Arrythmias
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a complete, exam-focused guide to Antiarrhythmic Drugs compiled from Lippincott Pharmacology, Katzung, and Goodman & Gilman.
Antiarrhythmic Drugs - Complete Study Guide
The Cardiac Action Potential (Foundation)
Before drugs make sense, you need to know what phase they target:
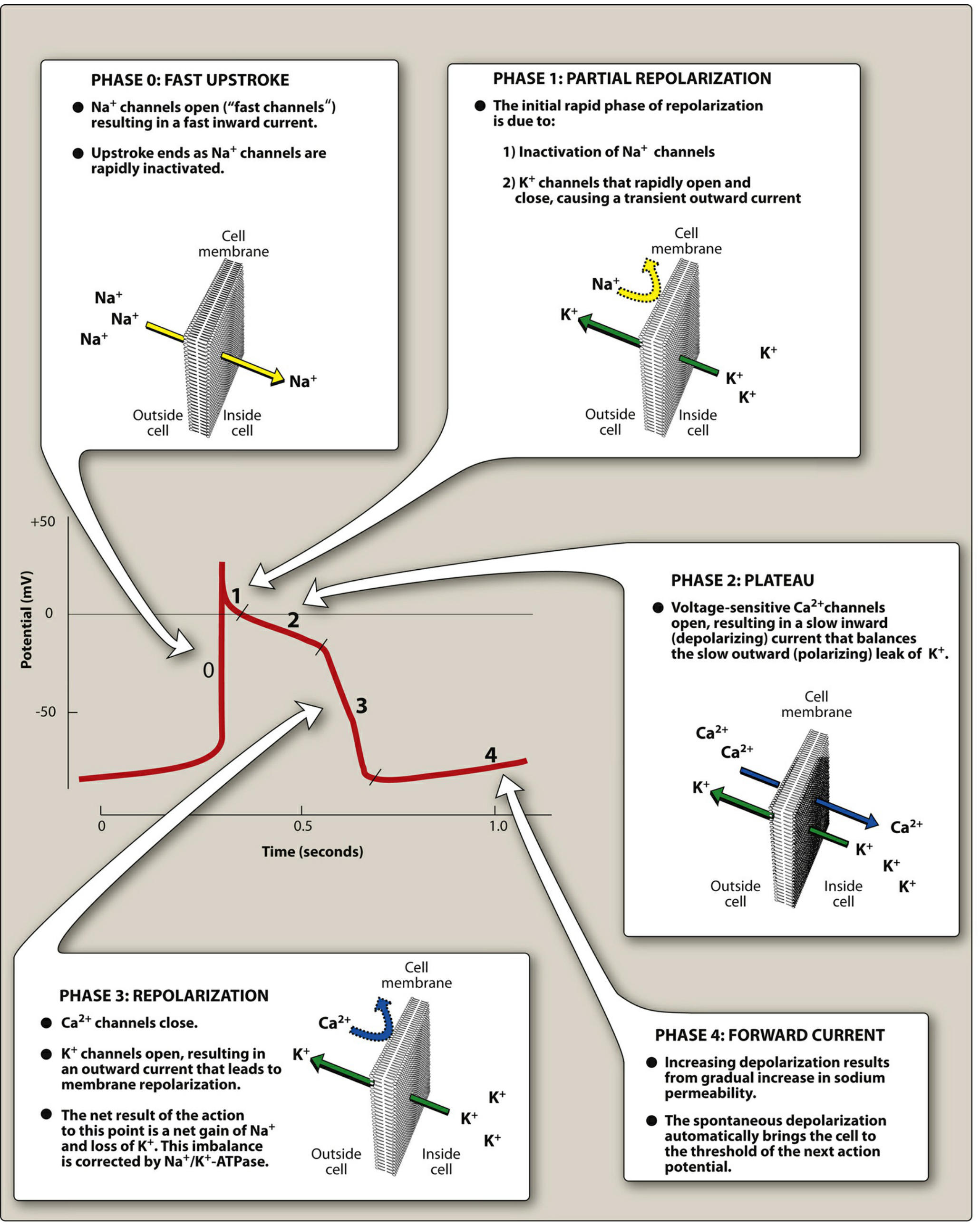
| Phase | What happens | Key ions |
|---|---|---|
| 0 | Fast depolarization (upstroke) | Na⁺ rushes in (fast channels open) |
| 1 | Partial repolarization | Na⁺ channels inactivate; transient K⁺ out |
| 2 | Plateau | Ca²⁺ in balances slow K⁺ out |
| 3 | Repolarization | Ca²⁺ channels close; K⁺ channels open |
| 4 | Pacemaker slow depolarization | Gradual Na⁺ permeability rise |
Vaughan-Williams Classification
Class I - Sodium Channel Blockers
All Class I drugs block Na⁺ channels, reducing the rate of rise of Phase 0. The subclasses differ by kinetics of channel dissociation and effect on action potential duration (APD).
