what can be the causes pf diffuse hair thinning
Reading File
Finding Sources
Searching PubMed
"diffuse hair loss" OR "telogen effluvium" causes
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Now I have excellent material from Fitzpatrick's Dermatology and Goldman-Cecil Medicine. Let me compile the full answer.
Causes of Diffuse Hair Thinning
Diffuse hair thinning (diffuse alopecia) means generalized, non-patchy reduction in hair density across the scalp. The causes span several categories:
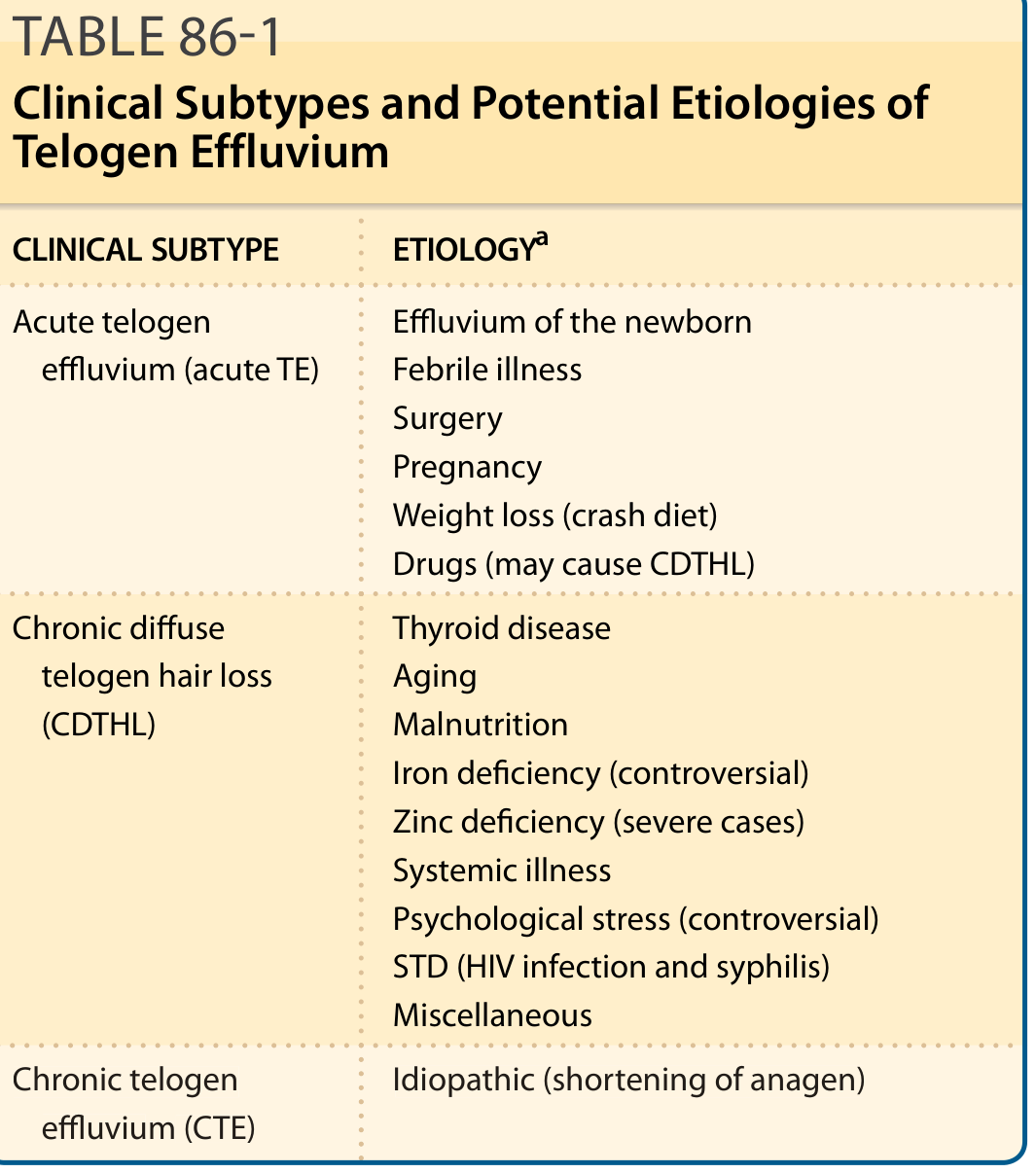
1. Telogen Effluvium (TE) - the most common cause
This is a shift of hair follicles from the growing (anagen) phase into the resting/shedding (telogen) phase. It has two main subtypes:
Acute TE - triggered by a sudden insult 2-3 months prior:
- Febrile illness (high fever, sepsis, influenza)
- Major surgery or general anesthesia
- Pregnancy / postpartum (hair sheds 2-3 months after delivery as estrogen drops)
- Rapid weight loss or crash dieting (calorie restriction <1200 kcal/day, or loss of >10 kg rapidly)
- Drugs (see below)
Chronic diffuse telogen hair loss (CDTHL) - ongoing or lasting >6 months:
- Thyroid disease (both hypo- and hyperthyroidism)
- Malnutrition, protein-calorie deficiency
- Iron deficiency (though the link remains somewhat controversial)
- Zinc deficiency (especially in severe cases / acrodermatitis enteropathica)
- Systemic illness (lupus, inflammatory disease, chronic infections)
- HIV infection and syphilis (STDs)
- Aging (senile effluvium with increased telogen ratio)
- Psychological stress (controversial in the literature)
Chronic Telogen Effluvium (CTE) - idiopathic, due to intrinsic shortening of anagen duration; typically middle-aged women with previously very dense hair.
2. Anagen Effluvium
Sudden, often dramatic shedding during the active growth phase:
- Chemotherapy (especially alkylating agents, taxanes)
- Radiation therapy to the scalp
- Heavy metal poisoning (thallium, arsenic)
- Some immunosuppressants
3. Androgenetic Alopecia (Female Pattern Hair Loss)
In women, this presents as diffuse thinning of the centroparietal scalp (Ludwig/Christmas tree pattern) - unlike the receding hairline seen in men. Caused by:
- Genetic predisposition
- Androgen sensitivity of hair follicles (DHT-mediated miniaturization)
- Hormonal shifts: menopause, polycystic ovary syndrome (PCOS), stopping oral contraceptives
4. Hormonal Causes
| Condition | Mechanism |
|---|---|
| Hypothyroidism | Reduced hair follicle metabolism; most common thyroid cause |
| Hyperthyroidism | Less well established but recognised |
| Menopause | Estrogen withdrawal increases androgen effect |
| PCOS | Elevated androgens |
| Hyperprolactinemia | Can precipitate diffuse shedding |
| Discontinuation of OCP | Sudden drop in estrogen triggers TE |
