Sinusitis management
Reading File
Finding Sources
Searching PubMed
"sinusitis" AND "management"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, well-sourced content to give a thorough answer. Here is the full synthesis:
Sinusitis Management
Classification
Sinusitis (more accurately, rhinosinusitis) is classified by duration:
| Type | Duration |
|---|---|
| Acute | Up to 3 weeks (some sources: <4 weeks) |
| Subacute | 3-6 weeks |
| Chronic | >12 weeks |
| Recurrent acute | ≥4 episodes/year without intervening symptoms |
The most commonly involved sinuses are the maxillary and anterior ethmoid; frontal and sphenoid involvement occurs later. The underlying mechanism is obstruction at the ostiomeatal unit, leading to mucus stasis and secondary bacterial infection.
Common Pathogens
| Type | Organisms |
|---|---|
| Acute bacterial | S. pneumoniae (30%), H. influenzae (20%), M. catarrhalis (20%) |
| Chronic | S. aureus, gram-negatives, anaerobes, Pseudomonas spp. |
| Fungal (invasive) | Aspergillus, Mucorales (Rhizopus, Mucor) - immunocompromised |
| Allergic fungal | Aspergillus, other fungi - atopic, immunocompetent |
Acute Sinusitis
Step 1 - Distinguish Viral from Bacterial
About 2% of viral URIs progress to bacterial rhinosinusitis. Antibiotics are indicated only when symptoms meet one or more of the following criteria (IDSA / Harrison's Table 37-2):
| Indication | Definition |
|---|---|
| Persistent | Symptoms lasting ≥10 days without improvement |
| Severe | Fever >102°F + purulent discharge or facial pain for ≥3-4 consecutive days |
| Worsening ("double sickening") | New fever, headache, or increased discharge after initial 5-6 days of improvement |