Class IA - Intermediate dissociation, PROLONGS APD & QT
Drugs: Quinidine, Procainamide, Disopyramide (mnemonic: Queen Proclaims Dignity)
| Feature | Details |
|---|---|
| Mechanism | Na⁺ channel block (primary) + K⁺ channel block (IKr) |
| Effect on AP | Slows Phase 0 + prolongs Phase 3 repolarization |
| ECG changes | Wide QRS + prolonged QT |
| Use | Pre-excited atrial arrhythmias, ventricular arrhythmias |
Drug-specific high-yield toxicities:
- Quinidine: Cinchonism (tinnitus, headache, visual disturbances), hemolytic anemia, torsades de pointes, thrombocytopenia
- Procainamide: Drug-induced lupus-like syndrome (reversible), hypotension; active metabolite NAPA (N-acetylprocainamide) can cause torsades in renal failure patients
- Disopyramide: Significant antimuscarinic effects (urinary retention, dry mouth); can precipitate heart failure
Class IB - Fast dissociation, SHORTENS APD
Drugs: Lidocaine, Mexiletine
| Feature | Details |
|---|---|
| Mechanism | Na⁺ channel block (activated and inactivated channels); fast kinetics |
| Effect on AP | Does NOT prolong - may actually shorten action potential |
| ECG changes | Minimal effect on QRS/QT |
| Use | Ventricular arrhythmias only (VT, VF post-cardioversion); NOT effective for atrial arrhythmias |
| Why only ventricles? | Preferentially binds frequently firing (diseased/ischemic) tissue |
Key toxicities:
- Lidocaine: IV only (extensive first-pass if oral). Neurologic toxicity - tremor, paresthesias, confusion, seizures
- Mexiletine: Oral lidocaine analogue; GI side effects (nausea, dyspepsia)
Class IC - Slow dissociation, NO CHANGE in APD
Drugs: Flecainide, Propafenone
| Feature | Details |
|---|---|
| Mechanism | Potent Na⁺ channel block; very slow dissociation |
| Effect on AP | Markedly slows Phase 0 (greatest QRS widening of all class I) |
| Use | SVT in structurally normal hearts; atrial fibrillation/flutter |
| CONTRAINDICATION | Post-MI / ischemic heart disease - CAST trial showed increased mortality |
Propafenone extra: Has weak beta-blocking activity; can cause bronchospasm
Class II - Beta-Blockers
Drugs: Propranolol, Metoprolol, Esmolol, Atenolol
| Feature | Details |
|---|---|
| Mechanism | β-adrenergic receptor blockade → inhibits Phase 4 depolarization in SA and AV nodes |
| Effect | Slows SA node automaticity + slows AV nodal conduction |
| ECG changes | Prolonged PR interval, bradycardia |
| Use | Atrial arrhythmias (AFib rate control), SVT, prevention of recurrent MI/sudden death |
High-yield: Esmolol is ultra-short acting (IV only), used for acute/intraoperative arrhythmias.
Toxicities: Bradycardia, AV block, bronchospasm (contraindicated in asthma), hypoglycemia masking, fatigue, sexual dysfunction
Class III - Potassium Channel Blockers (prolong repolarization)
Drugs: Amiodarone, Sotalol, Dofetilide, Ibutilide, Dronedarone
All prolong Phase 3 (K⁺ channel block → widened AP → prolonged QT). Risk of torsades de pointes.
Amiodarone (the "dirty drug" - most important for exams)
| Feature | Details |
|---|---|
| Mechanism | Blocks K⁺ (IKr), Na⁺, Ca²⁺ channels + β-adrenoceptors - all four classes! |
| Uses | Serious ventricular arrhythmias (VT, VF), AFib |
| Half-life | Extremely long: 40-55 days |
| Paradox | Low incidence of torsades despite QT prolongation |
Toxicities (must memorize - huge exam target):
- Pulmonary toxicity - pneumonitis, fibrosis (most serious)
- Hepatotoxicity - transaminase elevation, cirrhosis
- Thyroid dysfunction - both hypo- and hyperthyroidism (contains iodine; structurally like T4)
- Corneal microdeposits - reversible; optic neuritis (rare)
- Blue-gray skin discoloration (sun-exposed areas)
- Peripheral neuropathy
- Many drug interactions via CYP inhibition (raises levels of warfarin, digoxin, statins)
Other Class III drugs
| Drug | Key feature |
|---|---|
| Dofetilide | Pure IKr blocker; oral; used for AFib - must be initiated in hospital with ECG monitoring due to torsades risk; renally excreted |