5. Nutritional / Metabolic
- Iron deficiency (ferritin <30-70 ng/mL is often the threshold studied)
- Zinc deficiency
- Biotin deficiency (rare; more common in patients on prolonged raw egg diet or TPN)
- Vitamin D deficiency
- Protein malnutrition (kwashiorkor, crash diets, bariatric surgery)
- Selenium deficiency or excess
6. Medications (Drug-Induced Alopecia)
Common culprits include:
- Anticoagulants: heparin, warfarin
- Antithyroid drugs: propylthiouracil, carbimazole
- Retinoids: isotretinoin, acitretin
- Antidepressants: SSRIs, lithium, valproate
- Beta-blockers: propranolol, metoprolol
- Hormonal: androgens, anabolic steroids, progesterone-dominant OCP
- Cholesterol-lowering: statins (less common)
- GLP-1 receptor agonists (semaglutide, tirzepatide) - a recently recognized association
7. Systemic Diseases
- Systemic lupus erythematosus (SLE) - can cause diffuse non-scarring thinning
- Inflammatory bowel disease / malabsorption syndromes
- Chronic renal failure
- Liver disease / cirrhosis
- Diabetes mellitus
- HIV/AIDS and secondary infections
- Secondary syphilis (classically "moth-eaten" but can be diffuse)
8. Hair Treatments / Cosmetic Damage
- Excessive bleaching, chemical straightening, perming
- Heat damage reducing hair shaft integrity
- Tight styling (overlaps with traction alopecia)
Key Diagnostic Approach
The workup of diffuse thinning typically includes:
- History: timing (acute vs. chronic), drug history, family history, diet, systemic illness
- Labs: TSH, CBC, ferritin, TIBC, zinc, vitamin D, prolactin, androgens (DHEAS, free testosterone in women), ANA, RPR
- Trichoscopy/dermoscopy: helps distinguish TE (uniform hair calibre) from androgenetic alopecia (>20% variability in hair diameter)
- Scalp biopsy: if diagnosis remains unclear
Recent evidence note: A 2026 systematic review (PMID 41998799) identified GLP-1 receptor agonists (e.g., semaglutide/Ozempic) as a cause of hair loss, likely via rapid weight loss-induced TE. A 2026 review (PMID 41535530) also highlighted sleep deprivation as a contributing factor - an emerging association not yet in older textbooks.
Sources: Goldman-Cecil Medicine, Table 409-1; Fitzpatrick's Dermatology, Table 86-1 and Chapter 86.
normal anti top prolactin and testosterone levels
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
I have solid textbook data. Here is the comprehensive answer:
Normal Prolactin and Testosterone Reference Ranges
Important note: Reference ranges vary between laboratories and assay methods. Always interpret results against your specific lab's reference interval. The values below are widely accepted clinical norms.
Prolactin
Prolactin is secreted in a pulsatile, diurnal pattern - it is highest during sleep and lowest in the morning. Samples should be drawn fasting, early in the morning (ideally 2-3 hours after waking, without prior stress/exercise/breast stimulation), as stress, food, and time of day can all falsely elevate the result.
