Explain me ten common heart diseases with ecg changes and ecg images of those diseases
Reading File
Finding Sources
Finding Sources
Searching the Web
common heart diseases ECG changes with ECG images examples
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Searching the Web
ECG images atrial fibrillation ventricular tachycardia heart block LBBB wikimedia commons site:litfl.com OR site:ecgwaves.com
Loading Image
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
ECG examples STEMI atrial fibrillation ventricular tachycardia complete heart block pericarditis WPW site:ecgwaves.com OR site:litfl.com
Loading Image
Loading Image
Searching the Web
ECG pericarditis PR depression diffuse ST elevation image litfl.com OR ecgwaves.com
Loading Image
Loading Image
I now have comprehensive information from the textbooks and high-quality ECG images. Let me now compose the full, detailed answer.
Ten Common Heart Diseases: ECG Changes and Images
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural myocardial ischemia and necrosis. Three major electrophysiological events drive the ECG changes: abnormally rapid repolarization, decreased resting membrane potential from K+ loss, and delayed depolarization of infarcted fibers - all generating current flow that elevates the ST segment in overlying leads. (Ganong's Review of Medical Physiology, p.534)
ECG Changes:
- Hyperacute T waves - first change, tall peaked T waves in the territory of infarction
- ST-segment elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous precordial leads - the hallmark finding
- Reciprocal ST depression in leads on the opposite side of the heart
- Q-wave formation - pathological Q waves develop within hours to days as necrotic tissue becomes electrically silent (>40 ms wide, >25% of R-wave height)
- T-wave inversion as the infarct evolves
- R-wave loss in the territory of infarction
Localisation by leads:
- Anterior STEMI: V1-V4 (LAD territory)
- Inferior STEMI: II, III, aVF (RCA or LCx territory)
- Lateral STEMI: I, aVL, V5-V6
- Posterior STEMI: Tall R + ST depression in V1-V2 (reciprocal)
Current of injury - subendocardial vs. transmural (Harrison's, Fig. 247-11):

(A = subendocardial ischemia causes ST depression; B = epicardial/transmural ischemia causes ST elevation)
Wellens T-wave sign (anterior ischemia with severe LAD stenosis):

2. Non-ST-Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
Pathophysiology: Partial coronary occlusion causing predominantly subendocardial ischemia, without transmural involvement. Biomarkers are elevated in NSTEMI but not in unstable angina.
ECG Changes:
- ST depression ≥0.5-1 mm in ≥2 contiguous leads (horizontal or downsloping is most concerning)
- T-wave inversions - may be deep and symmetric
- No pathological Q waves in most cases
- Normal ECG in up to 30-50% of confirmed NSTEMI cases - a normal ECG does not exclude the diagnosis
- Transient ST elevation may occur with coronary vasospasm (Prinzmetal's angina), resolving within minutes
(Harrison's Principles, p.1916; Tintinalli's Emergency Medicine)
3. Atrial Fibrillation (AF)
Pathophysiology: Chaotic, disorganized atrial electrical activity from multiple re-entrant wavelets. The AV node is bombarded with thousands of impulses, passing only some irregularly to the ventricles.
ECG Changes:
- Absent P waves - replaced by irregular fibrillatory baseline (f-waves), most visible in V1 and II
- Irregularly irregular RR intervals - the hallmark finding; no two RR intervals are the same
- Normal narrow QRS complex (unless aberrant conduction or bundle branch block)
- Ventricular rate typically 100-180 bpm if uncontrolled
- Coarse AF: prominent, irregular f-waves >1mm (often in valvular/rheumatic AF)
- Fine AF: very low amplitude f-waves, almost isoelectric baseline
(Tintinalli's Emergency Medicine; Rosen's Emergency Medicine)
ECG of Atrial Fibrillation:

4. Ventricular Tachycardia (VT)
Pathophysiology: Rapid ventricular rhythm (>100 bpm, usually 120-250 bpm) arising from ventricular myocardium or His-Purkinje system, bypassing normal conduction. Can be monomorphic (uniform QRS) or polymorphic (varying QRS morphology).