| Ibutilide | IV only; conversion of acute AFib/atrial flutter; risk of torsades |
| Sotalol | Has both Class II (beta-block) AND Class III actions; used for AFib + ventricular arrhythmias |
| Dronedarone | Amiodarone derivative without iodine; multichannel actions; reduces mortality in AFib; contraindicated in severe heart failure |
Class IV - Calcium Channel Blockers
Drugs: Verapamil, Diltiazem (non-dihydropyridines only)
| Feature | Details |
|---|---|
| Mechanism | Block L-type Ca²⁺ channels → inhibit SA and AV node action potentials |
| Effect | Slows SA node automaticity + AV nodal conduction |
| ECG changes | Prolonged PR interval |
| Use | SVT (AVNRT termination), rate control in AFib/flutter |
Toxicities: Bradycardia, AV block, hypotension, acute heart failure, peripheral edema, constipation (verapamil > diltiazem)
Critical contraindication: Never use verapamil/diltiazem in WPW + AFib (blocks AV node, drives conduction down accessory pathway - can cause VF)
"Other" Antiarrhythmic Drugs
| Drug | Mechanism | Use | Key facts |
|---|---|---|---|
| Adenosine | Activates K⁺ channels → hyperpolarizes; slows/blocks AV node | Drug of choice for acute SVT termination | Ultra-short half-life (~10 sec); transient chest pain/flushing/dyspnea; antagonized by caffeine/theophylline |
| Digoxin | Inhibits Na⁺/K⁺-ATPase → increased vagal tone → slows AV node | Rate control in AFib | Narrow therapeutic window; toxicity: visual disturbances (yellow-green halos), GI symptoms, any arrhythmia |
| Magnesium sulfate | Stabilizes cell membrane | Torsades de pointes (drug of choice), digoxin toxicity arrhythmias | IV only; also used in eclampsia |
Drug-to-Arrhythmia Matching (Exam Favorite)
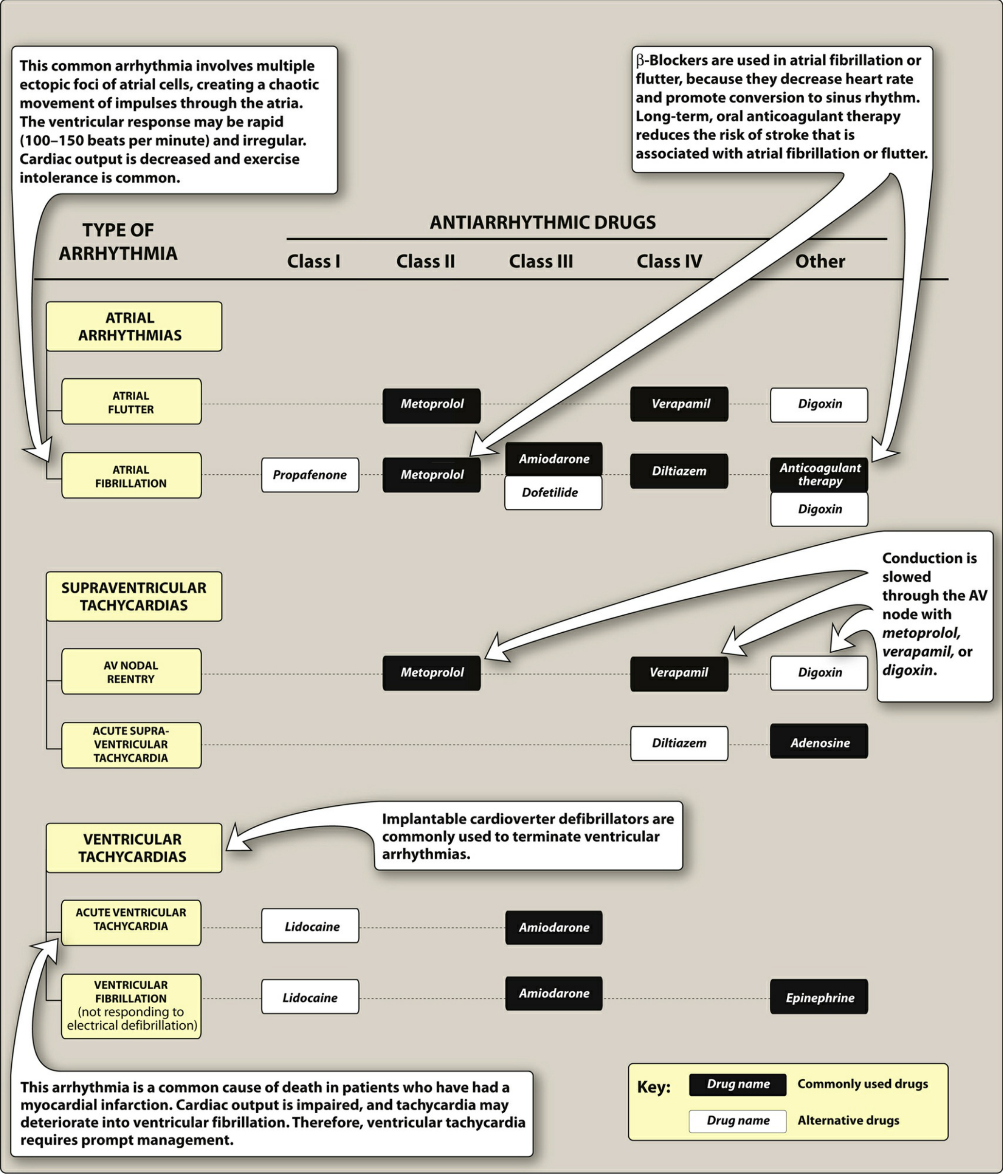
| Arrhythmia | First-line | Alternatives |
|---|---|---|
| Acute SVT | Adenosine | Verapamil, diltiazem |
| AFib rate control | Metoprolol | Verapamil, diltiazem, digoxin |
| AFib rhythm control | Amiodarone, dofetilide | Flecainide (normal heart), propafenone |
| Acute VT | Amiodarone, lidocaine | - |
| VF (refractory) | Amiodarone + epinephrine | Lidocaine |
| Torsades de pointes | Magnesium sulfate (IV) | Correct underlying QT cause |
| WPW + SVT | Procainamide | Avoid AV nodal blockers |
QT-Prolonging Drugs (High-Yield for Exams)
The following antiarrhythmics prolong QT and can cause torsades de pointes (polymorphic VT):
- Class IA: Quinidine > procainamide, disopyramide
- Class III: Sotalol, dofetilide, ibutilide (amiodarone - low risk despite QT prolongation)
Risk is amplified by: hypokalemia, hypomagnesemia, bradycardia, female sex, congenital long QT
Quick Mnemonics
- Class IA: "Quinidine Promotes Depolarization" (Quinidine, Procainamide, Disopyramide)
- Amiodarone toxicity: "PLATE" - Pulmonary, Liver, Athyroid, Thyroid, Eye (corneal)
- Adenosine reversal: Caffeine and theophylline are xanthines that block adenosine receptors - they antagonize its effect
- Class IC + MI = Bad: CAST trial - flecainide/encainide increased mortality post-MI despite suppressing PVCs
Sources: Lippincott Illustrated Reviews: Pharmacology; Katzung's Basic and Clinical Pharmacology 16e; Goodman & Gilman's Pharmacological Basis of Therapeutics
Congestive heart failure
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, exam-focused guide to Congestive Heart Failure (CHF), compiled from Braunwald's Heart Disease, Textbook of Family Medicine, and associated pharmacology sources.
Congestive Heart Failure - Complete Study Guide
Definition
Heart failure (HF) is a clinical syndrome resulting from the inability of the heart to meet the metabolic requirements of the body at normal filling pressures. It presents with dyspnea, fatigue, and fluid retention. The term "congestive" heart failure is older - current guidelines prefer heart failure because pulmonary congestion may actually be absent.