| Population | Normal Range |
|---|---|
| Men | 2 - 18 ng/mL (40 - 360 mIU/L) |
| Non-pregnant women (normal estrogen) | 2 - 29 ng/mL (up to ~600-800 mIU/L) |
| Women - amenorrheic, hypo-estrogenic, non-pregnant | Upper limit ~20-25 ng/mL (400-500 mIU/L) |
| Pregnant women | 10 - 300 ng/mL (rises progressively) |
| Lactating women | Up to 300 ng/mL or more |
Key thresholds:
-
>25 ng/mL in a non-pregnant woman: investigate for hyperprolactinemia
-
>100 ng/mL: suggests prolactinoma or pituitary adenoma (vs. drug-induced or hypothalamic causes which are usually <100 ng/mL)
-
Prolactin 5-50x above normal: highly suggestive of a prolactin-secreting adenoma (prolactinoma)
-
Tietz Textbook of Laboratory Medicine, 7th Edition
Testosterone
In Men
| Measurement | Normal Range |
|---|---|
| Total testosterone | 300 - 1000 ng/dL (10.4 - 34.7 nmol/L) |
| Free testosterone | 9 - 30 ng/dL |
| Hypogonadism threshold (AACE) | <200 ng/dL (but interpretation is clinical, not purely numerical) |
Practical notes:
-
Sample should be drawn in the early morning (8-10 AM) when levels peak (diurnal variation - levels drop 20-30% by afternoon)
-
A single low value is not diagnostic - always repeat to confirm
-
Hypogonadism is a clinical + biochemical diagnosis; a "low" number alone without symptoms is not sufficient for treatment
-
Free testosterone is more useful when SHBG is abnormal (e.g., obesity, liver disease, thyroid disease)
-
Textbook of Family Medicine, 9th Edition
In Women
| Measurement | Normal Range |
|---|---|
| Total testosterone | 15 - 70 ng/dL (0.5 - 2.4 nmol/L) |
| Free testosterone | 0.3 - 1.9 ng/dL |
- Women's testosterone is 10-20x lower than men's
- Elevated levels suggest PCOS, congenital adrenal hyperplasia (CAH), adrenal or ovarian tumor, or exogenous androgen use
- Levels vary slightly across the menstrual cycle
Quick Reference Summary
| Hormone | Men | Women (non-pregnant) |
|---|---|---|
| Prolactin | 2-18 ng/mL | 2-29 ng/mL |
| Total testosterone | 300-1000 ng/dL | 15-70 ng/dL |
| Free testosterone | 9-30 ng/dL | 0.3-1.9 ng/dL |
When to suspect abnormality:
- Prolactin high + hair loss + irregular periods + galactorrhea → hyperprolactinemia workup (MRI pituitary)
- Testosterone low (men) + fatigue + low libido + reduced muscle mass → hypogonadism workup
- Testosterone high (women) + hair loss + acne + irregular periods → androgen excess workup (PCOS, CAH)
a patient with normal anti tpo notmal testosterone and prolactin level having diffuse hairfall .. what could be the reason
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Excellent - I now have all the data needed for a thorough, clinically focused answer.
