Alcohol withdrawal delirium
Reading File
Finding Sources
Searching PubMed
"alcohol withdrawal delirium" OR "delirium tremens" treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Alcohol Withdrawal Delirium (Delirium Tremens)
Definition
Alcohol withdrawal delirium (AWD), classically called delirium tremens (DTs), is the most severe manifestation of alcohol withdrawal. It is characterized by acute and fluctuating disturbances in consciousness, confusion, psychomotor agitation, inattention, and impaired cognitive and perceptual function (hallucinations) unrelated to preexisting dementia. It develops in 3-5% of patients admitted to hospital for alcohol withdrawal. - Tintinalli's Emergency Medicine, p. 1266; Maudsley Prescribing Guidelines, p. 505
Pathophysiology
Chronic, heavy alcohol use has dual effects on the CNS:
- GABA-A receptor downregulation - alcohol chronically enhances GABAergic tone, so receptors are progressively downregulated
- NMDA receptor (NMDAR) upregulation - alcohol chronically inhibits glutamatergic transmission, causing compensatory upregulation
Upon acute cessation, the CNS enters a hyperexcitable state: reduced GABA-mediated inhibition + excessive NMDA-mediated excitation. This produces the autonomic storm, seizures, and delirium of DTs. Superimposed norepinephrine hyperactivity worsens the syndrome. - Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Time Course
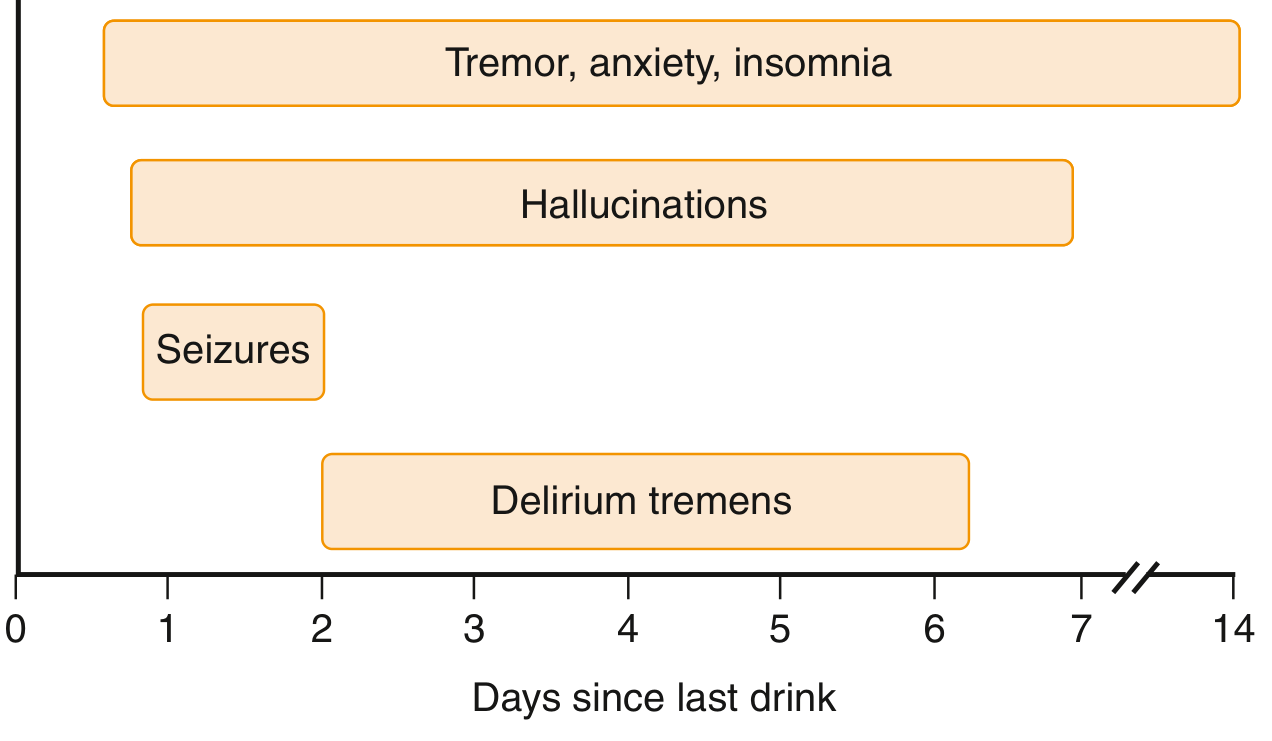
| Symptom | Onset after last drink |
|---|---|
| Tremor, anxiety, insomnia | 3-12 hours; peaks 24-48 h |
| Hallucinations | 24-36 hours |
| Seizures (generalized tonic-clonic) | 12-24 hours; 90% within 48 h |
| Delirium tremens | 72-96 hours (2-4 days) |
Withdrawal phenomena can persist in a milder form for 3-6 months as a protracted withdrawal syndrome. - Goldman-Cecil Medicine, p. 3779; Maudsley Prescribing Guidelines, p. 505
Clinical Features
Core features (DSM-5 requires both delirium + alcohol withdrawal criteria):
- Clouding of consciousness and disorientation
- Vivid hallucinations - visual and tactile predominate (cf. alcoholic hallucinosis where auditory hallucinations predominate)
- Marked tremor
- Psychomotor agitation and paranoid delusions
- Insomnia
Autonomic hyperactivity:
- Tachycardia
- Hypertension
- Diaphoresis
- Fever (hyperthermia)
Life-threatening complications:
- Fluid, metabolic, and electrolyte imbalances (hypovolemia, hypokalemia, hypomagnesemia, hypophosphatemia)
- Aspiration pneumonia
- Death - mortality 10-20% if untreated; reduced to ~1-5% with aggressive treatment. - Tintinalli's Emergency Medicine, p. 1265; Maudsley Prescribing Guidelines, p. 505
Risk Factors for DTs
- Prior history of DTs or complicated withdrawal
- Severe alcohol dependence (high daily intake, prolonged use)
- Prior detoxification history ("kindling effect")
- Older age
- Comorbid medical illness (e.g., hypertension, diabetes)
- Use of other CNS depressants
- About one third of patients with alcohol withdrawal seizures go on to develop DTs. - Tintinalli's Emergency Medicine, p. 1265
Assessment: CIWA-Ar Scale
The Clinical Institute Withdrawal Assessment for Alcohol - Revised (CIWA-Ar) is the standard tool for quantifying withdrawal severity and guiding treatment. It scores 10 parameters:
- Nausea/vomiting, tremor, sweating, anxiety, agitation, tactile disturbances, visual disturbances, auditory disturbances, headache, orientation
- Score >15: benzodiazepine doses every hour until score <15
- Score 8-14: doses every 2 hours until score <8
