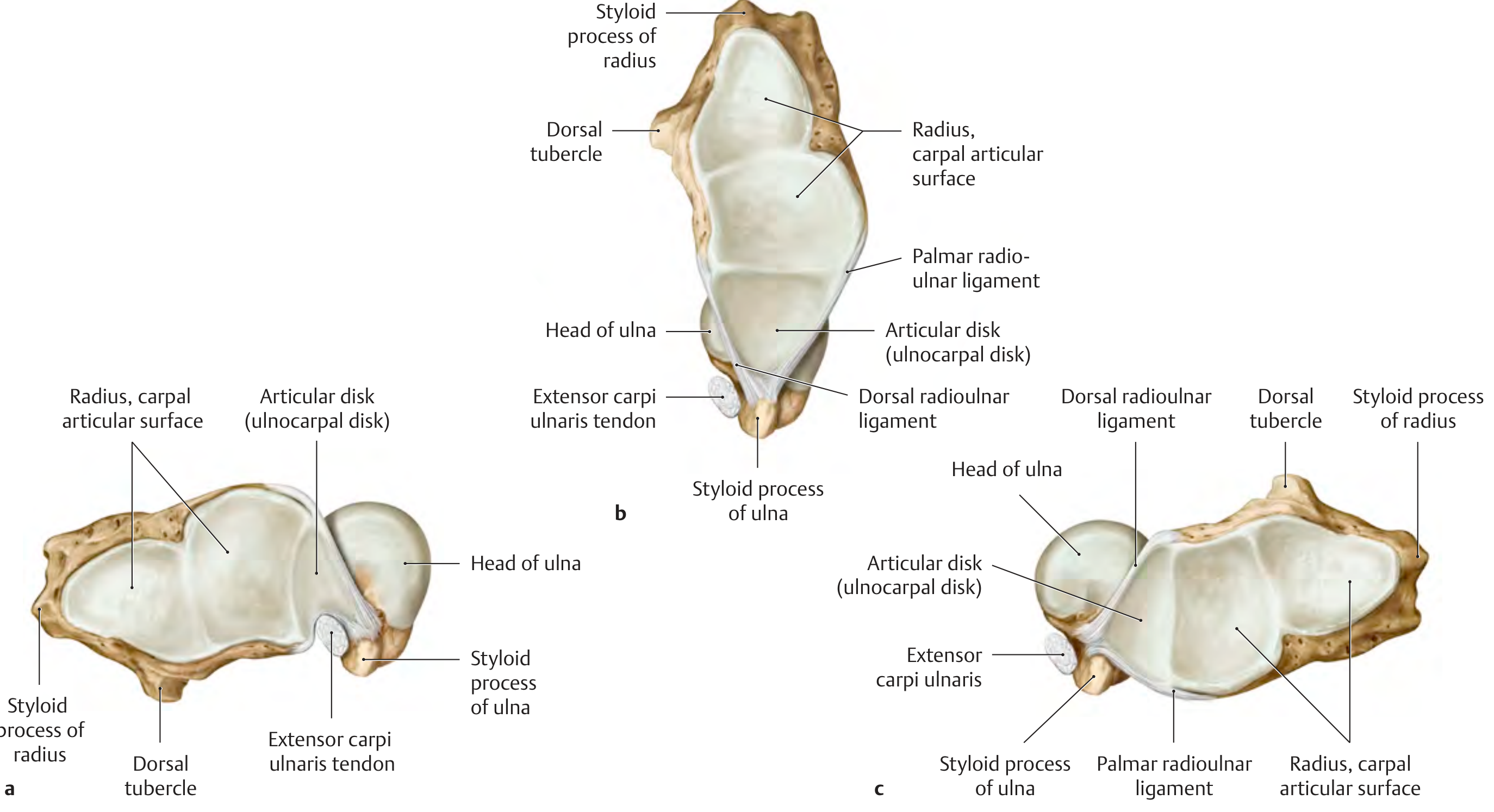
Biomechanics at the Distal RUJ
- In neutral position: styloid process of ulna is aligned with sigmoid notch of radius
- In pronation: ulnar head rotates - styloid process moves to the palmar side; radius migrates proximally (increases ulnar variance)
- In supination: styloid process moves to the dorsal side
- The two distal articular surfaces are in closest contact (congruent) only in neutral/semipronated position
Diagram: Radial head cross-section (Proximal RUJ)
(Based on Thieme Atlas, p. 302)
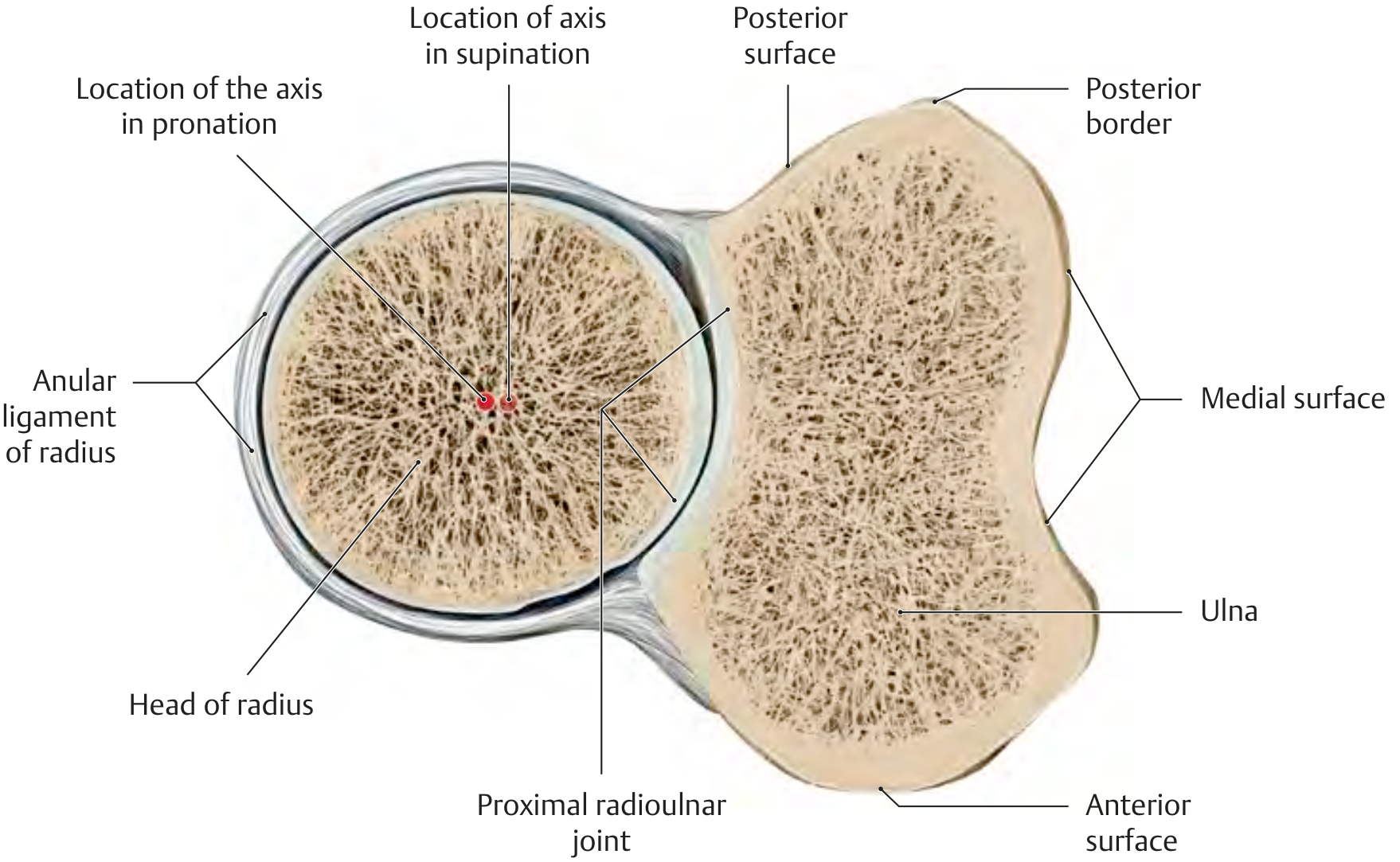
Note: The radial head is slightly oval - the pronation/supination axis shifts ~2 mm radially during pronation. Articular cartilage is thicker on the pronation side (adapts to higher pressure in pronated position).
Diagram: Distal RUJ - Rotation of radius around ulna
Clinical Points (High Yield)
1. Pulled Elbow (Nursemaid's Elbow)
- Common in children < 5 years
- Mechanism: sudden pull on the hand when the forearm is pronated
- Radial head slips out of the annular ligament
- Child holds arm in slight flexion and pronation, refuses to supinate
- Treatment: hyperpronation or supination + flexion manoeuvre - feel/hear a click
2. Monteggia Fracture-Dislocation
- Fracture of the proximal ulna + dislocation of the radial head from the proximal RUJ
- Disrupts the radioulnar joint
- Must always X-ray the elbow when there is a forearm fracture
- Rule: A line through the radial neck/head should always pass through the capitulum in all views
3. Distal Radioulnar Joint (DRUJ) Disruption
- Seen with distal radius fractures (Galeazzi fracture)