Diffuse Hair Loss with Normal Anti-TPO, Testosterone & Prolactin
So autoimmune thyroiditis, androgen excess, and prolactinoma have been effectively excluded. The differential now narrows to the following categories - listed in order of clinical likelihood:
1. TSH May Still Be Abnormal (Check TSH Directly)
Anti-TPO tells you about autoimmune activity, but not thyroid function. A patient can have:
- Subclinical hypothyroidism (elevated TSH, normal T4) with no anti-TPO elevation
- Non-autoimmune hypothyroidism (iodine deficiency, post-surgical, central/secondary hypothyroidism)
- Hyperthyroidism (low TSH) - often missed, also causes diffuse shedding
Anti-TPO being normal does not exclude thyroid dysfunction. TSH + free T4 must be checked independently.
2. Iron Deficiency / Low Ferritin (Most Common Identifiable Cause)
Iron deficiency is one of the most frequently found and treatable causes of diffuse hair loss, especially in women.
- Hair loss is typically a diffuse nonscarring alopecia
- Reported with ferritin <100 ng/mL (even without frank anemia)
- Ferritin <15 ng/mL: diagnostic of iron deficiency; ferritin <50 ng/mL should be considered abnormal in a symptomatic patient
- Iron may serve as a broader marker of nutritional status rather than being the direct causal factor alone
Check: Serum ferritin, serum iron, TIBC, iron saturation - Goldman-Cecil Medicine
Key clinical point: A patient can have normal hemoglobin and CBC but still have depleted iron stores causing hair loss. Always check ferritin specifically.
3. Telogen Effluvium (TE) from a Trigger 2-4 Months Prior
This is the single most common cause of acute diffuse shedding and may have no detectable lab abnormality. Look back at the history for:
| Trigger | Timing Before Shedding |
|---|---|
| Febrile illness / infection / COVID-19 | 6-12 weeks prior |
| Major surgery or hospitalization | 6-12 weeks prior |
| Postpartum (delivery) | 8-12 weeks prior |
| Rapid weight loss / crash diet | 6-12 weeks prior |
| Psychological/physical stress | 6-12 weeks prior |
| Stopping oral contraceptives | 6-12 weeks prior |
Lab results are typically all normal in acute TE - the diagnosis is clinical. - Andrews' Diseases of the Skin
4. Chronic Telogen Effluvium (CTE) - Idiopathic
- Affects middle-aged women (30-60 years), often with a history of previously very thick, long hair
- Diffuse shedding + bitemporal recession, fluctuating course
- All labs (including thyroid, iron, hormones) may be entirely normal
- Mechanism: intrinsic shortening of the anagen (growth) phase
- Diagnosis of exclusion; may respond to 5% minoxidil - Fitzpatrick's Dermatology
5. Nutritional Deficiencies (Beyond Iron)
Even with normal hormones, nutritional gaps can drive diffuse thinning:
| Nutrient | Notes |
|---|---|
| Zinc | Deficiency causes diffuse telogen hair loss; severe cases can mimic acrodermatitis enteropathica |
| Vitamin D | VDR (vitamin D receptor) plays a role in hair follicle cycling; low levels associated with TE |
| Biotin | Rare - mainly in patients on long-term TPN, raw egg diet, or with biotinidase deficiency |
| Protein/calorie | Crash diets, bariatric surgery, eating disorders |
| Selenium | Both deficiency and excess can cause hair loss |
Check: Zinc, vitamin D (25-OH), B12, folate in relevant patients.