ECG Changes:
- Wide QRS complexes (≥120-140 ms) - most important feature
- Regular or slightly irregular rhythm at 120-250 bpm
- AV dissociation - P waves march through at a different rate, independent of QRS
- Fusion beats - hybrid QRS from simultaneous sinus and ventricular depolarisation
- Capture beats - occasional narrow QRS when sinus impulse captures ventricles
- Concordance in precordial leads - all QRS complexes pointing same direction (positive or negative) strongly suggests VT
- Negative concordance (all precordial QRS negative) is highly specific for VT
- No P wave precedes each QRS
(Tintinalli's Emergency Medicine; Goldman-Cecil Medicine)
12-lead ECG showing monomorphic Ventricular Tachycardia:
5. Complete (Third-Degree) AV Heart Block
Pathophysiology: Complete dissociation between atrial and ventricular electrical activity. No atrial impulses pass through the AV node to the ventricles. An escape rhythm takes over from either the AV junction (narrow QRS, 40-60 bpm) or from the ventricles (wide QRS, 20-40 bpm - the more dangerous pattern).
ECG Changes:
- P waves and QRS complexes march independently - the defining feature
- Atrial rate > ventricular rate always
- Regular PP intervals and regular RR intervals but with no fixed relationship to each other
- Escape QRS morphology:
- Junctional escape: narrow QRS (~40-60 bpm) - block above the Bundle of His
- Ventricular escape: wide bizarre QRS (~20-40 bpm) - block below the Bundle of His
- PR interval varies randomly (no consistent PR relationship)
(Goldman-Cecil Medicine; Washington Manual of Medical Therapeutics)
6. Pericarditis (Acute)
Pathophysiology: Inflammation of the pericardium spreads to the underlying epicardium, producing diffuse superficial myocardial injury. This causes widespread ST-segment and PR-segment changes across multiple leads - distinguishing it from the regional pattern of MI.
ECG Changes (classic 4-stage progression):