Classification
By Ejection Fraction (Modern, Most Important)
| Type | EF | Mechanism | Also called |
|---|---|---|---|
| HFrEF | < 40-45% | Reduced LV contraction (systolic dysfunction) | Systolic HF |
| HFmrEF | 40-49% | Mildly reduced | - |
| HFpEF | ≥ 50% | Impaired LV filling/relaxation (diastolic dysfunction) | Diastolic HF |
ACC/AHA Staging (A-D) - "Cannot go backward"
| Stage | Description | NYHA Equivalent |
|---|---|---|
| A | At risk (HTN, DM, CAD, FHx cardiomyopathy) - no structural disease, no symptoms | None |
| B | Structural heart disease, no symptoms (e.g., asymptomatic LV dysfunction) | Class I |
| C | Structural disease + current or prior HF symptoms | Class II-III |
| D | Refractory HF requiring advanced therapies | Class IV |
NYHA Functional Classification (Symptom severity)
| Class | Symptoms |
|---|---|
| I | No symptoms with ordinary activity |
| II | Slight limitation - comfortable at rest, symptoms with moderate exertion |
| III | Marked limitation - comfortable at rest, symptoms with minimal exertion |
| IV | Symptoms at rest; unable to carry on any activity without discomfort |
Causes / Etiology
Most common overall: Ischemic heart disease (CAD/MI) and hypertension
| Low-output HF (most common) | High-output HF |
|---|---|
| CAD, MI | Hyperthyroidism |
| Hypertension | Severe anemia |
| Valvular disease (AR, MR, AS) | Beriberi (thiamine deficiency) |
| Dilated cardiomyopathy | Paget disease |
| Myocarditis | AV malformations |
| Tachycardia-induced CM | Multiple myeloma |
Precipitants of acute decompensation (PIRATES mnemonic):
Pulmonary embolism, Infection, Rheumatic heart disease / valvular, Anemia / A-fib, Thyrotoxicosis, Endocarditis, Salt excess / medication non-compliance
Pathophysiology
The key concept is LV remodeling - progressive dilation and dysfunction of the LV, driven by two neurohormonal systems:
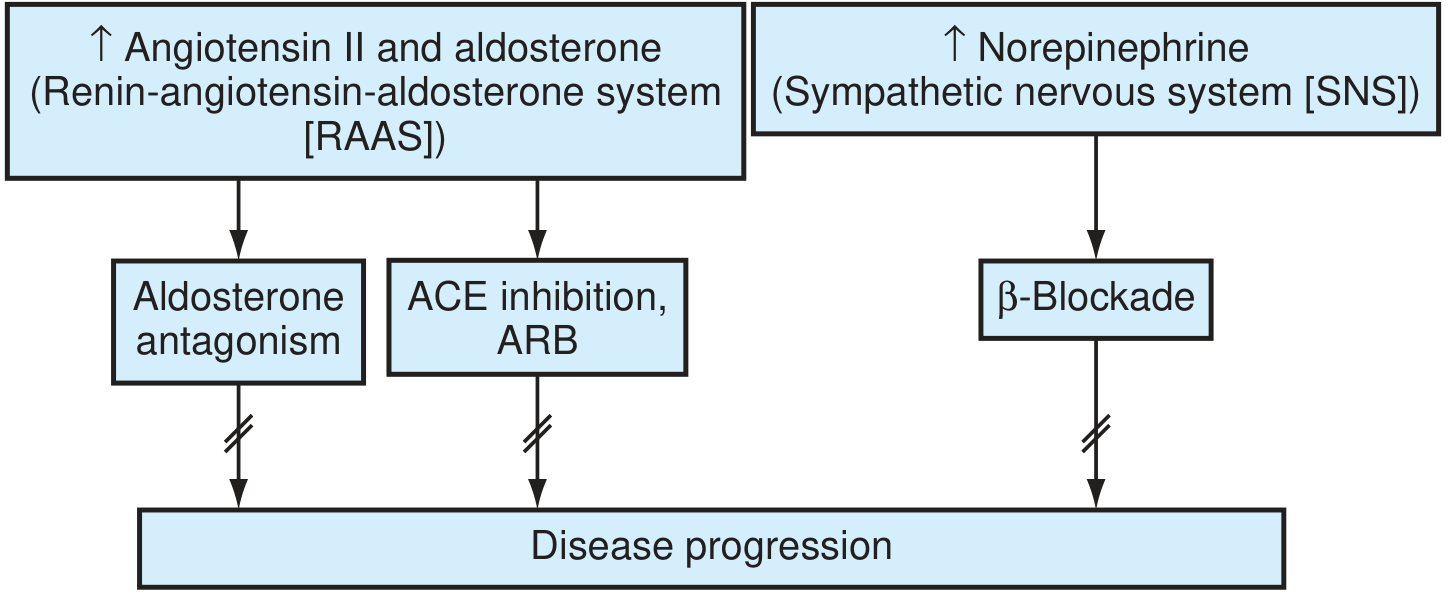
Two Harmful Neurohormonal Cascades:
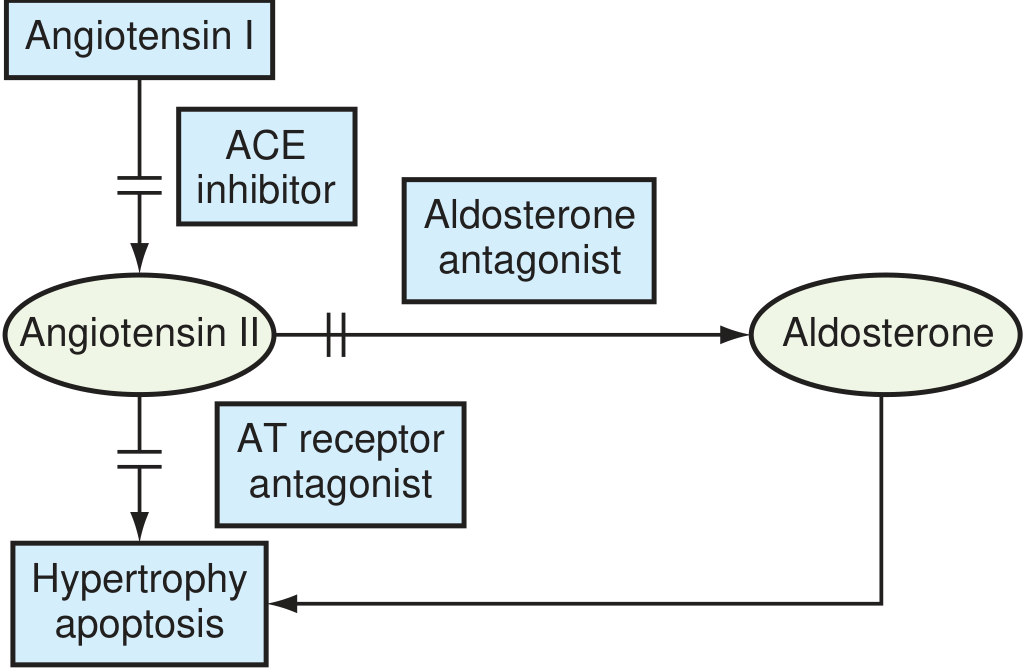
1. RAAS Activation:
- Low CO → renin → Angiotensin I → ACE → Angiotensin II
- AII → vasoconstriction, myocyte hypertrophy, apoptosis, ventricular fibrosis
- AII → aldosterone → Na⁺/water retention → increased preload → worsens congestion
2. Sympathetic Nervous System Activation:
- Low CO → ↑ norepinephrine → tachycardia, vasoconstriction
- Catecholamines → direct myocardial toxicity (Ca²⁺ overload), LVH, arrhythmias, ↑ O₂ demand
- Chronic: downregulation of β-adrenergic receptors
Both cascades are targets for pharmacotherapy - blocking them reverses remodeling and reduces mortality.