Roughly 20-50% of adults with sinusitis meet antibiotic criteria; 8 out of 10 patients improve without antibiotics (Cochrane Collaboration data).
Step 2 - Symptomatic Treatment (all patients)
- Intranasal decongestants: oxymetazoline 2 sprays each nostril BID - no more than 5 days
- Oral decongestants: pseudoephedrine 120 mg (12-h formulation) during the day
- Analgesics/antipyretics: acetaminophen or ibuprofen
- Nasal saline: sprays or higher-volume nasal washes - provide relief and improve drainage
- Intranasal glucocorticoids: especially helpful when there is an allergic component
Step 3 - Antibiotic Selection
Management algorithm (IDSA guideline):
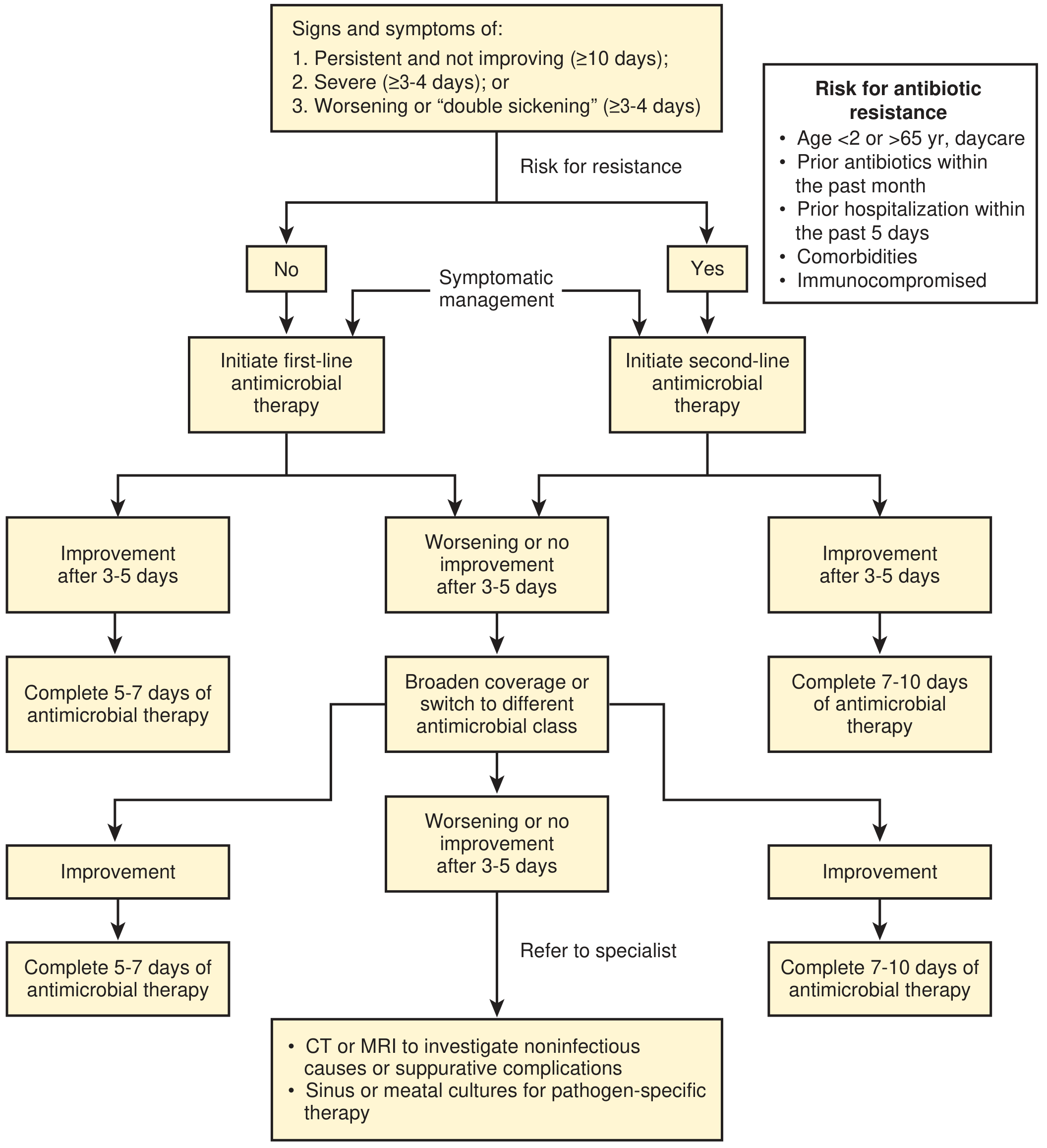
First-line (no resistance risk factors):
- Amoxicillin-clavulanate 875/125 mg PO BID x 7 days (preferred)
- Amoxicillin 875 mg PO BID x 7 days (alternative, if no resistance risk)
- Course: complete 5-7 days if improving after 3-5 days
Penicillin allergy:
- Mild allergy: cefuroxime
- Severe allergy: doxycycline
- Macrolides are specifically NOT recommended due to high rates of macrolide-resistant S. pneumoniae
Risk factors for antibiotic resistance (use second-line therapy):
- Age <2 or >65 years, daycare attendance
- Prior antibiotics within the past month
- Prior hospitalization within 5 days
- Significant comorbidities
- Immunocompromised state
Second-line (resistance risk or treatment failure at 3-5 days):
- Amoxicillin-clavulanate 2000/125 mg PO BID x 7 days
- Levofloxacin (fluoroquinolones - note risks: dysglycemia, neuropathy, tendon/aortic rupture)
- Complete 7-10 days if improving after 3-5 days
No improvement after second-line antibiotics: Refer to otorhinolaryngologist; obtain non-contrast CT (modality of choice); culture sinus/meatal aspirate.