- Stage 1 (hours to days): Diffuse concave ("saddle-shaped") ST elevation in most leads (I, II, III, aVF, aVL, V2-V6) + PR depression in the same leads + PR elevation in aVR (reciprocal) + ST depression in aVR and V1
- Stage 2 (days): ST and PR return toward baseline
- Stage 3 (weeks): Diffuse T-wave inversions
- Stage 4: ECG normalises
Key distinguishing features from STEMI:
- ST elevation is diffuse (not regional/territorial)
- ST elevation is concave upward (saddle-shaped), not convex
- No reciprocal ST depression (except aVR and V1)
- PR depression present
- No Q-wave formation
(LITFL ECG Library; Harrison's Principles of Internal Medicine)
ECG of Acute Pericarditis (saddle-shaped ST elevation with PR depression):
7. Left Bundle Branch Block (LBBB)
Pathophysiology: Conduction block in the left bundle branch causes delayed, abnormal depolarisation of the left ventricle. The right ventricle activates first via the right bundle, and the left ventricle activates late via slow cell-to-cell conduction, producing a wide, abnormal QRS.
ECG Changes:
- QRS duration ≥120 ms (complete LBBB)
- Broad notched "M-shaped" R wave in lateral leads (I, aVL, V5, V6) - the "William" pattern
- Deep "W-shaped" QS or rS in V1-V2 - the "Marrow" pattern
- No septal Q waves in leads I, V5, V6 (first part of septal depolarisation is lost)
- ST and T-wave changes discordant with QRS direction - ST depression and T-wave inversion in leads with tall R waves; ST elevation in leads with deep S waves (V1-V3)
- Left axis deviation common
- New LBBB with chest pain is treated as STEMI equivalent (Sgarbossa criteria used to detect MI in the presence of LBBB)
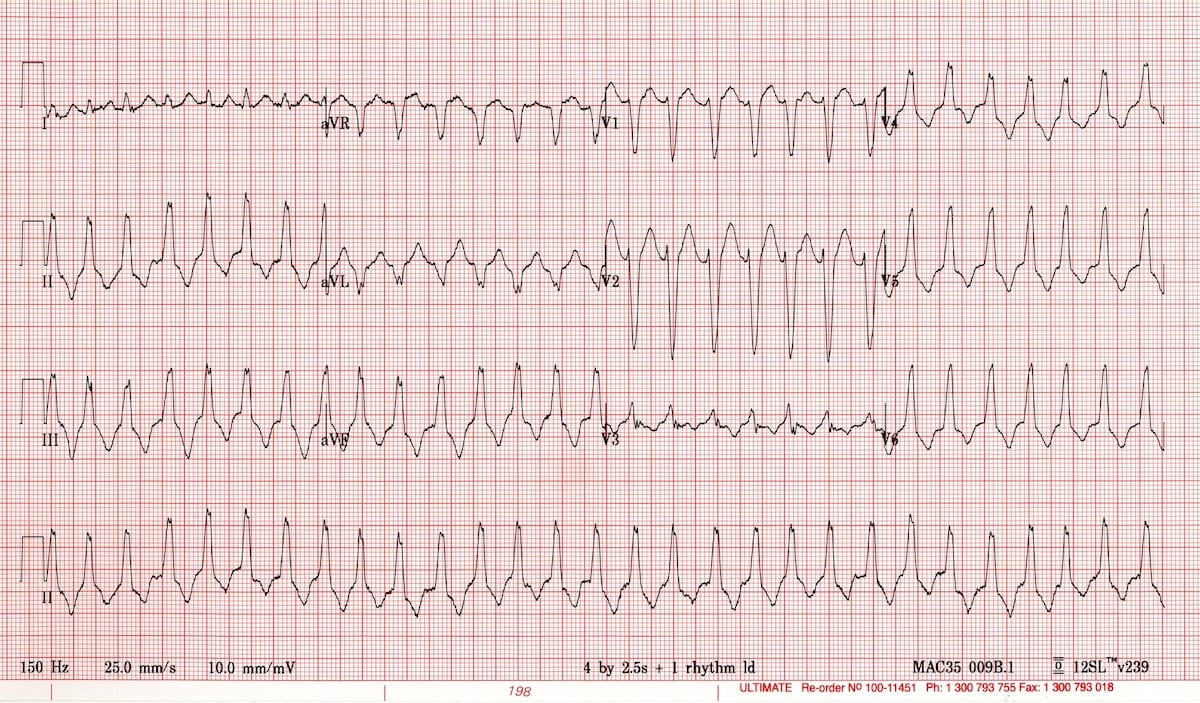
8. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, pre-exciting part of the ventricle before the normal impulse arrives. This produces characteristic ECG findings at rest, and predisposes to dangerous tachyarrhythmias.
ECG Changes (at rest, in sinus rhythm):