Clinical Features
Symptoms
| Left HF | Right HF |
|---|---|
| Dyspnea on exertion (earliest) | Peripheral pitting edema |
| Orthopnea (2-3 pillow) | Ascites |
| Paroxysmal nocturnal dyspnea (PND) | Hepatomegaly / RUQ discomfort |
| Fatigue, exercise intolerance | Jugular venous distension (JVD) |
| Cardiac cough | Anorexia, nausea |
Signs
- JVD (most reliable sign of elevated venous pressure)
- S3 gallop (pathological, sign of volume overload / dilated LV)
- S4 gallop (stiff, non-compliant LV - diastolic dysfunction)
- Displaced, sustained apical impulse
- Bilateral basal crackles (pulmonary edema)
- Cheyne-Stokes breathing (severe HF)
- Cool peripheries (low CO)
Investigations
| Test | Findings |
|---|---|
| BNP / NT-proBNP | Elevated - best screening/monitoring biomarker; rules out HF if low |
| ECG | LVH, Q waves (prior MI), LBBB, arrhythmias |
| CXR | Cardiomegaly, pulmonary vascular redistribution, Kerley B lines, pleural effusions |
| Echocardiogram | GOLD STANDARD - EF, wall motion, valves, diastolic function |
| BMP / LFTs | Hyponatremia (poor prognosis), renal impairment, hepatic congestion |
| CBC | Anemia as cause or exacerbant |
| TFTs | Thyroid disease as cause |
CXR in CHF - "ABCDE":
- Alveolar edema ("bat wing" opacities)
- B-lines (Kerley B lines - interstitial edema)
- Cardiomegaly (CTR > 0.5)
- Distended upper lobe veins (vascular redistribution)
- Effusions (pleural)
Pharmacological Management
HFrEF - Evidence-Based Drug Therapy (MORTALITY-REDUCING DRUGS)
The "fantastic four" drugs that reduce mortality in HFrEF:
1. ACE Inhibitors / ARBs (RAAS Blockade)
| Drug | Key Trial | Benefit |
|---|---|---|
| Enalapril, ramipril, lisinopril | SOLVD, AIRE | ↓ mortality, ↓ hospitalizations, reverse remodeling |
| Valsartan, candesartan (ARBs) | Val-HeFT | Use if ACE inhibitor intolerant (cough) |
| Sacubitril/Valsartan (ARNI) | PARADIGM-HF | Superior to enalapril - now preferred over ACE-i in stable HFrEF |
ACE inhibitor side effects: Dry cough (bradykinin), hyperkalemia, angioedema (switch to ARB), renal impairment, hypotension
CONTRAINDICATED in: Pregnancy, bilateral RAS, hyperkalemia, angioedema history
2. Beta-Blockers
| Drug | Key Trial |
|---|---|
| Carvedilol | US Carvedilol, COPERNICUS |
| Metoprolol succinate (CR/XL) | MERIT-HF |
| Bisoprolol | CIBIS-II |
- Block harmful effects of catecholamines, reverse remodeling, reduce sudden cardiac death
- Start low, go slow - never start during acute decompensation
- Reduce resting heart rate to 55-60 bpm target
- Carvedilol also has alpha-1 blocking (vasodilatory) properties
3. Mineralocorticoid Receptor Antagonists (MRAs)
| Drug | Key Trial |
|---|---|
| Spironolactone | RALES - 30% mortality reduction |
| Eplerenone | EMPHASIS-HF (post-MI HF) |
- Block aldosterone escape, reduce cardiac fibrosis
- Watch for: Hyperkalemia, gynecomastia (spironolactone)
- Use if K⁺ < 5.0 mmol/L and GFR > 30
4. SGLT2 Inhibitors (newest pillar - now standard of care)
| Drug | Key Trial |
|---|---|
| Dapagliflozin | DAPA-HF |
| Empagliflozin | EMPEROR-Reduced |
- Reduce HF hospitalizations and cardiovascular death regardless of diabetes status
- Mechanism in HF: osmotic diuresis, reduced preload/afterload, improved cardiac metabolism
- Also benefit HFpEF (EMPEROR-Preserved, DELIVER trials)
Additional Drugs
| Drug | Indication | Notes |
|---|---|---|
| Loop diuretics (furosemide, bumetanide) | Symptomatic relief of congestion | No mortality benefit; use for fluid overload; monitor K⁺, Cr |
| Hydralazine + Isosorbide dinitrate | HFrEF - especially in Black patients (A-HeFT trial) | Alternative if ACE-i/ARB not tolerated; also additional therapy in Black patients |
| Digoxin | Rate control in AFib + HF; reduces hospitalizations in HFrEF | No mortality benefit; narrow therapeutic window |
| Ivabradine | HR ≥ 70 bpm in sinus rhythm on max beta-blocker | Reduces hospitalizations; blocks funny current (If) in SA node |
HFpEF Management
Fewer evidence-based therapies than HFrEF:
- Treat underlying cause (HTN, AFib, volume overload)
- Diuretics for congestion symptoms
- SGLT2 inhibitors (dapagliflozin, empagliflozin) - now shown to reduce hospitalizations
- BP control (target < 130/80 mmHg)
- Rate control for AFib (non-dihydropyridine CCBs are safe here, unlike HFrEF)