Red Flags - When to Seek Urgent Care
Complications are rare but include orbital cellulitis, osteomyelitis, meningitis, intracranial abscesses, cavernous sinus thrombosis. Prompt reassessment is needed for:
- Confusion, unilateral weakness
- Proptosis, limited ocular movements, acute vision changes
- Recurrent fever >102°F after initial improvement
- Rapidly worsening, persistent facial pain
Chronic Sinusitis (>12 weeks)
Three Main Types
- Without polyps - more common in women; T-helper 1 predominance; bacterial etiology; facial pain prominent
- With polyps - more common in men; T-helper 2 / eosinophilic inflammation; associated with asthma and aspirin sensitivity (Samter's triad); hyposmia/anosmia prominent
- Allergic fungal rhinosinusitis - atopic patients in warm/humid regions; IgE-mediated + eosinophils; classically greenish-brown "peanut butter" mucus with viable fungal hyphae
Diagnosis
- Confirm with anterior rhinoscopy, nasal endoscopy, or imaging - up to 40% of patients with chronic sinus symptoms have no mucosal changes on exam
- Non-contrast CT is the imaging modality of choice - required before treatment to confirm diagnosis and identify polyps, septal deviation, allergic fungal sinusitis, or tumors
Medical Treatment
| Intervention | Notes |
|---|---|
| Trigger avoidance | Allergens, smoke, irritants |
| Nasal saline washes | Effective and well-tolerated; higher-volume washes more effective |
| Intranasal glucocorticoids | Mometasone, fluticasone, budesonide - reduce polyp size; mainstay especially for CRS with polyps |
| Oral glucocorticoids | 2-3 weeks - for CRS unresponsive to topical steroids, especially with polyps; short-lived benefit |
| Antihistamines (intranasal/oral) | If allergic component; note antihistamines can cause mucosal drying and mucus stasis |
| Leukotriene antagonists | Montelukast - useful adjunct for allergic component |
| Antibiotics | Frequently prescribed 2-4 weeks but little evidence of efficacy; 3 months of macrolides (modest evidence) for CRS without polyps |
| Antifungal agents | No demonstrated benefit for any subtype of CRS |
| Biologics | Dupilumab (anti-IL-4/IL-13) - approved for CRS with polyps; recent meta-analysis (PMID 39149992) shows comparable outcomes to sinus surgery in CRS with polyps |
Surgical Treatment - Functional Endoscopic Sinus Surgery (FESS)
Indicated when medical therapy has been inadequate. Goals:
- Remove polyps from nasal cavity and paranasal sinuses
- Improve sinus drainage by restoring ostiomeatal unit patency
- Patients with more focal, limited disease have more reliable results
- For allergic fungal rhinosinusitis: surgery produces good results; medical therapy is classically ineffective; post-operative systemic glucocorticoids help prevent recurrence
Special Populations
Immunocompromised Patients (HIV, Transplant Recipients, Hematologic Malignancy)
- CD4 ≥200 cells/µL: treat with standard regimens
- CD4 <200 or ANC <600: broaden antibiotic coverage to include Staphylococcus, Pseudomonas, and anaerobes
- Invasive fungal sinusitis (IFS): treat with IV antifungals + urgent surgical debridement; evaluate with gadolinium-enhanced MRI; this is a medical/surgical emergency
Nosocomial Sinusitis
- Suspect in hospitalized patients with fever without identifiable cause, especially nasotracheal intubation
- Remove precipitating factors (remove nasal tube if possible)
- Empiric broad-spectrum antibiotics; tailor to culture and susceptibility results
Pediatric Sinusitis
- Diagnosis: persistent (>10 days) or severe URI symptoms, or double sickening
- Most common pathogens same as adults
- Imaging not recommended routinely - sinus mucosal changes present in 97% of infants within 2 weeks of URI
- Antibiotic of choice: amoxicillin-clavulanate (high-dose for resistant organisms)
- Efficacy of antibiotics for pediatric CRS has not been validated; evidence-based treatment differs from adults (a 2025 Italian intersociety consensus - PMID 40140854 - provides updated pediatric guidance)
Recurrent Acute Sinusitis (≥4 episodes/year)
- Nasal culture during episodes
- Imaging between episodes to identify predisposing anatomic abnormalities (deviated septum, polyps)
- Allergic and immunologic evaluation
- Consider ENT referral for FESS if structural abnormality identified
Summary Algorithm
Acute URI symptoms
|
v
Are criteria met? (Persistent ≥10d, Severe, or Worsening)
|
NO --> Symptomatic only (decongestants, analgesics, saline, intranasal steroid)
|
YES --> Risk factors for resistance?
|
NO --> Amoxicillin-clavulanate 875/125 mg BID x 7d
YES --> Amoxicillin-clavulanate 2000/125 mg BID x 7d or levofloxacin
|
Reassess at 3-5 days
|
Improving --> Complete course
Not improving --> Escalate / refer / CT scan
Key references:
- Harrison's Principles of Internal Medicine 22E, pp. 298-300
- Textbook of Family Medicine 9e, pp. 421-426
- Tintinalli's Emergency Medicine, Ch. 123
- Cummings Otolaryngology Head and Neck Surgery
- IDSA Clinical Practice Guideline for ABRS (Chow et al., Clin Infect Dis 2012)
- Recent: Dupilumab vs. sinus surgery for CRS with polyps - systematic review/meta-analysis (Kim et al., Am J Rhinol Allergy 2024, PMID 39149992) - dupilumab shows comparable efficacy to surgery
This is a shared conversation. Sign in to Orris to start your own chat.