Limitations: 7 of 10 components require accurate communication with the patient. Language barriers, comorbidities, or sedating medications may impair scoring. - Tintinalli's Emergency Medicine, p. 1266
Treatment
1. Benzodiazepines - First Line
No specific benzodiazepine is superior. Choice depends on clinical context:
For delirium tremens (IV route required):
- Lorazepam 2-4 mg IV; double the dose every 15-20 min until light somnolence
- Diazepam 10-20 mg IV over 2 min; double every 5-10 min until light somnolence
Advantages of each:
- Diazepam/chlordiazepoxide: long-acting active metabolites (20-30 hr duration) - "self-tapering" effect
- Lorazepam/oxazepam: shorter-acting, preferred in liver disease (no active metabolites), elderly patients
- IV diazepam IM is NOT recommended (erratic absorption); IM lorazepam/midazolam is acceptable
Symptom-triggered therapy (guided by CIWA-Ar) uses less drug and shorter treatment than fixed dosing.
2. Refractory DTs
Failure to achieve adequate response with >50-100 mg diazepam or >10-20 mg lorazepam in the first hour indicates refractory DTs:
| Agent | Notes |
|---|---|
| Phenobarbital 65 mg IV every 15-30 min (max 260 mg) | Higher risk of respiratory depression; typically requires intubation |
| Propofol 5 mcg/kg/min IV | Titrate to effect; requires intubation. Risk: propofol infusion syndrome >48 h at >5 mg/kg/hr |
| Dexmedetomidine | Alpha-2 agonist; useful adjunct |
3. Seizures
- Lorazepam 2 mg IV is the recommended treatment
- Phenytoin is NOT recommended - does not prevent alcohol withdrawal seizures and may actually lower the seizure threshold
- Long-acting benzodiazepines (e.g., diazepam) as prophylaxis for those with prior seizure history
- Carbamazepine loading may be used as an alternative when seizures occur despite adequate benzodiazepine loading
4. Supportive Care (ESSENTIAL)
-
Thiamine 100 mg daily (always before glucose to prevent precipitating Wernicke's encephalopathy)
-
Folate 1 mg daily
-
Correct electrolytes: potassium, magnesium (sulfate only if hypomagnesemia confirmed), phosphate
-
Aggressive rehydration for hypovolemia
-
Treat hyperthermia
-
Prevent aspiration
-
Quiet, calm environment with low stimuli
-
Physical restraints temporarily if needed before chemical restraint achieved
-
Tintinalli's Emergency Medicine, p. 1267; Maudsley Prescribing Guidelines
Indications for Inpatient Admission
Inpatient treatment is required if any of the following are present:
- Consumption >30 units/day or SADQ score >30
- History of seizures or prior DTs
- Older adult or minor
- Current benzodiazepine + alcohol use
- Comorbid mental or physical illness
- Pregnancy
- Homelessness or no social support
- Failed community detoxification
ICU admission should be considered for severe withdrawal requiring close respiratory monitoring. - Maudsley Prescribing Guidelines, p. 507
Key Distinctions
| Feature | Alcohol Withdrawal Delirium | Alcoholic Hallucinosis |
|---|---|---|
| Timing | 72-96 h after last drink | Within 12-24 h |
| Hallucinations | Visual + tactile predominate | Auditory predominate |
| Sensorium | Clouded (delirium) | Clear/alert |
| Autonomic features | Prominent | Absent/mild |
| Mortality if untreated | 10-20% | Low |
Recent Evidence Note
A 2025 systematic review (PMID 36958342) examined antipsychotic treatment of alcohol withdrawal syndrome including DTs. Antipsychotics (e.g., haloperidol) may be considered as adjuncts for agitation and hallucinations but are not recommended as monotherapy because they lower the seizure threshold and do not treat the underlying neurochemical instability.
This is a shared conversation. Sign in to Orris to start your own chat.