6. Androgenetic Alopecia (AGA) in Women - Diffuse Form
Normal total testosterone does not exclude AGA in women because:
- AGA can occur with normal circulating androgens due to increased follicular sensitivity to DHT (5-alpha reductase activity)
- Female pattern AGA presents as diffuse centroparietal thinning (Ludwig pattern) or Christmas-tree pattern - maintained frontal hairline distinguishes it from male AGA
- Family history is often positive
- Dermoscopy shows >20% variability in hair shaft diameter (miniaturization)
Check free testosterone and DHEAS if not done - total testosterone alone can be normal even with androgen-driven AGA. - Fitzpatrick's Dermatology
7. Drug-Induced Alopecia
A full medication review is essential. Common culprits causing diffuse/telogen hair loss:
- Beta-blockers (propranolol, metoprolol)
- Anticoagulants (heparin, warfarin)
- Antidepressants (SSRIs, lithium, valproate)
- Retinoids (isotretinoin, acitretin)
- Antithyroid drugs
- GLP-1 agonists (semaglutide/Ozempic - likely via rapid weight loss-induced TE)
- Captopril, enalapril, cimetidine, carbamazepine, levodopa - Andrews' Diseases of the Skin
8. Other Systemic Conditions to Exclude
| Condition | Test |
|---|---|
| Systemic lupus erythematosus | ANA, anti-dsDNA |
| Secondary syphilis | RPR/VDRL, TPHA |
| HIV infection | HIV screen |
| Celiac disease / malabsorption | Anti-tTG IgA, IgA level |
| Chronic renal or liver disease | Renal + liver function tests |
| Diabetes mellitus | Fasting glucose, HbA1c |
Recommended Workup Summary for This Patient
| Test | Purpose |
|---|---|
| TSH + Free T4 | Exclude thyroid dysfunction (anti-TPO alone is not enough) |
| Serum ferritin | Most important nutritional test; target >70 ng/mL for hair |
| CBC | Rule out anemia |
| Zinc, vitamin D (25-OH) | Nutritional causes |
| Free testosterone + DHEAS | Even with normal total testosterone |
| ANA | Screen for lupus |
| RPR | Exclude secondary syphilis |
| Detailed drug/medication history | Drug-induced TE |
| Trichoscopy/dermoscopy | Distinguish AGA (variable shaft diameter) from TE (uniform) |
| Scalp biopsy | If diagnosis still unclear after above |
The single most important extra step: check TSH and ferritin - these are the two most common, treatable, and easily missed causes when anti-TPO/testosterone/prolactin are all normal.
chronic telegium efflovum treatment
Finding Sources
Searching PubMed
"chronic telogen effluvium" treatment
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive textbook content. Here is the full treatment answer:
Treatment of Chronic Telogen Effluvium (CTE)
First - Understand What You're Treating
CTE is defined as idiopathic diffuse hair shedding lasting >6 months with no identifiable cause, caused by intrinsic shortening of the anagen phase. It must be distinguished from Chronic Diffuse Telogen Hair Loss (CDTHL), which looks the same but has an identifiable cause (thyroid disease, iron deficiency, drugs, etc.). Treatment differs:
- CDTHL: treat and eliminate the underlying cause - hair recovers
- True idiopathic CTE: cause unknown, so management is different
The most important first step is always a thorough exclusion of all secondary causes (see previous responses).