- Short PR interval (<120 ms) - bypass of AV nodal delay
- Delta wave - slurred upstroke at the beginning of the QRS (initial slow conduction via accessory pathway)
- Wide QRS (>120 ms) - combination of delta wave + normal conduction
- Secondary ST-T changes discordant with QRS
- Pseudo-infarct patterns (Q waves or ST changes that mimic MI)
During tachycardia:
- Orthodromic AVRT (most common, ~70%): narrow QRS tachycardia (antegrade via AV node, retrograde via accessory pathway)
- Antidromic AVRT (~5-10%): wide QRS tachycardia (antegrade via accessory pathway) - looks identical to VT
- AF with WPW: Irregularly irregular, very rapid (>250 bpm), wide bizarre QRS - life-threatening pattern that can degenerate to VF
(Tintinalli's Emergency Medicine)
WPW ECG showing delta waves and pre-excitation triggering AVRT:

(Left portion shows sinus rhythm with delta waves and short PR; right shows the AVRT tachycardia)
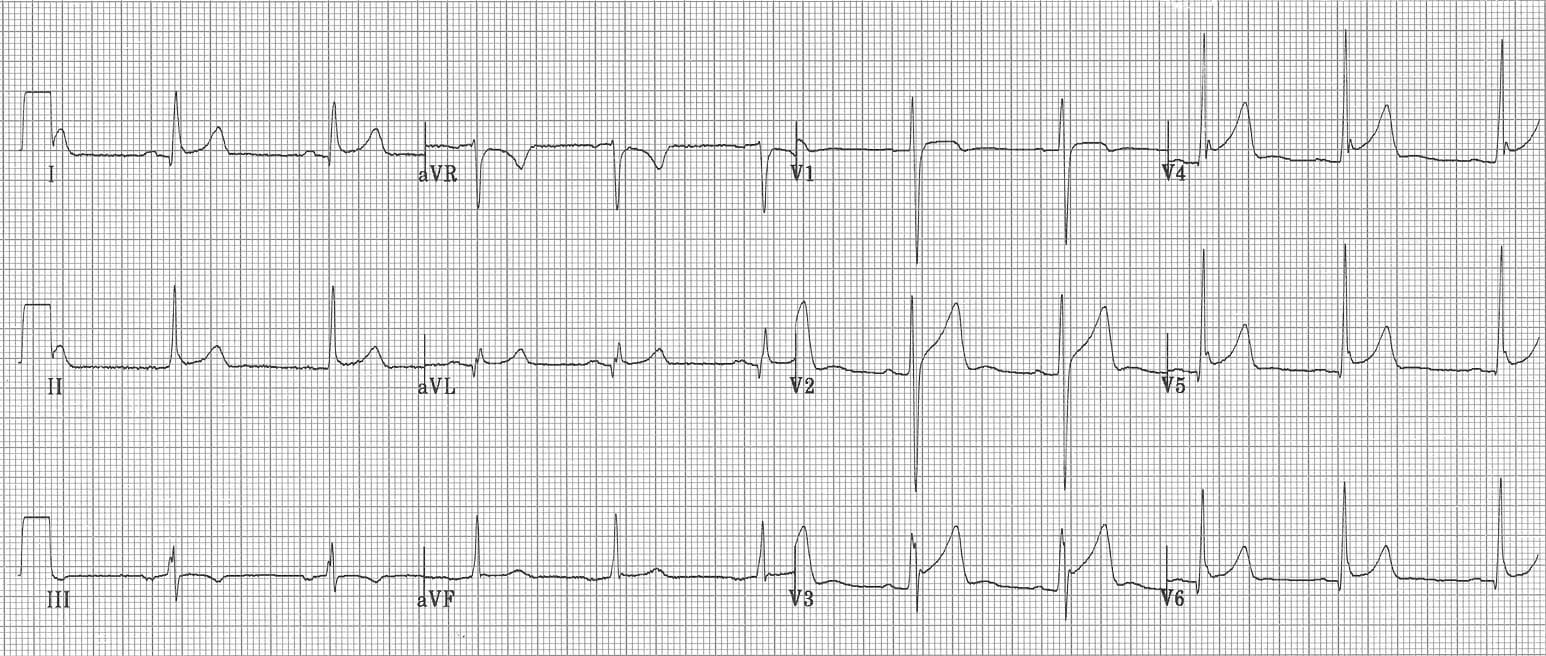
9. Hypertensive Heart Disease / Left Ventricular Hypertrophy (LVH)
Pathophysiology: Chronic pressure overload from hypertension causes concentric hypertrophy of the left ventricular wall. The increased muscle mass generates larger electrical voltages on the ECG.
ECG Changes:
- Increased QRS voltage - the core finding
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm
- Cornell criteria: R in aVL + S in V3 >28 mm (men) or >20 mm (women)
- Left axis deviation
- LV "strain" pattern - ST depression and asymmetric T-wave inversion in lateral leads (I, aVL, V5, V6) - caused by abnormal repolarisation
- Widened QRS (not as wide as BBB, but delayed)
- Left atrial enlargement pattern: biphasic P wave in V1 with prominent negative component; P-wave duration >120 ms in lead II
- Prolonged QRS-T angle
10. Ventricular Fibrillation (VF)
Pathophysiology: Completely chaotic, disorganized ventricular electrical activity with no coordinated contraction. The ventricles quiver without pumping blood - cardiac arrest. VF is the most common initial rhythm in sudden cardiac death.