Drugs to AVOID in HFrEF
| Drug | Reason |
|---|---|
| Non-dihydropyridine CCBs (verapamil, diltiazem) | Negative inotropy - worsen systolic function |
| NSAIDs / COX-2 inhibitors | Na⁺ retention, worsen renal function, blunt diuretic response |
| Thiazolidinediones (glitazones) | Fluid retention |
| Class IC antiarrhythmics (flecainide) | Increased mortality in structural heart disease |
| Dronedarone | Increased mortality in severe HF |
Device Therapy (Non-Pharmacologic)
| Device | Indication |
|---|---|
| ICD (implantable cardioverter-defibrillator) | EF ≤ 35%, NYHA II-III, on optimal medical therapy for ≥ 3 months - primary prevention of sudden death |
| CRT (cardiac resynchronization therapy) | EF ≤ 35% + LBBB with QRS ≥ 150 ms + NYHA III-IV - improves symptoms and mortality |
| CRT-D | Combined CRT + ICD |
| Cardiac transplant | Stage D (refractory) HF |
Quick Summary: Drug Targets in HF
| System | Drug Class | Examples |
|---|---|---|
| RAAS (ACE) | ACE inhibitors | Enalapril, lisinopril |
| RAAS (AT1 receptor) | ARBs | Valsartan, candesartan |
| RAAS (neprilysin + AT1) | ARNI | Sacubitril/valsartan |
| RAAS (aldosterone) | MRAs | Spironolactone, eplerenone |
| SNS (β1/β2/α1) | Beta-blockers | Carvedilol, metoprolol, bisoprolol |
| Glucose transporter | SGLT2 inhibitors | Dapagliflozin, empagliflozin |
| Volume overload | Loop diuretics | Furosemide, bumetanide |
| SA node If current | Ivabradine | Ivabradine |
Key Exam High-Yield Points
- BNP is the best biomarker for HF diagnosis and monitoring
- Echocardiogram is the investigation of choice
- S3 gallop = volume overload (HFrEF); S4 gallop = stiff LV (HFpEF)
- Sacubitril/valsartan is now preferred over ACE inhibitors in stable HFrEF (PARADIGM-HF)
- SGLT2 inhibitors are the newest pillar - benefit in both HFrEF and HFpEF
- Beta-blockers reduce sudden cardiac death (↓ mortality from arrhythmia)
- Spironolactone - monitor K⁺; contraindicated if K⁺ > 5.0 or GFR < 30
- Carvedilol is preferred over non-selective beta-blockers (also blocks alpha-1)
- Only amiodarone and dofetilide are safe antiarrhythmics in HF
- ACC/AHA stages cannot go backward (unlike NYHA which can improve with treatment)
Sources: Textbook of Family Medicine 9e; Braunwald's Heart Disease 2 Vol Set; Lippincott Illustrated Reviews Pharmacology; Katzung's Basic and Clinical Pharmacology 16e
Acute
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete, exam-focused guide to Acute Heart Failure (AHF), compiled from Tintinalli's Emergency Medicine, Braunwald's Heart Disease, Brenner & Rector's The Kidney, Katzung's Pharmacology, and Guyton & Hall Physiology.
Acute Heart Failure - Complete Study Guide
Definition
Acute heart failure (AHF) is the rapid onset or worsening of signs and symptoms of heart failure, requiring urgent therapy. It encompasses:
- New-onset AHF - first presentation (e.g., large MI, acute valvular rupture)
- Acute-on-chronic HF - decompensation of previously stable chronic HF (most common)
Pathophysiology
What happens immediately after acute cardiac damage
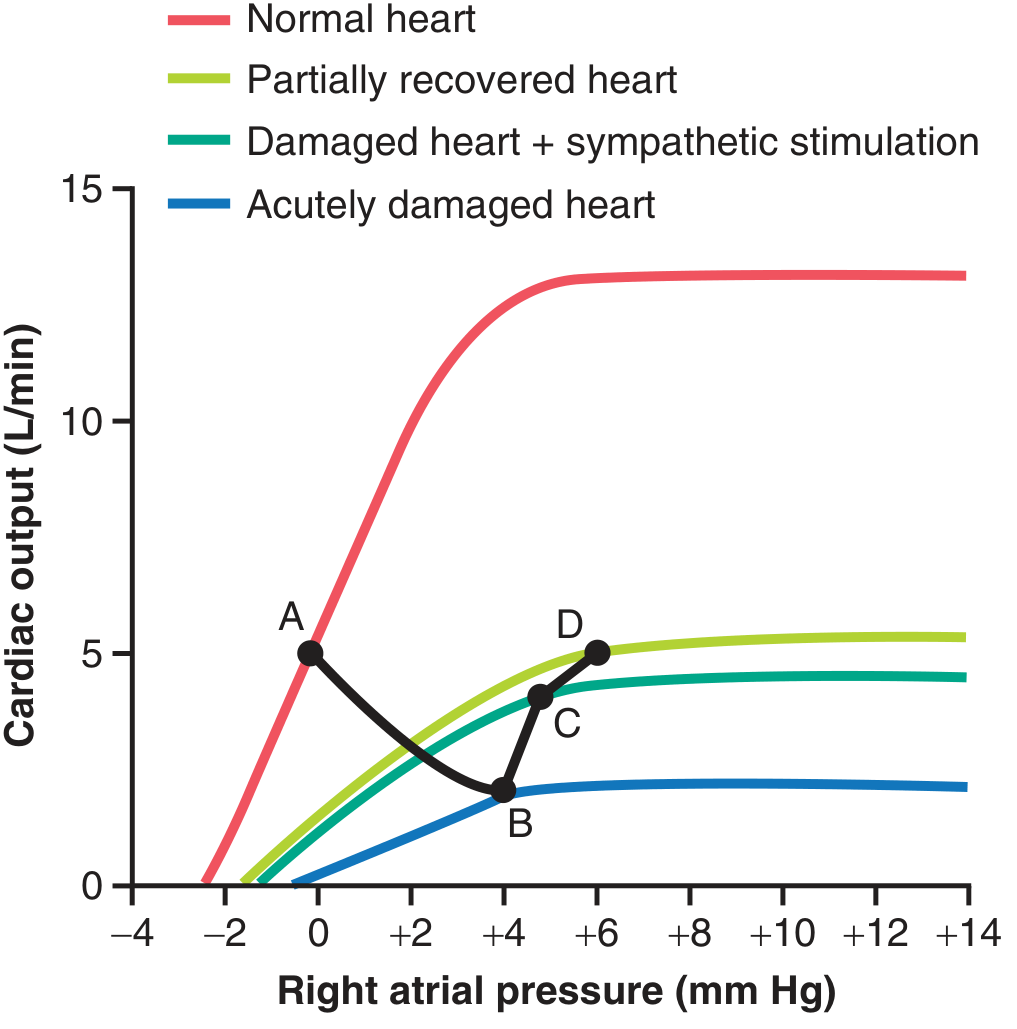
| Point | State | CO | RAP |
|---|---|---|---|
| A | Normal | 5 L/min | 0 mmHg |
| B | Acutely damaged heart | ~2 L/min | +4 mmHg |
| C | Damaged + sympathetic compensation | ~3.5 L/min | +5 mmHg |
| D | Partial recovery over days-weeks | ~5 L/min | +6 mmHg |
Neurohormonal cascade (from Guyton & Hall)
- Cardiac output falls → baroreceptors fire → sympathetic nervous system activated
- Norepinephrine released → tachycardia, vasoconstriction, increased venous return (↑ preload)
- Renal perfusion falls → RAAS activated → angiotensin II + aldosterone → Na⁺/water retention
- Vasopressin (ADH) released → water retention
- Endothelin-1 → potent vasoconstriction
- TNF-α, cytokines → endothelial dysfunction
- Net result: ↑ filling pressures → pulmonary and peripheral congestion
These short-term compensations maintain blood pressure but increase myocardial O₂ demand and worsen pump function over time.
Clinical Classification of AHF (6 Phenotypes - Tintinalli)
This is the most important classification for emergency management because each phenotype has a different treatment approach:
| Phenotype | BP | Key Features | Primary Treatment |