Step 1 - Correct Any Identifiable Underlying Cause (CDTHL)
Before anything else, address reversible contributors:
| Cause | Treatment |
|---|---|
| Iron deficiency (low ferritin) | Oral ferrous sulfate 200 mg once-twice daily; target ferritin >70 ng/mL |
| Zinc deficiency | Zinc supplementation (zinc sulfate or gluconate) |
| Vitamin D deficiency | Cholecalciferol supplementation |
| Hypothyroidism | Levothyroxine (TSH must be checked - anti-TPO alone is not enough) |
| Drug-induced | Identify and stop the causative drug; recovery expected ~3 months after stopping |
| Protein/calorie deficiency | Dietary correction, high-protein diet |
| Nutritional deficiency overall | Balanced diet, correct identified deficiencies |
Iron replacement alone may not resolve the hair loss but improves overall nutritional status - Andrews' Diseases of the Skin
Step 2 - Core Management of Idiopathic CTE
A. Reassurance + Psychological Support (First-Line)
This is the cornerstone of CTE management per Fitzpatrick's Dermatology:
-
Explain the hair cycle and the mechanism of TE to the patient
-
Reassure that CTE does not lead to total baldness - long-term follow-up shows no visible reduction in hair density even after 7-8 years of continuous fluctuating loss
-
Counsel that spontaneous resolution is the expected outcome
-
For patients needing objective proof of recovery: periodical collection and counting of shed hairs under standardized conditions (e.g., after daily shampooing) - the patient can visually track improvement
-
Address any underlying anxiety or depression, which may co-exist and worsen perceived symptoms (trichodynia is common in CTE and is often linked to anxiety)
-
Fitzpatrick's Dermatology
B. Topical Minoxidil 5% (First Pharmacologic Option)
-
Minoxidil 5% solution or foam applied to scalp once or twice daily
-
Mechanism: prolongs anagen phase, increases follicle size, increases hair shaft diameter
-
Effective in CTE - may respond to 5% formulation
-
Important warning to give patients: shedding typically increases for the first 2-6 weeks after starting minoxidil (immediate telogen release mechanism) - patients must be warned or they will stop the drug thinking it is worsening things
-
Results visible at 3-6 months; assess at 12 months for full effect
-
Side effects: scalp irritation or contact dermatitis (more with liquid due to propylene glycol; use foam if this occurs)
-
Fitzpatrick's Dermatology, Cummings Otolaryngology
C. Low-Dose Oral Minoxidil (Emerging / Off-Label)
-
Used when topical minoxidil is insufficient or not tolerated
-
Dose: 0.25 mg to 2.5 mg daily (women); lower doses used to minimize cardiovascular side effects
-
A retrospective study of 36 women with CTE treated with oral minoxidil showed improvement in all patients at 6 or 12 months
-
More rapid and extensive hair growth than topical in some patients
-
Not FDA-approved for hair loss - prescribed off-label
-
Must discuss cardiovascular risks before prescribing (fluid retention, pericardial effusion, reflex tachycardia)
-
Common side effect: hypertrichosis (facial hair growth)
-
Cummings Otolaryngology Head and Neck Surgery
Step 3 - Additional / Adjunctive Options
| Treatment | Evidence / Role |
|---|---|
| Nutritional supplements (biotin, iron, zinc, vitamin D) | Correct deficiencies; limited evidence for supplementation without deficiency |
| Spironolactone (25-100 mg/day, women only) | Anti-androgen effect; used in combination with oral minoxidil; helpful if any androgen contribution |
| Low-level laser therapy (LLLT) | FDA-cleared device; stimulates follicle metabolism; modest evidence, safe option |
| Platelet-rich plasma (PRP) | Injected into scalp; growth factors may stimulate follicles; evidence growing (included in 2024 systematic review PMID 38886861) |
| Melatonin topical | Some evidence for promoting anagen; available as topical solution |
| Ketoconazole 2% shampoo | Anti-inflammatory; adjunctive role |
Step 4 - Manage Comorbid Scalp Disease
- Treat seborrheic dermatitis or scalp psoriasis if present (listed as TE triggers)
- Anti-inflammatory scalp conditions can worsen TE
Prognosis
-
CTE has a favorable long-term prognosis - visible baldness does not occur
-
Shedding fluctuates but does not progress to complete hair loss
-
Hair density remains normal or near-normal long-term even without specific treatment
-
Spontaneous resolution occurs in many patients over months to years
-
The condition is distressing but not disfiguring - this message is important to convey clearly
-
Fitzpatrick's Dermatology (Whiting DA, long-term follow-up)
Summary Flowchart
CTE suspected (>6 months diffuse shedding)
↓
Thorough investigation to exclude CDTHL causes
↓
Cause found? → Treat it (iron, thyroid, drugs, nutrition)
↓
No cause found (true idiopathic CTE)?