- Signs: pain at DRUJ, prominence of ulnar head (piano key sign), restricted and painful pronation/supination
- Stable DRUJ is essential for painless forearm rotation
4. TFCC (Triangular Fibrocartilage Complex) Injury
- Stabilizes the DRUJ
- Injury causes ulnar-sided wrist pain worse on pronation/supination and grip
- Diagnosed by MRI; treatment ranges from physiotherapy to arthroscopic repair
5. Radioulnar Synostosis
- Bony or fibrous union between radius and ulna
- Forearm is fixed in pronation - loss of supination
- Can be congenital or post-traumatic (after severe forearm fractures, especially if both bones fractured at same level)
6. Superior Radioulnar Joint in Rheumatoid Arthritis
- Synovitis leads to destruction of the annular ligament
- Causes instability of the radial head and loss of rotation
Summary Table
| Feature | Detail |
|---|---|
| Type of movement | Pronation and Supination |
| Joint type | Pivot / Trochoid |
| Axis | Radial head to ulnar styloid/fovea |
| Range | ~90° pronation, ~90° supination |
| Strongest supinator | Biceps brachii |
| Strongest pronator | Pronator teres |
| Proximal stabiliser | Annular ligament |
| Distal stabiliser | TFCC + dorsal/palmar RU ligaments |
| Link between joints | Interosseous membrane |
| Moving bone | Radius (rotates around the ulna) |
| Fixed bone | Ulna (relatively stationary) |
Sources: General Anatomy and Musculoskeletal System, Thieme Atlas of Anatomy (p. 270-302); Imaging Anatomy Text and Atlas Vol. 3, Biomechanics of the Arm and Forearm; Rockwood and Green's Fractures in Adults, 10th ed. 2025
This is a shared conversation. Sign in to Orris to start your own chat.