|---|---|---|---|
| Hypertensive AHF | SBP > 140 mmHg | Rapid onset (< 48h), pulmonary edema, relatively preserved EF | Vasodilators first (nitrates) |
| Pulmonary edema | Variable | Resp distress, rales, ↓ SpO₂, CXR changes | O₂/NIV + vasodilators |
| Cardiogenic shock | SBP < 90 mmHg | Tissue hypoperfusion, cold/clammy | Inotropes + revascularization |
| Acute-on-chronic HF | 90-140 mmHg | Gradual worsening over days, edema, weight gain | Diuretics |
| High-output HF | Normal/high | Warm extremities, tachycardia; EF preserved; cause: anemia, thyrotoxicosis | Treat underlying cause |
| Right heart failure | Low-normal | JVD, hepatomegaly, edema; little pulmonary congestion | Treat cause; avoid aggressive diuresis |
Common Precipitants of Acute Decompensation
Mnemonic: PIRATES
- P - Pulmonary embolism
- I - Infection (pneumonia, sepsis)
- R - Rhythm disorder (new AFib most common)
- A - Anemia / Acute MI
- T - Treatment non-compliance (salt, fluids, medications)
- E - Endocrine (thyrotoxicosis)
- S - Substance abuse (alcohol, cocaine) / Salt excess
Clinical Features
Symptoms
| Left-sided congestion | Right-sided congestion | Low output |
|---|---|---|
| Dyspnea (most common) | Peripheral edema | Fatigue, weakness |
| Orthopnea | Ascites | Cold extremities |
| Paroxysmal nocturnal dyspnea | RUQ discomfort | Confusion, oliguria |
| Cardiac cough | Anorexia, nausea | Hypotension (severe) |
Signs
- Tachycardia, tachypnea
- JVD (elevated venous pressure)
- Bilateral basal crackles (pulmonary edema)
- S3 gallop (volume overload)
- Peripheral pitting edema
- Displaced/sustained apex beat
- Hepatomegaly, hepatojugular reflux
Investigations
| Test | Key Finding |
|---|---|
| BNP / NT-proBNP | Most useful single test - markedly elevated; useful to distinguish cardiac vs. respiratory dyspnea |
| CXR | Cardiomegaly, pulmonary vascular redistribution, Kerley B lines, pleural effusions, bat-wing pulmonary edema |
| ECG | Look for precipitant: MI (ST changes), AF, LBBB |
| Echo (urgent) | EF, wall motion abnormalities, pericardial effusion, valvular cause |
| Troponin | Rule out ACS as precipitant |
| BMP | Hyponatremia (poor prognosis), creatinine (diuretic resistance), K⁺ |
| ABG/SpO₂ | Severity of respiratory failure |
BNP Interpretation:
- BNP < 100 pg/mL: HF unlikely
- BNP > 400 pg/mL: HF likely
- Grey zone 100-400: consider other causes (PE, COPD, renal failure also raise BNP)
Emergency Management
Immediate Priorities (ABC approach)
- Airway/Breathing - oxygen to maintain SpO₂ ≥ 95%
- Sit patient upright - reduces preload
- IV access + monitoring - ECG, SpO₂, urine output
- Identify and treat precipitant
Treatment by Phenotype
A. Hypertensive AHF / Pulmonary Edema
Goal: Rapid afterload and preload reduction
Step 1 - Vasodilators (first-line, before diuretics)
| Drug | Route | Dose | Mechanism |
|---|---|---|---|
| Nitroglycerin (NTG) | SL | 0.4 mg (1-2 sprays) q5 min | Venodilatation (↓ preload) at low dose; arteriodilatation (↓ afterload) at high dose |
| IV NTG | IV | Start 0.5-0.7 mcg/kg/min; titrate up to 200 mcg/min | Titrate to symptoms |
| Nitroprusside | IV | 0.25-10 mcg/kg/min | Balanced arterio/venodilator; use in severe hypertension |
| Nesiritide | IV | Recombinant BNP | Vasodilation + natriuresis; alternative if dyspneic despite IV diuretics without hypotension |
- Key point: In hypertensive AHF, fluid redistribution (not overload) is the main problem - symptoms may resolve with vasodilators alone without needing large doses of diuretics
- NTG complication: hypotension (give 250-1000 mL NS if persistent)
Step 2 - Loop diuretics (if volume overload)
| Drug | IV dose | Notes |
|---|---|---|
| Furosemide | 1-2.5x usual oral dose IV q12h | DOSE trial: reasonable starting strategy |
| Bumetanide | 1 mg = furosemide 40 mg | |
| Torsemide | 20 mg = furosemide 40 mg | Better oral bioavailability; may reduce re-admission |
- IV preferred over oral in acute setting (bowel wall edema reduces oral absorption)
- Onset of diuresis: ~10-15 minutes IV
- Monitor: K⁺, Cr, urine output (target 0.5-1 mL/kg/hr)
- If inadequate response: double dose and repeat in 30-60 min; consider adding acetazolamide
Step 3 - Non-invasive ventilation (NIV)
- CPAP or BiPAP if severe dyspnea or hypoxia despite O₂