↓
1. Reassurance + counseling (mandatory)
2. Topical minoxidil 5% (first-line drug)
3. Address nutritional deficiencies
4. Low-dose oral minoxidil if inadequate response (off-label)
5. Consider PRP, LLLT as adjuncts
6. Monitor and follow up every 3-6 months
shampoo for tenoflavum
Finding Sources
Searching the Web
best shampoo for telogen effluvium ketoconazole evidence 2024
Finding Sources
Searching PubMed
"ketoconazole shampoo" hair loss alopecia
Here is a clear, practical answer:
Shampoos for Telogen Effluvium
Important context first: No shampoo directly treats or reverses telogen effluvium, because TE is driven by internal factors (nutritional, hormonal, stress-related). Shampoos work at the scalp surface and cannot change the anagen/telogen ratio. Their role is supportive - reducing scalp inflammation, improving the follicular environment, and managing co-existing scalp conditions that can worsen shedding.
1. Ketoconazole 2% Shampoo - Best Evidence (Adjunctive)
Examples: Nizoral 2% (prescription), Nizoral 1% (OTC)
- Most studied shampoo in the context of hair loss
- Primary action: antifungal targeting Malassezia (scalp yeast), reduces scalp inflammation
- Secondary effects: may weakly inhibit androgen activity at the scalp level (5-alpha reductase inhibition locally)
- Studies show 18% increase in hair density and 7% increase in shaft diameter over 6 months in alopecia patients
- Reduces scalp inflammation that can co-exist with and worsen TE
- How to use: 2-3 times per week, leave on scalp for 3-5 minutes before rinsing
- Can be drying with frequent use - follow with conditioner on lengths (not scalp)
2. Zinc Pyrithione Shampoo
Examples: Head & Shoulders, Selsun Blue (some formulations)
- Anti-dandruff, antifungal, anti-inflammatory
- Reduces Malassezia overgrowth and scalp inflammation
- Some evidence of modest hair count improvement in AGA; useful adjunct in TE
- Gentler than ketoconazole, suitable for daily use
- Good choice if scalp is dry/sensitive
3. Caffeine Shampoo
Examples: Alpecin Caffeine Shampoo, various brands
- Caffeine penetrates the scalp and has been shown to stimulate hair follicle metabolism and prolong anagen duration in lab studies
- A study showed significant reduction in hair loss over 3 months compared to placebo
- Mechanism: inhibits phosphodiesterase, increases cAMP in follicular cells - similar pathway to minoxidil
- Important: must be left on scalp for at least 2 minutes before rinsing to allow absorption
- Particularly relevant to TE as it targets the anagen/telogen balance
4. Biotin + Keratin Fortifying Shampoos
- Strengthen the hair shaft and reduce breakage
- Do NOT treat the underlying shedding but improve appearance and reduce mechanical hair loss
- Examples: OGX Biotin & Collagen, Viviscal Gorgeous Growth
- Useful while waiting for pharmacologic treatments to take effect (3-6 months)
5. Gentle/Sulfate-Free Shampoo (General Recommendation)
- During active TE, the scalp is already shedding more; harsh sulfate-based shampoos can accelerate mechanical loss
- Use a gentle, sulfate-free shampoo for regular washing
- Wash every 2-3 days (not daily unless very oily - daily washing doesn't cause TE, but excessive manipulation does)
- Examples: Vanicream Free & Clear, CeraVe Hydrating Cleanser (scalp), Dove Dermacare
What to Avoid
| Avoid | Reason |
|---|---|