ECG Changes:
- No identifiable P waves, QRS complexes, or T waves - all organized waveforms are absent
- Irregular, chaotic undulations of varying amplitude and frequency
- Coarse VF: large irregular oscillations (>3 mm amplitude) - more likely to be shocked to sinus rhythm, typically earlier in the arrest
- Fine VF: low amplitude oscillations (<3 mm) - more difficult to shock, often represents prolonged arrest or severe myocardial dysfunction; can mimic asystole
- Heart rate: effectively unmeasurable; chaotic baseline
- Always fatal without immediate defibrillation
Summary Table
| Disease | Key ECG Findings |
|---|---|
| STEMI | ST elevation (convex), Q waves, reciprocal ST depression |
| NSTEMI/Unstable Angina | ST depression, T-wave inversion, may be normal |
| Atrial Fibrillation | Absent P waves, irregularly irregular RR, fibrillatory baseline |
| Ventricular Tachycardia | Wide QRS, AV dissociation, fusion/capture beats |
| Complete Heart Block | P waves and QRS march independently, escape rhythm |
| Acute Pericarditis | Diffuse concave ST elevation, PR depression, no Q waves |
| LBBB | Wide QRS ≥120 ms, M-shape V5/V6, W-shape V1, no septal Q waves |
| WPW Syndrome | Short PR, delta wave, wide QRS; tachyarrhythmias |
| LVH | High voltage, strain pattern (ST-T changes in lateral leads) |
| Ventricular Fibrillation | Chaotic baseline, no organized waveforms |
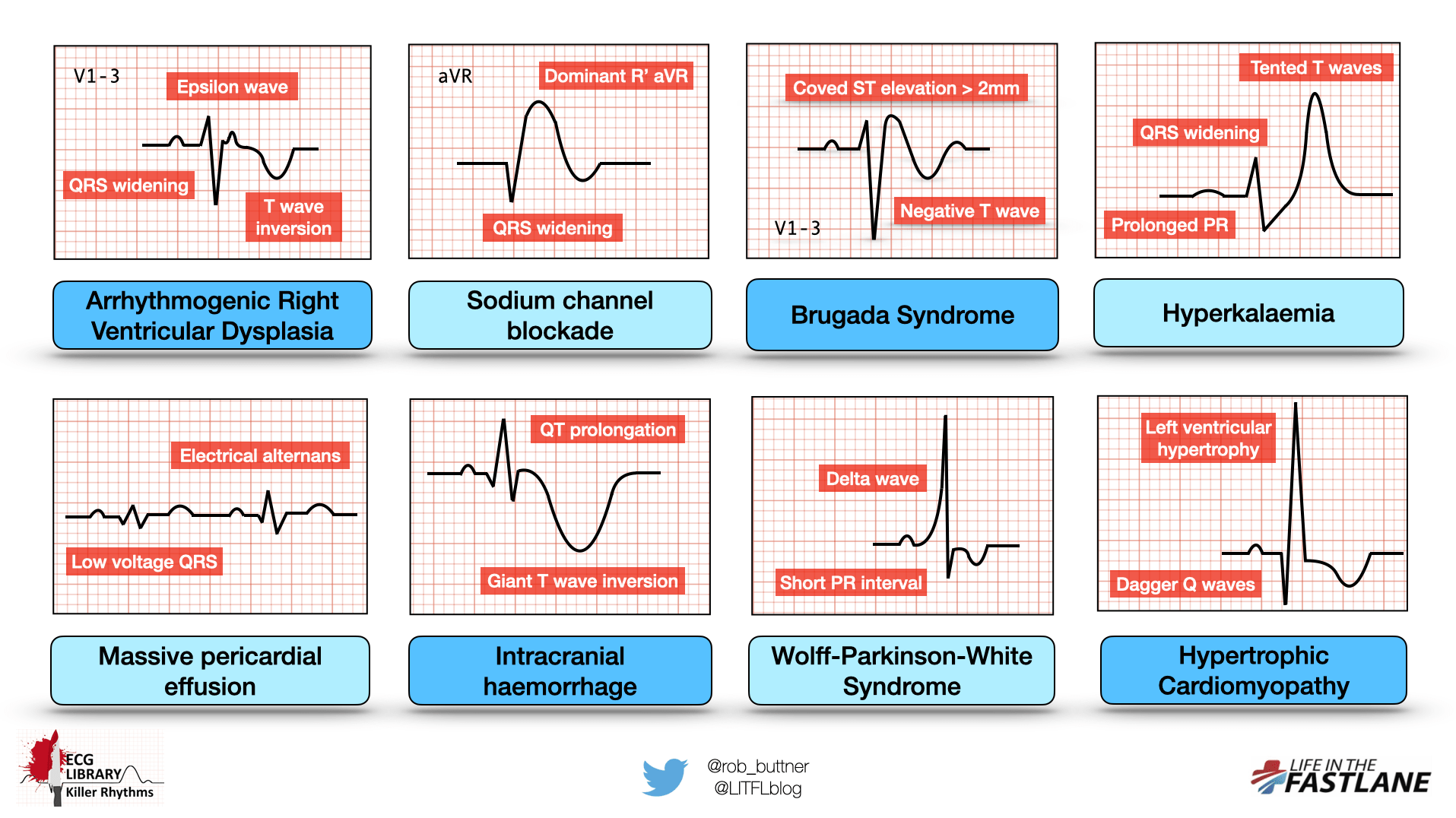
Overview of killer ECG patterns (from LITFL ECG Library):
Clinical note: ECG interpretation must always be correlated with clinical history, examination, and laboratory findings (troponins, BNP, electrolytes). A single normal ECG never excludes acute MI. Serial ECGs and continuous monitoring are often required. (Harrison's Principles of Internal Medicine 22E, 2025)
This is a shared conversation. Sign in to Orris to start your own chat.