- Reduces work of breathing and need for intubation
- Indicated: SpO₂ < 90% despite O₂, RR > 25, PaCO₂ rising
B. Normotensive AHF (Acute-on-Chronic)
- Loop diuretics first
- Titrate based on urine output and symptoms
- Add vasodilator if congestion persists despite diuretics
- Continue chronic HF medications if tolerated
C. Cardiogenic Shock (SBP < 90 mmHg)
Goal: Restore perfusion pressure and cardiac output
| Drug | Mechanism | Dose | Use |
|---|---|---|---|
| Dobutamine | β1 agonist - positive inotropy | 2-20 mcg/kg/min IV | Preferred inotrope; normotensive/mild hypotension |
| Dopamine | β1 + α1 (dose-dependent) | 5-20 mcg/kg/min IV | Hypotension; high doses worsen vasoconstriction |
| Norepinephrine | α1 dominant vasoconstriction | 0.01-3 mcg/kg/min | Vasopressor for refractory hypotension |
| Milrinone | PDE-3 inhibitor (inodilator) | 0.375-0.75 mcg/kg/min | Inotrope + vasodilator; useful in PCWP elevation |
| Levosimendan | Calcium sensitizer | IV infusion | Non-inferior to dobutamine; approved in Europe |
- Inotropes reserved for: hypotension, end-organ dysfunction, unresponsive to standard therapy
- Consider IABP (intra-aortic balloon pump) or ECMO in refractory cardiogenic shock
- Urgent revascularization if ACS-related (PCI/CABG)
D. High-Output Heart Failure
- Treat the underlying cause (transfuse for anemia, antithyroid drugs for thyrotoxicosis, thiamine for beriberi)
- Diuretics if congested, but avoid excessive volume removal
E. Right Heart Failure
- Identify cause (PE? Pulmonary HTN? RV infarct? Valvular?)
- Avoid aggressive diuresis - RV is preload dependent
- Treat underlying cause
- Optimize right ventricular preload carefully
Medications Table Summary
| Drug | Class | Route | Key Use | Main Risk |
|---|---|---|---|---|
| Furosemide | Loop diuretic | IV/PO | Volume overload | Hypokalemia, hypovolemia |
| Nitroglycerin | Venodilator | SL/IV | Hypertensive AHF, pulmonary edema | Hypotension, headache |
| Nitroprusside | Balanced vasodilator | IV | Severe hypertensive AHF | Cyanide toxicity (prolonged use) |
| Dobutamine | Inotrope | IV | Cardiogenic shock | Tachyarrhythmias |
| Milrinone | Inodilator | IV | Cardiogenic shock | Hypotension |
| Nesiritide | Recombinant BNP | IV | Volume overload + dyspnea | Hypotension, renal impairment |
| Morphine | Opioid | IV | (Historically used) - now controversial; may worsen outcomes | Respiratory depression |
Disposition / Admission Criteria
Admit to ICU if any:
- Altered mental status
- Persistent hypoxia despite NIV
- Hypotension
- Troponin elevation / ischemic ECG changes
- Tachycardia / tachypnea not responding
- Inadequate urine output
Consider discharge / ED observation if:
- Good response to therapy
- No high-risk features
- Good social support and follow-up
AHF in the Context of Acute MI
- Priority: Rapid coronary reperfusion (PCI or thrombolysis)
- IV furosemide acutely reduces LVEDP in 5-15 minutes via venodilation (before diuresis begins)
- Use diuretics judiciously - avoid reducing preload too aggressively (may reduce CO further)
- Vasodilators (isosorbide dinitrate) + furosemide = best first-line combination in LVF complicating MI
- Inotropes if cardiogenic shock develops
Key Exam Points
- Vasodilators before diuretics in hypertensive AHF (fluid redistribution, not just overload)
- Diuretics first in normotensive acute-on-chronic HF with edema
- CPAP/BiPAP reduces intubation need in pulmonary edema
- Dobutamine = inotrope of choice for cardiogenic shock with near-normal BP
- Avoid morphine in AHF - associated with worse outcomes in recent data
- BNP is the best biomarker; also used to monitor response to treatment
- Torsemide may have advantages over furosemide (better bioavailability, less re-admissions)
- Diuretic resistance: try higher IV dose, add thiazide (metolazone), or consider ultrafiltration
- In AHF + hyponatremia: vasopressin antagonists (tolvaptan, conivaptan) may help symptoms but do NOT reduce mortality
- Nesiritide reduces PCWP but does NOT improve mortality vs. standard therapy
Sources: Tintinalli's Emergency Medicine; Braunwald's Heart Disease; Brenner & Rector's The Kidney; Katzung's Basic & Clinical Pharmacology 16e; Guyton & Hall Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.