| Harsh sulfate shampoos (SLS) | Strip scalp, worsen dryness and inflammation |
| Very hot water when washing | Increases shedding during shower |
| Vigorous towel rubbing | Mechanical breakage of fragile telogen hairs |
| Shampoos with heavy silicones + sulfates | Buildup + stripping cycle damages shaft |
Practical Shampoo Routine for TE
| Day | Shampoo |
|---|---|
| Mon/Wed/Fri | Ketoconazole 2% (leave 3-5 min) |
| Other days | Gentle sulfate-free or caffeine shampoo |
Bottom Line
| Shampoo | Role | Evidence |
|---|---|---|
| Ketoconazole 2% | Anti-inflammatory, anti-androgen locally | Best evidence |
| Zinc pyrithione | Scalp health, anti-inflammatory | Good |
| Caffeine | Follicle stimulation, prolongs anagen | Moderate |
| Gentle/sulfate-free | Reduce mechanical loss | Supportive |
| Biotin/keratin | Shaft strengthening only | Cosmetic |
Shampoos are adjuncts to - not replacements for - the primary management of TE: treating the underlying cause, nutritional correction, and topical/oral minoxidil where indicated.
best 2 percent ketoconazole shampoo
Searching the Web
best 2% ketoconazole shampoo brands available 2025 hair loss
Here is a practical breakdown:
Best 2% Ketoconazole Shampoos
Availability Note
2% ketoconazole requires a prescription in the US, UK, and many countries. The 1% version (e.g., Nizoral A-D in the US) is available OTC. In many South Asian countries (India, Pakistan, Bangladesh), 2% is available over the counter as a branded or generic product.
Top 2% Ketoconazole Shampoo Brands
| Brand | Notes |
|---|---|
| Nizoral 2% (Janssen/J&J) | The original gold standard; most studied in clinical trials; widely used globally |
| Ketomac Shampoo | Popular in India/South Asia; 2% ketoconazole; widely available OTC; affordable |
| Fungitar 2% Shampoo | Generic; commonly available in South Asia |
| Scalpe+ 2% Shampoo | India; contains 2% ketoconazole + ZPTO (zinc pyrithione); dual action |
| Selsun Gold (some formulations) | Contains ketoconazole in some regional versions |
| Ketoconazole generic shampoo | Multiple manufacturers; identical active ingredient to Nizoral at lower cost |
Which to Choose
For hair loss / telogen effluvium specifically:
- Nizoral 2% if available - most evidence, well-formulated
- Ketomac or Scalpe+ are excellent, cost-effective alternatives in South Asia with equivalent active ingredient concentration
The active ingredient is what matters - all 2% ketoconazole shampoos have the same therapeutic effect regardless of brand. Generics work just as well.
How to Use (Correct Technique)
- Wet scalp thoroughly
- Apply shampoo directly to scalp (not hair lengths)
- Leave on for 3-5 minutes - this contact time is essential for effect; rinsing immediately defeats the purpose
- Rinse thoroughly
- Use 2-3 times per week (not daily - can cause dryness)
- Follow with a gentle conditioner on the lengths (avoid scalp)
Important Points
- Expect no dramatic hair regrowth from ketoconazole shampoo alone - it is an adjunct, not a standalone cure
- Works best when combined with topical minoxidil (the two have complementary mechanisms)
- Avoid using on chemically colored/bleached hair frequently - can slightly affect color
- If scalp becomes dry or irritated, reduce to once a week and increase moisturizing conditioner
This is a shared conversation. Sign in to Orris to start your own chat.